ROBERT A. CHRISTMAN AND JACQUELINE TRUONG
The radiographic presentation, or ossification, of the pediatric foot and ankle varies considerably from patient to patient. It depends on the age and sex of the individual, and variation is frequently encountered. Ossification center time of appearance can vary not only between individuals but also within the same individual with respect to bones in the same extremity. The normal expected learning curve, therefore, is much longer than that for radiographic anatomy of the adult foot and ankle, especially since one sees far fewer pediatric radiographic studies than the adult.
Evaluation of the pediatric skeleton requires observation of all the following:
1. Presence of the ossification centers
2. Orderly appearance of the ossification centers
3. Form (size and shape) of visible ossification centers
4. Relationships of one ossification center to another
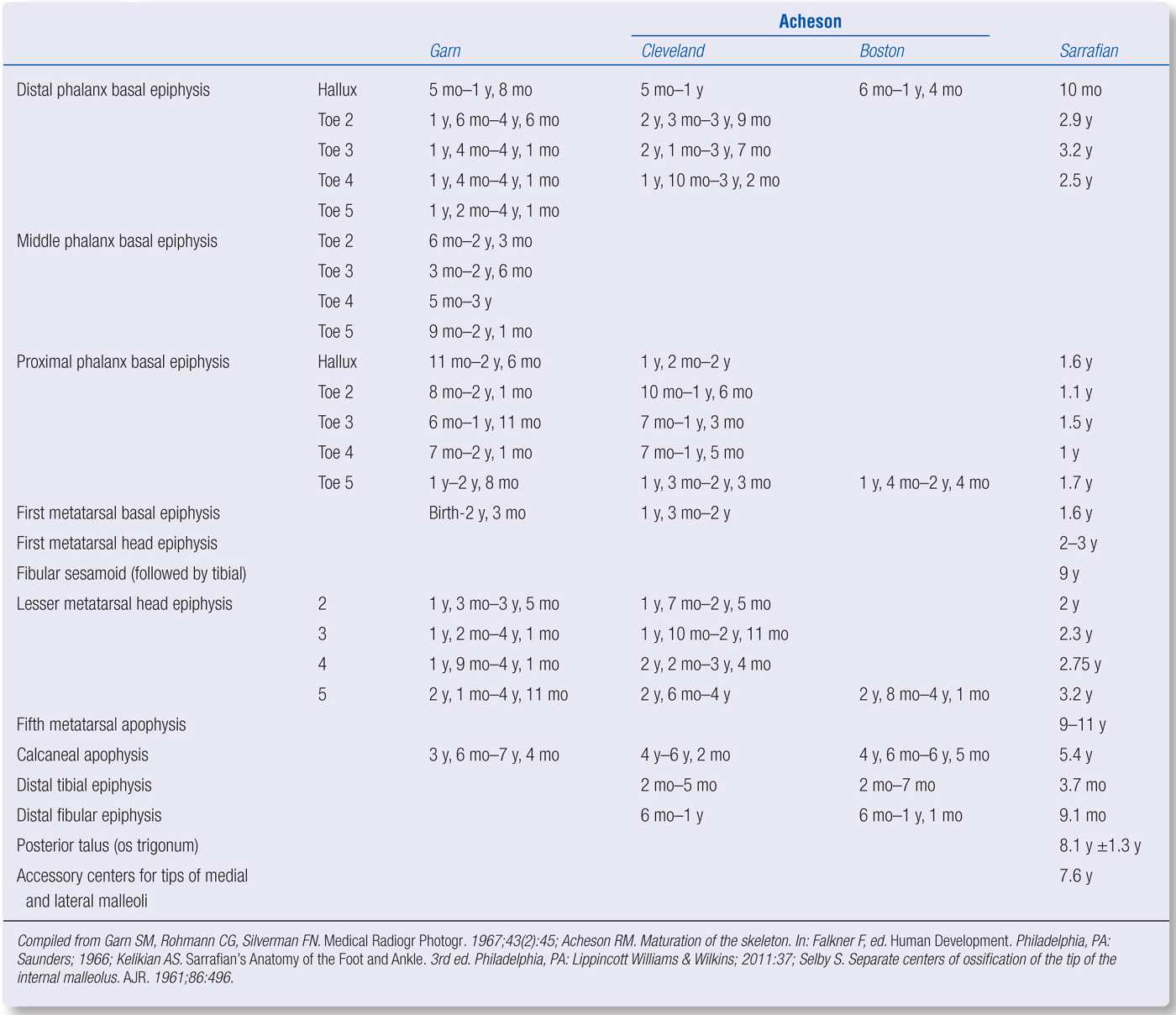
Several authors have listed the time of appearance of primary and secondary ossification centers; Tables 7-1 through 7-4 summarize many of them.1–3 In some instances, you can see a range of appearance time, and these times may vary among authors. The appearance time of ossification centers is earlier for females than for males. The sequence of fetal (primary) foot bone ossification centers is listed in Box 7-1.4 The time in which these primary centers completely ossify is listed in Table 7-5. Some accessory ossification centers have also been included: the os trigonum, and the tips of the medial and lateral malleoli. Sarrafian also lists a secondary ossification center for the posterior border of the talus that unites with the talus at 12.9 ± 1.3 years (male) and 9.8 ± 1.3 years (female); it appears the same time as the os trigonum ossification center.3
| Time of Appearance of Primary Ossification Centers: Male |
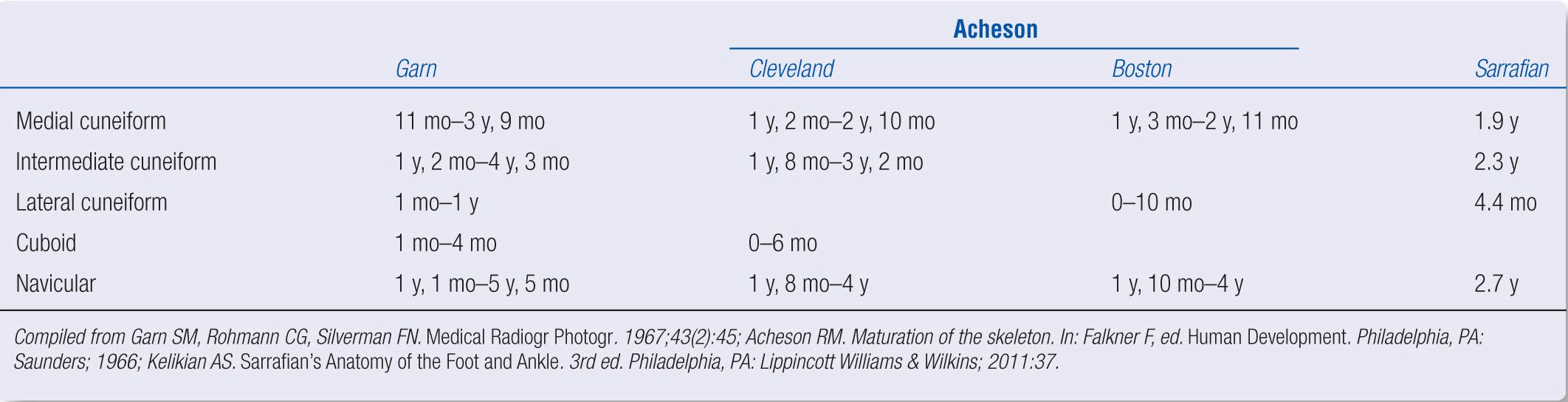
TABLE 7-2 |
| Time of Appearance of Primary Ossification Centers: Female |
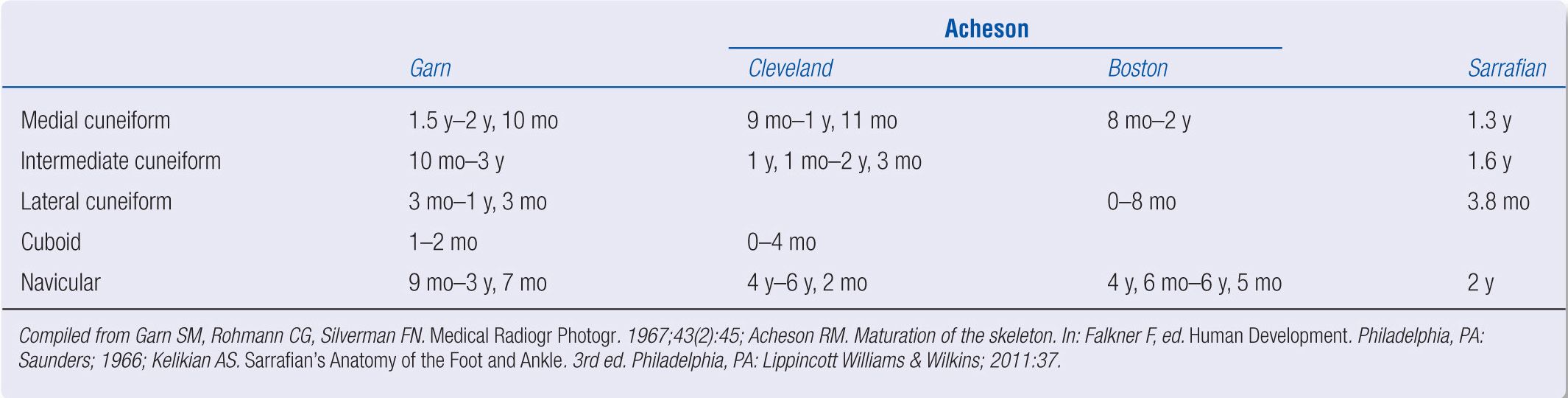
TABLE 7-3 |
| Time of Appearance of Secondary Ossification Centers: Male |
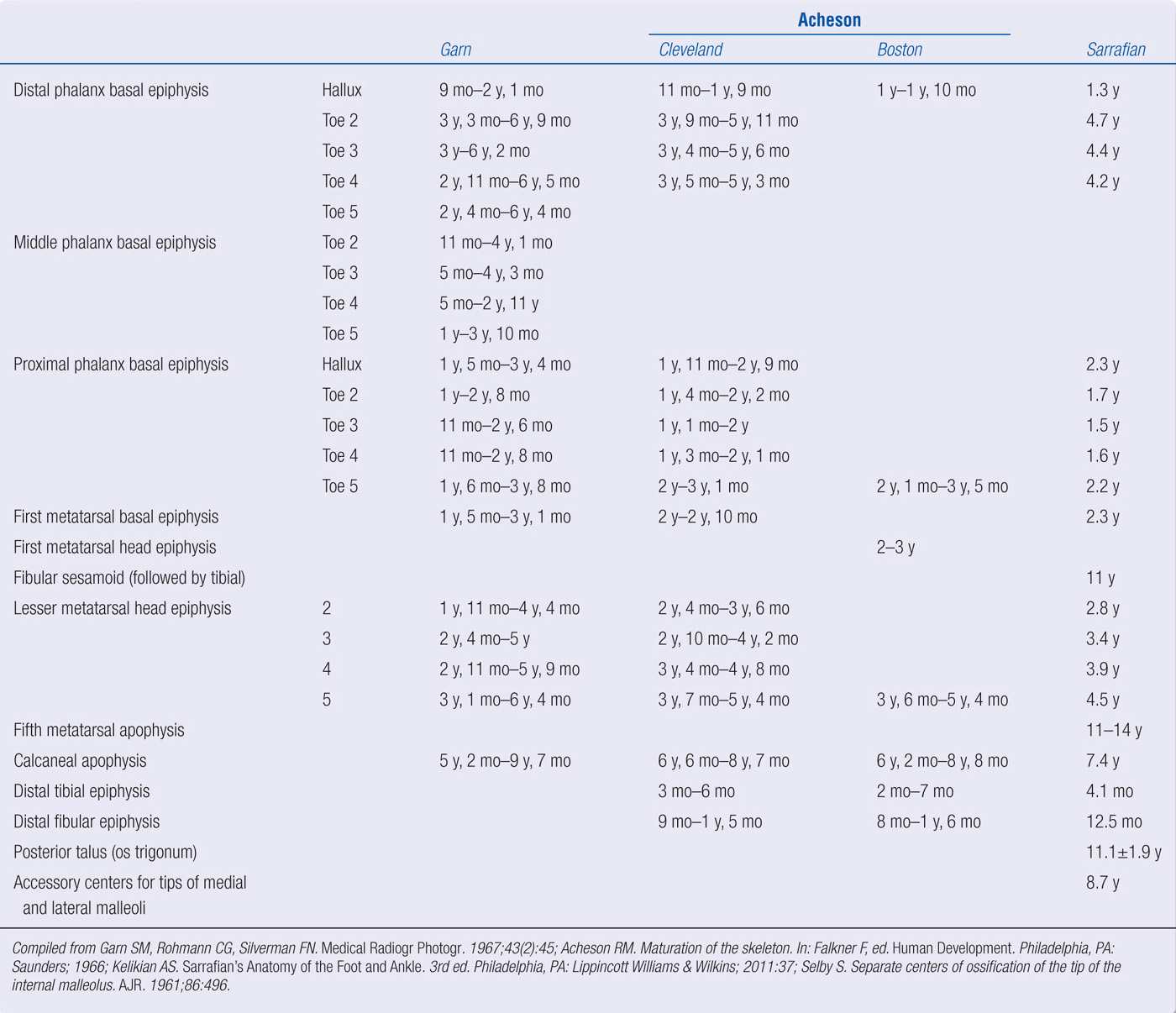
A complete description of the developing foot’s radiographic anatomy at different ages is nearly impracticable as the range of ossification varies considerably within individual children and between children of the same age, as shown in Tables 7-1 through 7-4. Instead, composite radiographs based primarily on the orderly appearance of primary and secondary ossification centers, after reviewing numerous sets of children radiographs at varying stages of development, are illustrated in Figures 7-1 through 7-19. These examples adhere to the skeletal maturity indicators described by Hoerr et al.5
| Time of Appearance of Secondary Ossification Centers: Female |
BOX 7-1 Sequence of Ossification of Fetal Foot
Sequence
1st Hallux distal phalanx and second, third, and fourth metatarsals
2nd Second through fifth toe distal phalanges and the first and fifth metatarsals
3rd Hallux and second toe proximal phalanges
4th Second, third, and fourth toe proximal phalanges
5th Second, third, and fourth toe middle phalanges
6th Fifth toe middle phalanx
7th Calcaneus
8th Talus
9th Cuboid
Compiled from Arey LB. Developmental Anatomy. 7th ed. Philadelphia, PA; Saunders; 1965:104.
| Completion of Ossification |
| Male (y) | Female (y) |
Hallux distal phalanx basal epiphysis | 13.6–16 | 11.3–13.4 |
Fifth toe proximal phalanx basal epiphysis | 14.7–16.7 | 12.9–15.1 |
Fifth metatarsal head epiphysis | 14.8–16.7 | 13–15.3 |
Medial cuneiform | 13.8–15.6 | 11.2–13.3 |
Lateral cuneiform | 13.8–15.6 | 11–13.5 |
Navicular | 13.8–15.6 | 11.1–13.3 |
Calcaneal apophysis | 14.5–16.6 | 12.8–15.2 |
Distal tibial epiphysis | 15.3–17.2 | 13.8–15.9 |
Distal fibular epiphysis | 15.4–17.4 | 14–16.2 |
Compiled from Acheson RM. Maturation of the skeleton. In: Falkner F, ed. Human Development. Philadelphia, PA: Saunders; 1966. | ||
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


