Introduction
The forearm and wrist provide the base for the fine skilled movements of the fingers and thumb. Objects and tools must be held in a particular orientation for their functional use. A cup full of coffee will soon be spilled if it cannot be held upright. This depends not only on the grip of the fingers and thumb on the handle of the cup but also on the position of the forearm and the stability of the wrist. The hand must also be orientated accurately on to surfaces when the hand explores the environment.
Many manipulative tasks involve the bilateral activity of the two hands working together. The two hands may be performing similar movements, as in rolling pastry or pressing the keys of a computer keyboard. At other times, one hand may provide stability while the other hand makes precise movements, for example in stirring the contents of a saucepan, unscrewing the top of a jar or sewing.
Fine movements of the fingers and thumb are performed by the intrinsic muscles of the hand. These muscles also depend on forearm muscles for their strength and for the fixation of their proximal attachments. Together, the forearm, wrist and hand form an interdependent system for the performance of manipulative movements.
Functions of the forearm and wrist
The forearm and wrist co-operate in the orientation of the hand in space.
The forearm:
- enables the hand to grip handles and hold objects in any orientation in the performance of functional activities;
- allows the hand to function as a tactile sense organ by contact with all surfaces.
The wrist:
- lifts the hand to a functional position by counteracting the effect of gravity tending to pull the hand into flexion or ulnar deviation;
- stabilises the relative positions of the hand and forearm during manipulative movements.
The combination of the movements of the forearm and the wrist means that the hand is joined to the arm by a virtual joint that moves in all axes.
The forearm
In the anatomical position, the radius and the ulna are parallel. When movement occurs in the forearm the radius rotates and crosses over the ulna. This movement of the radius carries the hand with it.
When the elbow is flexed, the radius and ulna are parallel, and the palm of the hand faces upwards. The movements of the forearm are:
- pronation: turns the hand to face downwards and the radius and ulna are crossed;
- supination: turns the hand to face upwards and the radius and ulna are parallel again.
The midprone position is when the hand faces inwards or medially. This is the functional position of the hand.
When pronation and supination are limited, for example after fractures of the forearm, there is considerable loss of hand function.
- Find handles and rails in different positions, i.e. vertical, horizontal, at an angle. Grip each one and notice how the position of the forearm changes in each position to allow the hand to grip.
- Grip the vertical handle of a teapot orjug and then tip to pour out the contents. Note how the grip remains the same while the tipping is done by pronation and supination of the forearm.
- Turn a tap or a round door-knob. The fingers and thumb exert pressure on the tap, while the forearm movement provides the power to turn it.
Radioulnar joints
The movements of pronation and supination occur at synovial pivot joints found at the proximal and distal ends of the radius and ulna. In between, the shafts of the two bones are held together by an interosseous membrane, a fibrous joint of the syndesmosis type (Figure 6.1a).
The superior (proximal) radioulnar joint lies between the head of the radius and the radial notch on the ulna. The joint lies inside the capsule of the elbow joint, but its movements are entirely independent. The radius is held in contact with the ulna by the annular ligament (lined by a thin layer of cartilage), which surrounds the head of the radius and is firmly attached to the margins of the radial notch on the ulna (Figure 6.1b). The capsule of the elbow joint blends with the annular ligament so that the radius can rotate independently within this ring whatever the angulation of the elbow joint may be.
The inferior (distal) radioulnar joint: the lower end of the radius pivots round the head of the ulna, and is held in contact with it by a disc of fibrocartilage. This disc joins the styloid process of the ulna to the ulnar notch of the radius (Figure 6.1c). The joint has a thin loose capsule, but the bones are held together by the articular disc and the interosseous membrane above.
All the muscles involved in pronation and supination are inserted into the radius, which then moves around the fixed ulna. The supinators, inserted into the radius, can also assist other muscles to move the elbow, e.g. the biceps brachii is also an elbow flexor, and the supinator helps in extension of the elbow.
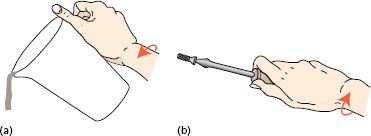
Pronation puts the palmof the hand flat on a surface, or tips forwards a vessel held in the hand (Figure 6.2a). Strong pronation and supination movements are needed to use a screwdriver or a corkscrew (Figure 6.2b).
Supination is more powerful than pronation, and so most screws have a right-handed thread.
The brachioradialis, already described with the elbow flexors in Chapter 5, can move the forearm to the midprone position from full pronation or full supination.
Muscles producing pronation and supination
Two forearm muscles are active in pronation: the pronator teres and pronator quadratus.
Figure 6.1 Right radioulnar joints: (a) middle, anterior view; (b) proximal; (c) distal.
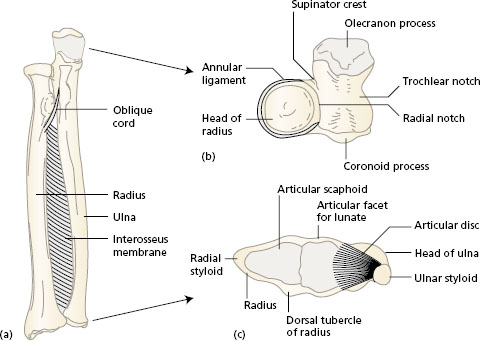
Figure 6.2 Activites involving pronation and supination: (a) pouring from a jug – pronation; (b) turning a screw – supination.
The pronator teres (Figure 6.3a), which crosses the anterior forearm from the medial side of the elbow to half way down the lateral shaft of the radius has already been described in Chapter 5, with the elbow flexors.
The pronator quadratus (Figure 6.3a) is a deep muscle of the forearm just above the wrist. Its fibres pass transversely between the lower anterior shafts of the radius and ulna. The muscle is deep to the flexor tendons which pass into the hand. When force is applied to the outstretched hand in pushing or falling, the pronator quadratus prevents separation of the radius and ulna. Many pronation movements are made with the pronator quadratus alone, the pronator teres being recruited for extra power against resistance.
Figure 6.3 Muscles and movements of (a) pronation and (b) supination. Right forearm and hand.
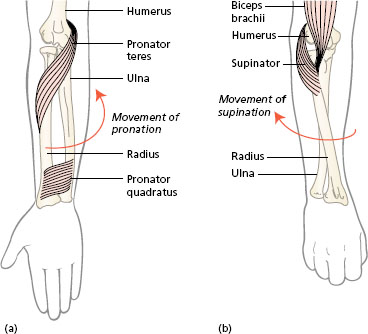
The two muscles active in supination are the biceps brachii and supinator.
The biceps brachii (Chapter 5, Figure 5.13) makes all supination movements against resistance. Its tendon pulls on the radial tuberosity just below the elbow to rotate the radius to the position parallel with the ulna. The attachments and action of biceps have already been described in Chapter 5 with the elbow flexors.
The supinator (Figure 6.3b) is a deep posterior muscle of the forearm which is involved in slow, unopposed movements of supination, such as when the arm hangs by the side. This muscle is covered by the long extensors of the wrist and fingers. The origin of the supinator is from the lateral epicondyle of the humerus and adjacent areas of the ulna. A short flat muscle, its fibres wrap round the proximal end of the radius close to the bone and insert into the upper end of the shaft.
The wrist
The wrist region is concerned with movements of the carpus of the hand on the distal ends of the radius and ulna of the forearm. The range of movement is increased by the movement of the carpal bones on each other, particularly between the proximal and distal rows.
Joints and movements of the wrist
The wrist joint is composed of the joints between the carpal bones (intercarpal joints) and the radiocarpal articulation between the forearm and the proximal row of carpals. The intercarpal joint between the two rows of carpals is known as the midcarpal joint. The main movement at the wrist occurs at the radiocarpal and midcarpal joints.
The radiocarpal joint is formed by the concave distal end of the radius and an articular disc over the ulna articulating with a reciprocally convex surface formed by the three carpal bones in the proximal row, i.e. scaphoid, lunate and triangular (triquetral). This joint is an ellipsoid type allowing movement in two directions (see Chapter 2, Figure 2.3c). The articular surface of the radius and ulna is shown in Figure 6.1c.
The midcarpal joint lies between the proximal and distal row of carpals, i.e. distal surfaces of the scaphoid, lunate and triquetral, with proximal surfaces of the trapezium, trapezoid, capitate and hamate. The joint cavity is continuous between the two rows of carpals and extends between the individual bones. (The fourth bone in the proximal row, the pisiform, does not take part in either of the joints.)
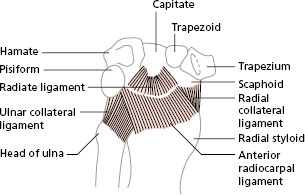
The capsule of the radiocarpal joint, strengthened by ligaments, extends to cover the midcarpal joint. Both joints are strengthened on each side by the ulnar and radial collateral ligaments (Figure 6.4).
The movements at the joints of the wrist are flexion, extension, abduction (radial deviation) and adduction (ulnar deviation).
Figure 6.4 Right wrist (radiocarpal) joint, anterior aspect.
There is no active rotation of the wrist about a longitudinal axis. Remember that rotation of the hand on the forearm occurs at the radioulnar joints of the forearm, i.e. pronation and supination movements.
Radiographs of the wrist in action show that all the carpals move as well as the radiocarpal articulation. In some movements, the scaphoid, for instance, may move as much as 1 cm. The radiocarpal joint contributes most to extension and adduction, while the midcarpal joint moves further in flexion and abduction. All the joints act together as a single mechanism for wrist movement.
- Place the supinated hand (palm upwards) on a flat surface in a relaxed position. Notice the slight flexion and deviation to the ulnar side.
- Look at an articulated skeleton to see the shape of the lower end of the radius extending further on the dorsal side and laterally at the styloid process, which accounts for the position of the hand.
- Lift the hand and move the wrist into flexion, extension, abduction (radial deviation) and adduction (ulnar deviation). Note the range of each of these movements. You will see that the hands move further in flexion than extension, and more easily in ulnar deviation than radial deviation.
- Compare your own range of these wrist movements with those of other people. Notice the difference in range between individuals, but the relative amounts for each movement are usually the same.
Since there is a variation in range of movement in normal subjects, the assessment of an injured wrist should be done by comparing it with the normal wrist of the same person and not with the ‘average’ wrist.
- Colles’ fracture when the lower broken ends of bone are displaced backwards; or
- Smith’s fracture when only the radius is fractured and the distal fragment displaces forwards.
A fall on the hand with the wrist in full extension may fracture the scaphoid. The scaphoid bone fractures across its waist, and the proximal fragment may die due to poor blood supply. This avascular necrosis may produce persistent pain and weakness of the wrist.
Muscles moving the wrist
The muscles arranged around the wrist combine in different ways to produce the movements of flexion, extension, abduction and adduction. If the wrist is viewed in cross-section, the flexor and extensor tendons involved in wrist movement can be seen around the oval shape of the carpus. The tendons pull on the carpus in different combinations, like the strings of a marionette, to produce all the movements of the wrist.
The two anterior muscles, active in flexion of the wrist, are the flexor carpi ulnaris and flexor carpi radialis. The palmaris longus is another wrist flexor that lies between the other two, but it is absent in 15% of people. All three muscles have a common origin on the medial epicondyle of the humerus, and form the superficial layer of muscles in the anterior forearm.
The flexor carpi ulnaris is attached to the pisiform bone and on to the base of the fifth metacarpal. The flexor carpi radialis lies deep to the muscles at the base of the thumb as it crosses the wrist and ends at the bases of metacarpals 2 and 3 (Figure 6.5a).
The palmaris longus has a long thin tendon that inserts into the palmar aponeurosis, a layer of dense fibrous tissue below the skin of the palm, considered in more detail later in the chapter.
Figure 6.5 Flexors of the wrist: (a) position in the superficial layer of the anterior right forearm; (b) combing the hair.
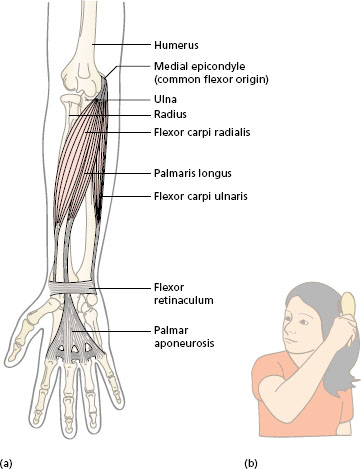
A functional use of the wrist flexors can be seen in Figure 6.5b, where they are used to counteract the resistance offered by the hair on the comb.
Three posterior muscles, active in extension of the wrist, are the extensor carpi ulnaris and the extensor carpi radialis longus and brevis (Figure 6.6a). The long radial extensor takes origin on the ridge above the lateral epicondyle of the humerus with brachioradialis, already described in Chapter 5. The other two muscles are attached to the lateral epicondyle which is the common extensor origin. All three muscles pass down the posterior side of the forearm and insert at the wrist following the same pattern as the flexors: extensor carpi radialis longus into metacarpal 2; extensor carpi radialis brevis into metacarpal 3; and extensor carpi ulnaris into metacarpal 5.
Figure 6.6 Extensors of the wrist: (a) position in the posterior right forearm; (b) hand held with extended wrist to use a keyboard.
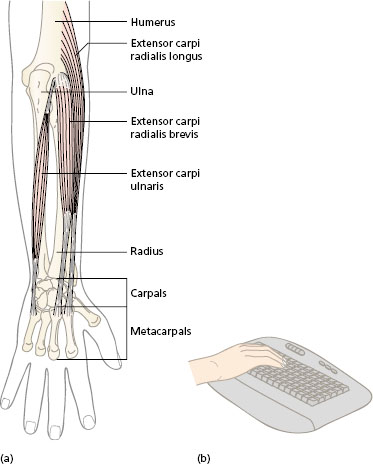
In the use of the pronated hand, e.g. pressing keys of a typewriter or piano (Figure 6.6b), the wrist extensors are active to lift the weight of the hand against gravity. Weakness of these muscles leads to ‘wrist drop’. In strong gripping by the whole hand, the wrist extensors act as synergists to counteract flexion of the wrist by the long finger flexors.
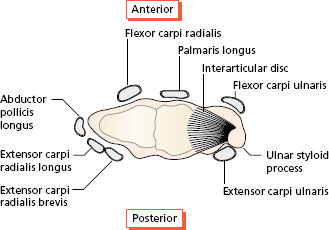
Abduction and adduction of the wrist is achieved by contraction of the flexor and extensor muscles on the radial and ulnar sides, respectively. See Figure 6.7 for the position of the tendons around the wrist. Contraction of the flexor carpi ulnaris and extensor carpi ulnaris muscles adducts the wrist, often known as ulnar deviation. Similarly, contraction of the flexor carpi radialis and extensor carpi radialis longus and brevis together will result in abduction of the wrist or radial deviation.
Figure 6.7 shows the positions of the tendons of the wrist flexors and extensors arranged around the wrist. Note that the flexors insert into the anterior or palmar side, and the extensors insert into the posterior or dorsal side. A strong and stable wrist in the midprone position of the forearm is used in operating many tools, for example a saw. When the muscles around the wrist are weak, the hand falls into ulnar deviation when holding the tool.
Figure 6.7 Position of the wrist flexors and extensors around the distal end of the radius and ulna, inferior view.
Functions of the hand
The hand performs fine movements of the fingers and thumb to operate small tools and keyboards. The intrinsic muscles of the hand combine to make the small movements of the fingers and the thumb required in skillful activites, for example writing, texting using a mobile phone, painting and playing musical instruments.
The hand is the mechanism to grasp handles and large tools while the upper limb moves them in space. In all gripping movements, the thumb is placed opposite to the fingers in different ways depending on the size and shape of the object. The wrist is important in gripping by providing a stable base for the hand, and by directing the pull of the tendons of the forearm muscles acting on the fingers and thumb. Grasping activites also involve release movements to let go or set down, using the opposing group of muscles to those that make the grip.
The hand is also a sense organ. The skin of the hand, particularly the palm and the fingertips, is richly supplied with receptors, and a large area of the somatosensory cortex in the brain (see Chapter 3) processes information from them. All gripping activities involve the continuous monitoring of activity in the tactile and pressure receptors in the hand. For example, in writing, accurate formation of the letters depends on the correct pressure of the fingers on a pen, and the hand on the paper. Response from receptors in the skin of the hand is important to protect it from injury. Trauma or pathological changes in the bones and joints of the wrist may damage sensory fibres in the nerves passing over them and affect hand sensation.
Further processing of all the sensory information in the brain allows us to ‘recognise’ objects held in the hand without seeing them. This is known as stereognosis (see Chapter 3).
Finally, the hand is used in communication and in the expression of emotion. Watch how people use their hands as they greet each other, or chat in a group. Hands are used to complement and reinforce the spoken word in a conscious way, or may be used unconsciously in ‘body language’.
In summary, the functions of the hand are:
- the performance of fine manipulative movements;
- to grasp and release objects and tools;
- asa sense organ for the exploration of the environment and recognition of objects;
- in the communication and expression of emotion.
Movements of the hand: fingers and thumb
The movements of the hand are performed by muscles that originate partly in the hand (intrinsic muscles) and partly in the forearm (extrinsic muscles), passing over the wrist into the hand. The hand performs complex and precision movements in the manipulation of utensils, tools and equipment in daily living. The increased use of electrically powered equipment in the home and in the workplace has reduced the need for the hand to exert great power, but has introduced a greater variety of precision movements required to operate switches and controls.
A large number of muscles, originating in both the forearm and the hand, is inserted into the fingers and the thumb. Most of the tendons of these muscles pass over several joints, and the combinations of different directions of pull of the tendons allow the fingers to move in a variety of ways.
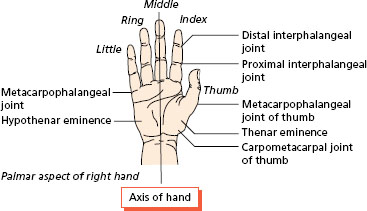
- The five digits are numbered 1–5 from lateral (thumb) to medial.
- The fingers are identified by name: index finger, middle finger, ring finger, little finger.
- The central axis of the hand extends through the third metacarpal and the third (middle) finger.
- When the fingers separate, the other fingers move away from the central axis (Figure 6.8).
- The names of muscles moving the fingers include ‘digitorum’, while those moving the thumb include ‘pollicis’. Thenar muscles are associated with the thumb, and hypothenar muscles are associated with the little finger.
Joints of the fingers and thumb
The main joints are identified in Figure 6.9.
The metacarpophalangeal (MCP) joints, commonly known as the knuckles, are formed by the articulations of the heads of the metacarpals with oval concavities at the base of the proximal phalanges. The thumb, as well as the four fingers, has an MCP joint. The MCP joints of the fingers are synovial ellipsoid, biaxial joints. Each MCP joint of the fingers has a strong palmar ligament, which is attached firmly to the phalanx but loosely to the metacarpal bone. The palmar ligaments of these four joints are connected by a deep transverve ligament, which holds the heads of the metacarpals together to form the body of the palm of the hand. The collateral ligaments are bands present on each side of the joints (Figure 6.9). The movements of the MCP joints allow the fingers to flex and extend, abduct and adduct. In abduction, the fingers move away from the middle finger, which forms the central axis of the hand.
Figure 6.8 Palmar view of the right hand; location of the joints.