Introduction
The trunk is the central axis of the body. The limbs use the trunk as the base on which to move. When the body is upright, the trunk supports the head and maintains the erect posture with minimal effort.
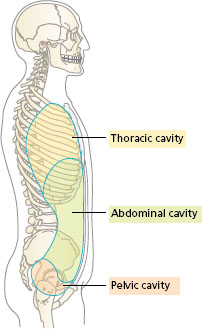
The trunk consists of the thorax, abdomen and pelvis, stacked one above the other (Figure 10.1). These three areas form two enclosed cavities, with bony and muscular walls, separated by the muscular diaphragm. Any change in the pressure inside one of the cavities affects the other. The vertebral column links the two cavities posteriorly.
- The thoracic cavity extends from the clavicle and first rib above to the muscular diaphragm below. Its walls are formed by the thoracic vertebrae, the ribs and the intercostal muscles in between.
- The abdominopelvic cavity has the dome of the diaphragm as the roof and the muscular pelvic floor below. The posterior wall contains the lumbar vertebrae, with muscle on either side of it. The anterolateral wall is formed by the abdominal muscles. The blade of the iliac bone of the pelvis lies in the abdomen. The pelvic part of the cavity is a bowl formed by the sacrum and the two innominate bones, with a muscular floor.
The joints and muscles of the trunk combine to form a stable system when standing upright. The muscles act like guy-ropes keeping the balance when external forces act on the trunk. If a group of muscles becomes weak, the trunk changes its position, in the same way that a tent will lean to one side if a guy -rope is loosened.
Figure 10.1 Side view of the trunk: outlines of the thoracic and abdominopelvic cavities.
The trunk has a protective function for the lungs, heart, digestive tract, kidneys and pelvic organs (bladder, rectum and reproductive organs). The spinal cord is also protected by being enclosed by the bones of the vertebral column, with pairs of spinal nerves emerging between adjacent vertebrae to be distributed to all parts of the body.
Ventilation of the lungs is the result of changes in the size of the thoracic cavity. Breathing also involves the anterior abdominal wall. Increased abdominal pressure pushes the diaphragm upwards and expels air from the lungs. Changes in the pressure in the abdominopelvic cavity are used to expel urine or faeces and in childbirth.
Lifting, carrying, pushing and pulling heavy loads all involve the trunk. The muscles of the trunk counteract the forces on the limbs, and adjust the line of gravity over the foot base. Carrying a heavy load of shopping in one hand requires muscle activity on the opposite side of the trunk to balance the weight. Increase in pressure in the abdominopelvic cavity, by tensing the anterior abdominal muscles, reduces the stress on the back in lifting loads from the front.
In summary, the trunk:
- maintains the upright posture;
- protects the organs of the thorax, abdomen and pelvis;
- ventilates the lungs in breathing;
- expels urine, faeces, and also the baby at birth;
- adapts to changes in the line of gravity as the body moves;
- releases pressure on the spine when lifting loads.
Most of the movements of the trunk are performed by large muscles arranged in sheets around the axial skeleton. The position of the muscles and direction of the fibres determine the ways in which each contributes to trunk movement.
Upright posture
The bones and ligaments of the vertebral column form a stable balanced support that requires little muscle activity when standing still. Any slight sway is counteracted by the tension in the strong longitudinal ligaments joining the individual vertebrae.
The vertebral column contains 33 bony segments. An individual vertebra articulates with the one above and the one below by a cartilaginous joint (intervertebral disc) between the bodies, and by four synovial joints between the articular processes. The position of the articular processes in a thoracic vertebra is shown in Appendix I.
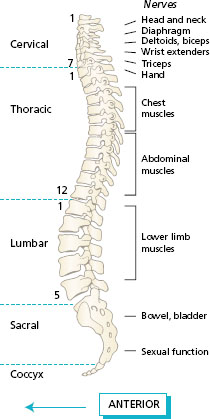
At birth, the vertebral column has a primary curve, concave forwards. As the baby learns to support the weight of the head and trunk in sitting and then standing, two secondary curves develop in the neck and lower back. From 2 years onwards, the vertebral column has four curves as follows: seven cervical vertebrae, convex forwards, secondary; 12 thoracic vertebrae, concave forwards, primary; five lumbar vertebrae, convex forwards, secondary; five sacral vertebrae (fused), concave forwards, primary; and three coccygeal vertebrae.
The four curves provide an efficient way of combining support with flexibility and resilience (Figure 10.2).
Figure 10.2 Side view of the vertebral column: cervical, thoracic, lumbar and sacral curves.
- Observe a partner standing upright. Look first from the side to imagine a line from the ear through the vertebral column to the hip and knee, ending just in front of the ankle. Move the trunk until the position looks balanced. Notice the curves of the back. Refer to an articulated skeleton to see the curves more easily. Next, look at your partner from the front to see whether the shoulders and hips are level, i.e. no lateral curves.
- Watch a person sitting at a keyboard and notice the shape of the back in relation to the shape of the back of the chair. Try raising and lowering the keyboard to see the effect on the working posture.
- Look at elderly people sitting in easy chairs. Think where a cushion should be placed to support the lumbar curve of the back.
If an abnormal posture is adopted over long periods, the normal relaxed position is progressively lost and muscle activity must be used to a greater extent. Examples of abnormal posture are: kyphosis, standing with rounded shoulders; lordosis, standing with a hollow back; and scoliosis, lateral curvature to the spine, and tilting of the shoulders.
Shoes with high heels throw the body weight forwards and the vertebral column adapts by increasing the lumbar curvature (lordosis). Problems with breathing may develop in scoliosis owing to the effect on the shape of the thorax. Poor working posture increases the possibility of lower back pain, even in the young. In the elderly, degenerative changes in the vertebrae and discs due to disease or ageing, coupled with the loss of the need and motivation to move about during the day, give general loss of mobility, and deformity develops which may become permanent.
Joints and movements of the vertebral column
When the trunk moves in different directions, the movement between adjacent vertebrae is small, but the result of combined movement of vertebrae at all levels results in a considerable range of movement.
Joints of the vertebral column
There are two series of joints between adjacent vertebrae in the column: anterior and posterior.
The anterior joints are between the bodies of the vertebrae: these articulations are secondary cartilaginous joints, the intervertebral discs. They increase in thickness from the upper cervical vertebrae down to the lumbar vertebrae. In the fibrocartilaginous discs, which form about a quarter of the total length of the vertebral column, the collagen fibres are arranged in concentric layers, the annulus fibrosus. The semifluid central mass of the disc is the nucleus pulposus. During movements of the trunk, the cartilaginous discs are compressed on one side (see Chapter 1, Figure 1.6b).
The posterior joints are between the articular processes on the vertebral arch of bone which surrounds the spinal cord: these are synovial plane joints. A thin capsule surrounds the adjacent articular surfaces and allows gliding movements between adjacent vertebrae.
All of the vertebrae are joined together by anterior and posterior longitudinal ligaments that extend along the whole length of the vertebral column joining the respective surfaces of the vertebral bodies. Other ligaments join all of the spines and transverse processes of the vertebrae.
Figure 10.3 Movements of the trunk: (a) flexion (forwards) and extension (backwards); (b) lateral flexion; (c) rotation; (d) circumduction.
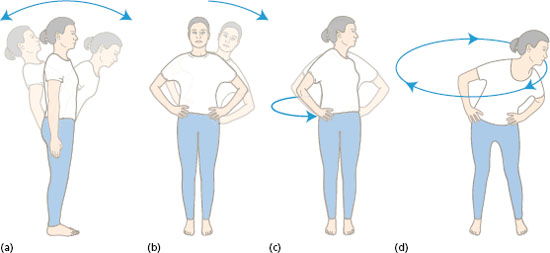
The movements of the trunk, shown in Figure 10.3, are described as follows:
- Flexion occurs in bending forwards, or sitting up from lying. The thorax moves towards the pelvis.
- Extension straightens the trunk from flexion and the trunk can bend backwards from the upright position. The thorax moves away from the pelvis.
- Lateral flexion bends the trunk to the side. The ribs move towards the pelvis on one side only.
- Rotation twists the trunk to the right or the left. The head and shoulders are turned so that the eyes can look to the side or behind, either to the right or left.
The trunk -rolling exercise shown in Figure 10.3d is a combination of all of these movements.
The range of the individual movements varies in different parts of the vertebral column, depending on the thickness of the intervertebral discs, the direction of the articular facets of the synovial joints, and the length and angulation of the spines. The regions with secondary curves have the greatest mobility. Movements of the cervical region are important for the eyes to scan a large area. Reversing a car becomes difficult when there is loss of mobility in the neck. The lumbar region has the greatest range for flexion and extension movements. The extreme bending movements of the acrobat and gymnast are achieved by continual exercises to stretch the intervertebral ligaments and increase the separation of the lumbar vertebrae. Conversely, the fusion of the lumbar vertebrae in some pathological changes of the spine will reduce the overall mobility of the trunk by a significant amount.
Muscles moving the trunk
Two systems of muscles collectively perform all movements of the trunk: the deep posterior muscles of the back and the abdominal muscles.
Deep posterior muscles of the back
The posterior aspect of the vertebral column, from the sacrum to the skull, provides a long line of bony processes for the attachment of muscle fibres. Some of these muscles fibres are long, extending from the sacrum to the thorax, while others are short and only span one, two or three vertebrae. The vertical fibres pull the column into extension, those arranged obliquely can rotate one vertebra on the next, and the lateral fibres which are attached to the angles of the ribs can assist lateral flexion.
The largest muscle in this group of deep back muscles is the erector spinae (also known as the sacrospinalis), which originates from the sacrum by a thick broad tendon. In the lumbar region, this muscle is thick and can be palpated in the lower back. Continuing upwards, the muscle is in three bands in the thoracic region, attached to the spines of the vertebrae, the transverse processes and the ribs. The uppermost fibres in the cervical region end on the base of the skull.
The muscles connecting the trunk to the upper limb, for example the latissimus dorsi and trapezius (described in Chapter 5), are separated from the deep muscles of the back by a layer of deep fascia.
Figure 10.4 follows the line of erector spinae on the right -hand side of the vertebral column. Note how the muscle starts at the sacrum and climbs up the back to the head. Deep to the erector spinae another group of muscles is found (Figure 10.4, left -hand side of the vertebral column). Most of the fibres in this deeper group lie obliquely from the transverse process of one vertebra to the spine of the vertebra above, or they may span three or four vertebrae. The parts found in the thorax and neck are known as semispinalis.
In movements of the trunk, the erector spinae acts strongly to raise the body from forward flexion to an upright position. The erector spinae counteracts both the tendency to sway forwards in standing and the force of loads carried in front of the body.
Figure 10.4 Erector spinae (right); semispinalis and quadratus lumborum (left), posterior view of the trunk.
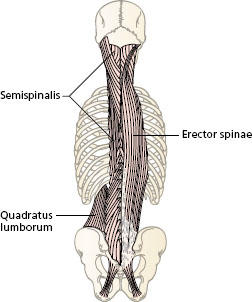
Figure 10.5 Lifting: (a) straight legs; (b) sitting; (c) knees bent. 1 = line of gravity, 2 = load arm; 3 = effort force.
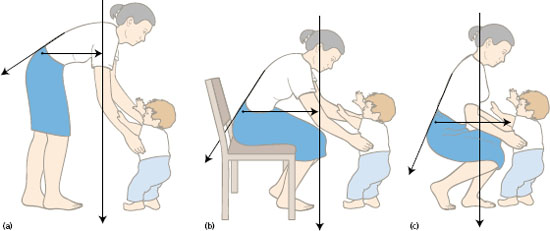
Lifting loads placed in front of the body may cause considerable stress on the lower back. In raising the trunk and the load, the pull of the erector spinae muscle compresses the lumbar intervertebral discs, which may prolapse (see Practice note-pad 10A). The aim of good lifting practice is to reduce the compression force on the lumbar discs. Figure 10.5 shows the application of the principle of levers (see Chapter 2) in three positions for lifting a child.
In lifting with straight legs, the starting position is forward flexion (Figure 10.5a). From this position, the line of weight of the trunk plus the child (1) is some distance from the fulcrum in the lower back, so that the load arm (2) is long. The erector spinae, acting on a short lever arm, must develop considerable effort force (3) to overcome the moment of force of the trunk.
In lifting from the sitting position (Figure 10.5b), the line of weight (1) is even further from the fulcrum and the load arm (2) is longer. The compression load on the discs is therefore much greater as the erector spinae extends the spine. People in wheelchairs should avoid lifting heavy loads, since the stress on the back will be greater than the same load lifted by someone who can stand close to the load.
In lifting with the knees bent and with the load as close to the body as possible, the line of weight (1) is moved nearer to the body, and the load arm of the trunk plus the child (2) is short. This means that the effort force (3) exerted by erector spinae to counteract the load is reduced. In addition, it allows the extensors of the hip and the knee to contribute most of the effort force for the lift. This explains how bending the knees and keeping the trunk as upright as possible puts less stress on the back in lifting.
Anterior abdominal wall
The anterior abdominal wall consists of flat sheets of muscle forming a four -way corset or girdle between the ribs and the pelvis. The position of the individual muscles is as follows. The rectus abdominis lies down the centre of the abdomen, one on either side of the midline. The muscle fibres are in the vertical direction. The external and internal oblique abdominal muscles are two sheets of muscle around the anterior and lateral walls of the abdomen. The muscle fibres are arranged diagonally. The transversus abdominis is a muscle lying deep to the obliques which has horizontal fibres forming a band wrapping round the abdomen.
Figure 10.6a shows the direction of the fibres of the abdominal muscles seen from the side. The fibres of the two oblique muscles and transversus abdominis blend into an aponeurosis (dense fibrous tissue) towards the midline, connecting with those from the opposite side to form a sheath around the rectus abdominis.
The rectus abdominis (Figure 10.6b) is a strap -like muscle extending from the lower end of the sternum and the costal cartilages of the fifth, sixth and seventh ribs to the pubis below. The muscle fibres are usually interrupted at three intervals by transverse bands of fibrous tissue, known as tendinous intersections. The four bulges of muscle fibres in between can be seen clearly in men who have done weight training. The rectus abdominis flexes the trunk by pulling the sternum towards the pelvis, so acting strongly in sitting up from lying. When the body is lifted off the ground, as in running and jumping, the rectus abdominis supports the front of the pelvis.
The external oblique abdominal muscle is attached to the outer surfaces of the lower eight ribs. The posterior fibres pass vertically to insert on the anterior part of the iliac crest of the pelvis. All of the other fibres lie in a direction downwards and forwards, i.e. like hands in a side -pocket, to attach to the wide central aponeurosis (Figure 10.6c). The lower margin of the muscle and aponeurosis is thickened to form the inguinal ligament, which extends from the anterior superior iliac spine to the pubic crest (see Chapter 8, Figure 8.10). The inguinal ligament acts as a retinaculum forming the division between the trunk and the thigh.
The internal oblique abdominal muscle is attached to the fascia of the lower back (thoracolumbar fascia), the anterior iliac crest (deep to the external oblique) and the inguinal ligament. The muscle fibres pass upwards and inwards, to attach to the lower ribs, and become a wide aponeurosis as far as the midline (Figure 10.6d). The aponeuroses of the right and left obliques meet in the midline at the linea alba, a strip of fascia from the lower end of the sternum to the pubic symphysis.
The muscle fibres of the two oblique abdominal muscles lie at right angles to each other. The ways in which the two layers of oblique abdominal muscles work in combination to produce movements of the trunk will now be considered.
- Flexion of the trunk involves the external and internal obliques on both sides together.
- Lateral flexion involves the external and internal oblique on one side only.
- Rotation of the trunk involves the external oblique on one side working with the internal oblique on the opposite side. The trunk then rotates towards the side of the internal oblique (Figure 10.6e).
In standing and sitting, the oblique abdominals work with the neck muscles in turning to look to the side and behind. In walking, the pelvis is carried forwards on the side of the leading leg and the trunk rotates to keep the eyes looking forwards.
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


