Chapter 5 Arthrodesis of the Hip
Techniques
Arthrodesis with Cancellous Screw Fixation




Arthrodesis with Cobra Plate Fixation
 Place the patient supine with a sandbag under the ipsilateral buttock. Prepare and drape both lower extremities and anterior superior iliac spines to allow access to both iliac crests and both ankles.
Place the patient supine with a sandbag under the ipsilateral buttock. Prepare and drape both lower extremities and anterior superior iliac spines to allow access to both iliac crests and both ankles.
 Make a linear longitudinal midlateral incision along the femoral diaphysis to a point 8 cm distal to the tip of the greater trochanter (Fig. 5-1A).
Make a linear longitudinal midlateral incision along the femoral diaphysis to a point 8 cm distal to the tip of the greater trochanter (Fig. 5-1A).


 Identify the anterior and posterior margins of the gluteus medius.
Identify the anterior and posterior margins of the gluteus medius.
 Use an oscillating saw to make a greater trochanteric osteotomy so that the proximal fragment includes the insertion of the gluteus medius and minimus (Fig. 5-1B).
Use an oscillating saw to make a greater trochanteric osteotomy so that the proximal fragment includes the insertion of the gluteus medius and minimus (Fig. 5-1B).
 Elevate the hip abductors with the greater trochanteric fragment, and hold them superiorly with two large Steinmann pins hammered into the iliac wing (Fig. 5-1C).
Elevate the hip abductors with the greater trochanteric fragment, and hold them superiorly with two large Steinmann pins hammered into the iliac wing (Fig. 5-1C).
 Perform a superior hip capsulotomy.
Perform a superior hip capsulotomy.



 Remove a corresponding 0.5-cm wafer of bone from the superior pole of the femoral head.
Remove a corresponding 0.5-cm wafer of bone from the superior pole of the femoral head.






 Test hip flexion with the Thomas test.
Test hip flexion with the Thomas test.
 Distal to the plate, attach an AO tensioner to the lateral femoral cortex with a single unicortical 4.5-mm cortical screw (Fig. 5-1D).
Distal to the plate, attach an AO tensioner to the lateral femoral cortex with a single unicortical 4.5-mm cortical screw (Fig. 5-1D).





 Reattach the greater trochanter with a 4.5-mm cortical screw and washer (Fig. 5-1E and F). A trochanteric grip plate with wires may provide superior fixation if necessary.
Reattach the greater trochanter with a 4.5-mm cortical screw and washer (Fig. 5-1E and F). A trochanteric grip plate with wires may provide superior fixation if necessary.
 Pack any remaining corticocancellous bone around the hip joint, and obtain an anteroposterior pelvic radiograph to check the position of the plate, screws, and hip joint (Fig. 5-1G).
Pack any remaining corticocancellous bone around the hip joint, and obtain an anteroposterior pelvic radiograph to check the position of the plate, screws, and hip joint (Fig. 5-1G).
 Thoroughly irrigate the wound, and close the soft tissue in layers over drains.
Thoroughly irrigate the wound, and close the soft tissue in layers over drains.

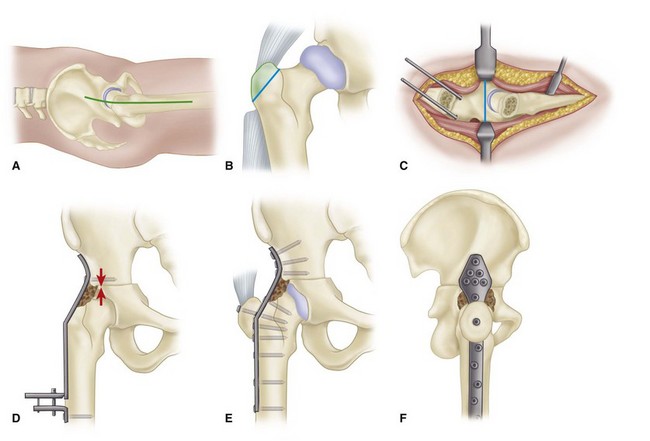
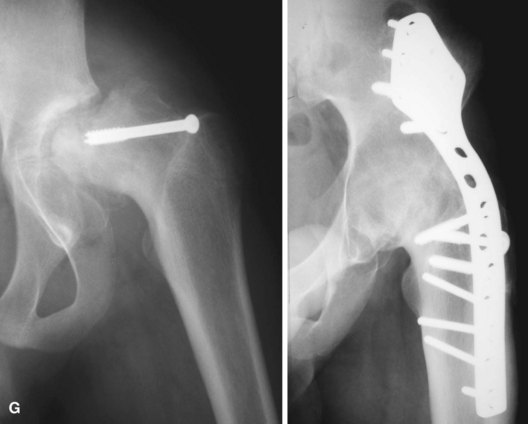
Figure 5-1 Hip arthrodesis with cobra plate fixation (see text). A, Longitudinal midlateral incision. B, Osteotomy of greater trochanter. C, Transverse innominate osteotomy. D, Cobra plate contoured and attached with two screws for application of compression force. E, Final fixation of plate. F, Lateral view of plate and reattachment of greater trochanter. G, Hip fusion with cobra plate. SEE TECHNIQUE 5-2.
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


