ROBERT A. CHRISTMAN AND JACQUELINE TRUONG
The number of variations in the adult foot may appear overwhelming, but at least they are of one developmental age group, that is, mature. In contrast, consider all the variations that might occur at all different developmental stages. And the radiographic appearance of one child’s foot at 5 years of age may be considerably different from another child’s at the same chronologic age. Fortunately, the variants of development are not that numerous and are primarily seen during the earlier stages of development; the reader should, however, refer to Chapter 7 for the varying radiographic presentations seen during skeletal development.
Developmental variants may easily be mistaken for pathology. The more frequent variants are multiple primary or secondary ossification centers, the presence of accessory ossification centers at sites other than the expected locations, and variants of form. A jagged metaphysis adjacent to the physis may suggest abnormality but is usually a normal variation. Accessory ossicles may be seen, but usually only later in skeletal development. Also, do not be surprised to see the initial appearance of an ossification center much earlier or even later than expected.
Confusion exists regarding the terms epiphysis and apophysis. An epiphysis is defined as “the expanded articular end of a long bone, developed from a secondary ossification center…”1 In contrast, an apophysis is “any outgrowth or swelling, especially a bony outgrowth that has never been entirely separated from the bone of which it forms a part, such as a process, tubercle, or tuberosity.”1

FIGURE 8-1. Multiple ossification centers, medial cuneiform, in a 5-year-old male.
MULTIPLE OSSIFICATION CENTERS
Both primary and secondary (epiphyseal/apophyseal) ossification centers can radiographically appear to ossify from multiple sites. These findings typically are asymptomatic and have been associated with a heterogeneous group of disorders known as the osteochondroses2 (see Chapter 17). Generally speaking, the radiographic picture of multiple centers of ossification is a variant of normal and occurs frequently.
It is rare to see the primary centers of tubular bones ossify from multiple areas, but the irregular bones of the midtarsus are often affected. The more commonly affected midtarsal bones are the medial cuneiform and navicular (Figures 8-1 and 8-2, respectively). Depending on the stage of development, appearance can vary considerably. The presence of multiple navicular ossification centers alone is not diagnostic of the osteochondrosis known as Kohler disease even though they both may appear flattened and asymmetric when first ossified.3 In fact, in most cases, radiographs of these same patients years later show normal ossification although the contour of the adult bone may be altered (Figure 8-3).4

FIGURE 8-2. Multiple ossification centers, navicular, in a 7-year-old male (medial oblique view).
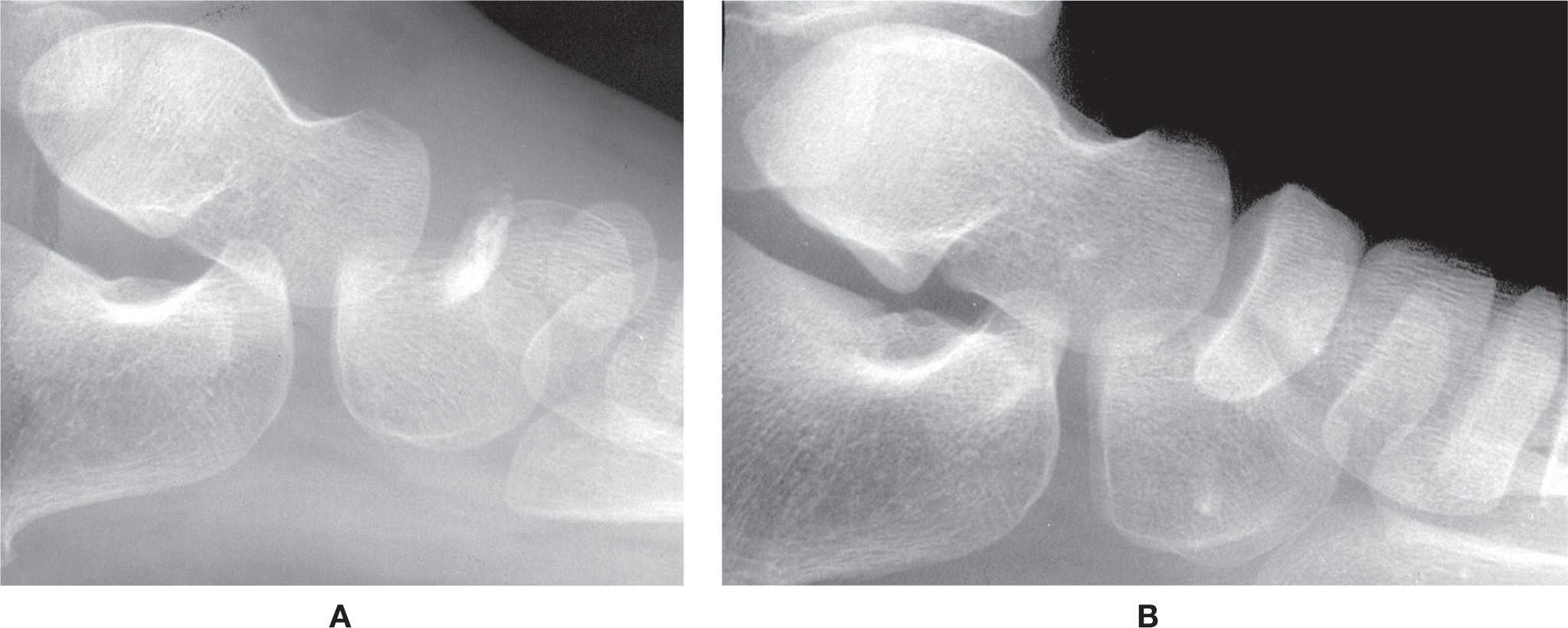
FIGURE 8-3. Variant navicular ossification can easily be misdiagnosed as Kohler disease. A: Sclerotic fragmented appearance at 4 years of age (asymptomatic). B: Normal navicular ossification at 8 years of age in the same patient.
Rarely, the calcaneus may appear to ossify from two centers (Figure 8-4); this has been called the bifid calcaneus, calcaneus bipartitus, and duplicate calcaneus.5–7 Characteristically, the calcaneus in this situation develops from a larger posterior and smaller anterior segment.8 It was first described by Sever9 in 1930. Cormier-Daire et al.10 believe that the duplicate calcaneus may reflect a more generalized developmental defect.
The persistence of two separate primary ossification centers into adulthood is known as a bipartition. The precursor to bipartition may be seen in the developing skeleton; it affects the first metatarsophalangeal sesamoids, albeit later in development,11 and rarely the medial cuneiform, navicular, and talus12,13 bones.
Secondary ossification centers (epiphyses and apophyses) frequently appear to ossify from multiple sites14 and are most evident in the metatarsals and calcaneus. Other sites affected include the hallux proximal phalanx basal epiphysis and the distal tibial epiphysis (Figure 8-5). Partitioning of the basal and apophyseal secondary ossification centers, in particular, may be mistaken for fracture. In general, multiple secondary ossification centers seem always to coalesce into one center, although the entire center may remain separate from its adjacent primary ossification center.
A metatarsal epiphysis may ossify from two, sometimes three centers (Figure 8-6). However, not all metatarsal epiphyseal centers need to be partite in the same foot or even bilaterally. Furthermore, their size and shape may not be symmetric.
Segmentation of the hallux proximal phalanx epiphysis is known as a bipartite basal epiphysis and can easily mimic a fracture (Figure 8-7). Typically, the bipartition is off center, the medial segment being the larger of the two. It may or may not present bilaterally.
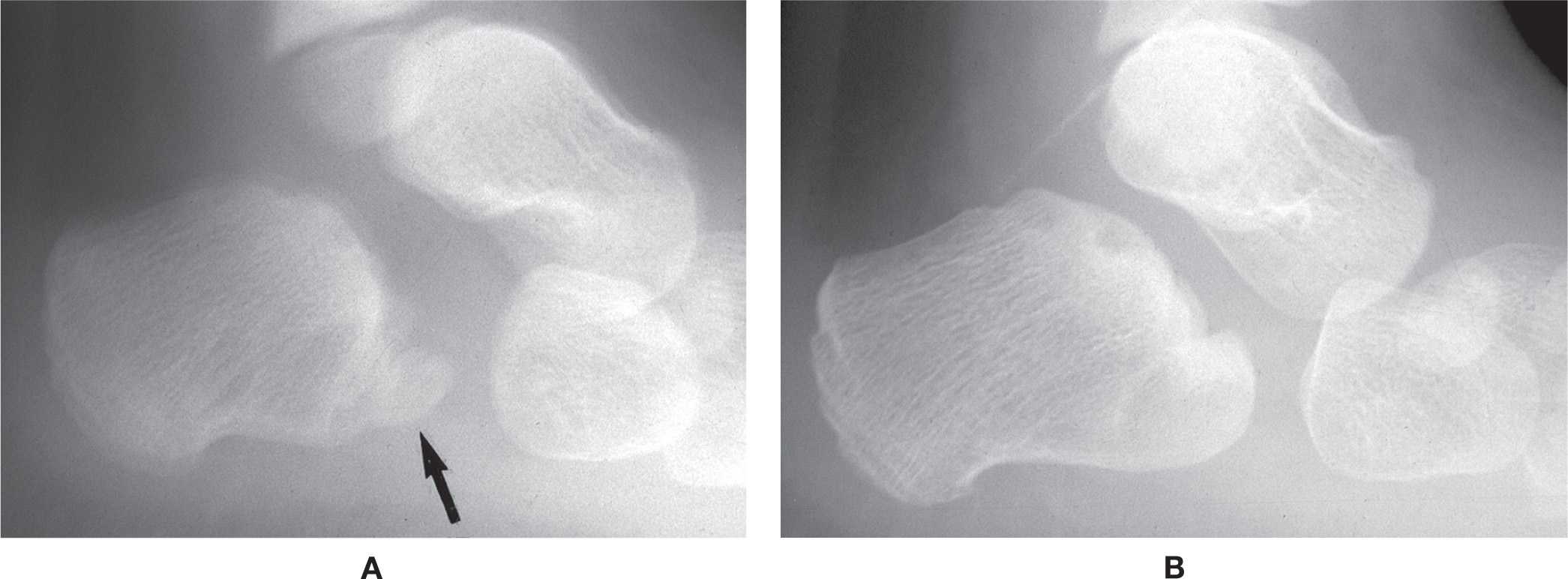
FIGURE 8-4. Multiple ossification centers, calcaneus. A: Smaller, separate ossification center anteriorly (arrow). B: One year later, the two ossification centers are united.

FIGURE 8-5. Segmentation (bipartition, arrow) of the distal tibial epiphysis, lateral view (a bilateral finding).

FIGURE 8-6. Multiple ossification centers, metatarsals. A: Bipartite first, second, and third metatarsals (5-year-old male). B: Bipartite fifth metatarsal tuberosity epiphysis.

FIGURE 8-7. Bipartite basal epiphysis, hallux proximal phalanx (a unilateral finding in this patient).
The calcaneal apophysis characteristically appears with multiple ossification centers radiographically (Figure 8-8). These centers are often irregular in outline and easily mimic fracture (“Sever disease”). However, this apparent “fragmentation” of the apophysis is entirely normal—often appearing to be more sclerotic than the rest of the bone and irregular.3 At first ossification begins posteroinferiorly; later ossification extends inferiorly to include the tuberosities and superiorly the bursal projection. At times an ossification center for the lateral tuberosity may be very large and suggests the development of an os subcalcis (Figure 8-9).
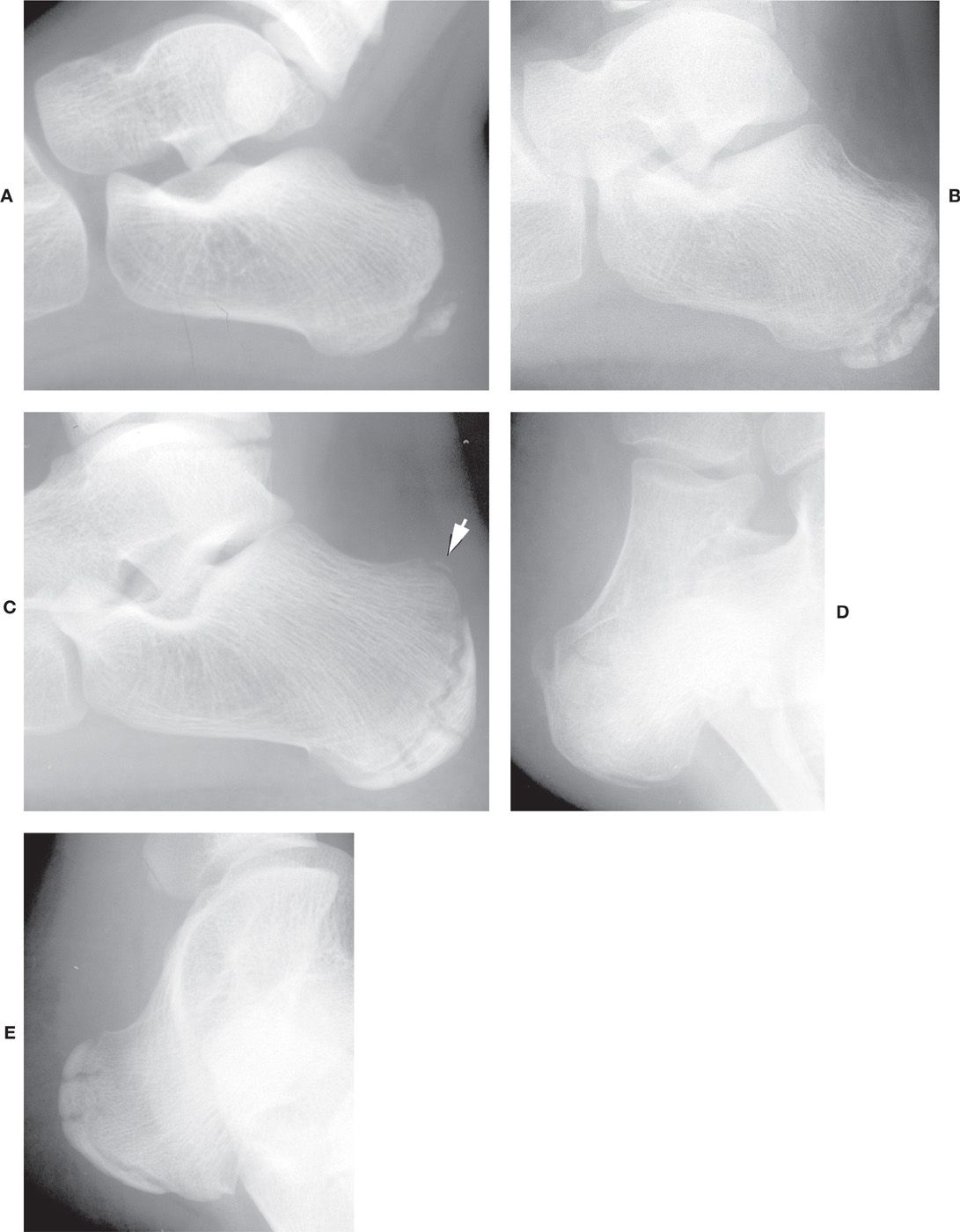
FIGURE 8-8. Multiple ossification centers, calcaneal epiphysis. A: Five-year-old female. B: Note the irregular appearance of the adjacent metaphysis. C: Twelve-year-old male. Note the separate ossification of the bursal projection (posterosuperior aspect, arrow) mimicking a fracture. D: Nine-year-old female. Medial oblique view demonstrating ossification of lateral tuberosity. Multiple ossification centers, calcaneal apophysis. E: Thirteen-year-old male. Lateral oblique view demonstrating ossification of medial tuberosity.

FIGURE 8-9. Separate, large ossification center for the lateral tuberosity in a 14-year-old male (medial oblique view). This center eventually united with the parent bone 2 years later.
The fifth metatarsal tuberosity apophysis appears between 6 and 15 years of age as a thin and fragile shell-like bone lateral to the base of the fifth metatarsal (Figure 8-10A).3 Irregular segmentation of this apophysis is frequent (Figure 8-10B) and commonly misinterpreted as fracture.
PSEUDOEPIPHYSES
Secondary ossification centers may appear to present at locations in addition to the normally expected epiphyseal sites. Typical sites in the foot include the head of the first metatarsal and the bases of the second through fourth metatarsals.15 The terms pseudoepiphysis and supernumerary epiphysis have been used to describe these variants in the forefoot. Lachman16 differentiates between the two types radiographically as follows: Pseudoepiphysis refers to “those epiphyses that show a bony bridge connecting them with the shaft,” and supernumerary epiphysis presents as a “truly independent center.” However, these two types more likely represent the same entity at varying stages of development. Furthermore, discrepancy exists regarding the histology of this enigma. Ogden et al.17 have demonstrated that this is not a true epiphysis but an extension of the metaphysis (hence, pseudoepiphysis). In contrast, Vilaseca and Ribes18 claim that it histologically and anatomically resembles all other physes. Another study has shown that this entity is actually quite common.19

FIGURE 8-10. A: Early ossification of the fifth metatarsal apophysis (arrow). B: Irregular, multiple ossification centers for the fifth metatarsal tuberosity epiphysis.
Radiographically, the first metatarsal pseudoepiphysis appears to develop similar to other secondary ossification centers; however, as ossification increases, superimposition and early closure of the physis give the appearance of incomplete development (Figure 8-11). Hypertrophy of the adjacent distal metaphysis may be noticed laterally and superiorly (Figure 8-12).
Pseudoepiphyses may also be seen along the bases of the second, third, and fourth metatarsals. Initially the developing bases appear irregular; separate ossification centers may or may not be easily visualized, again depending on the amount of superimposition and the stage of development (Figure 8-13).
ACCESSORY OSSIFICATION CENTERS
An ossification center may be seen for any of the accessory ossicles mentioned in Chapter 6. Typically, such centers appear during the later stages of development. Examples include the accessory sesamoid, os intermetatarseum, and os supranaviculare.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


