Introduction
Upper limb function depends on five roots of origin of spinal nerves in the neck. These spinal roots branch and join in a complex manner forming the brachial plexus, which passes over the first rib and under the clavicle to reach the axilla. There, five nerves emerge and pass down the limb to supply all of the structures in the arm, forearm and hand. Traction injuries to the upper limb can tear the roots from the spinal cord. If all of the roots are involved, upper limb function is lost. The brachial plexus is also vulnerable to pressure in the axilla.
The brachial plexus
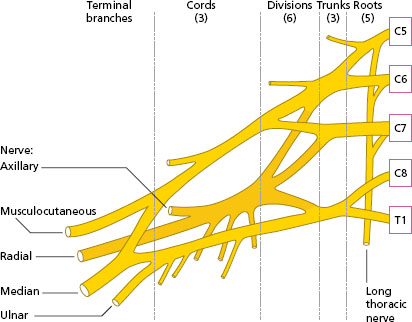
The position and plan of the brachial plexus are shown in Figures 7.1 and 7.2. The plexus is derived from five spinal segments, C5–C8 and T1. Three trunks are formed by the upper two and the lower two roots joining. These three trunks pass downwards and laterally between two muscles of the neck: the scalenus anterior and medius (see Chapter 10, Figure 10.7). The trunks meet the axillary artery and continue with it behind the clavicle. Each trunk then divides into anterior and posterior divisions to deliver the nerves to the anterior and posterior aspects of the limb, respectively. The six divisions continue through the axilla where they combine to form three cords lying behind the pectoralis minor muscle (see Chapter 5, Figure 5.6) and surrounding the axillary artery. The posterior divisions form the posterior cord, and the anterior divisions form the medial and lateral cords.
The posterior cord terminates in the posterior extensor nerve of the upper limb. The medial and lateral cords terminate in the flexor nerves of the upper limb. At the lower part of the axilla, the three cords split into the five terminal branches which enter the arm (Figure 7.2).
Figure 7.1 Position of the brachial plexus.
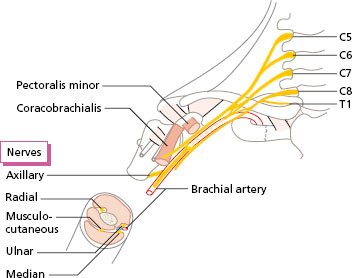
Figure 7.2 Plan of the brachial plexus showing the origin of the terminal branches.
Terminal branches of the brachial plexus
There are five terminal branches of the brachial plexus. The movements that are activated by each of the five nerves can be summarised as follows:
- axillary nerve: shoulder movement;
- radial nerve: extension of the elbow, wrist, fingers and thumb;
- musculocutaneous nerve: flexion of the elbow;
- median nerve: flexion of the wrist and fingers, opposition of the thumb;
- ulnar nerve: fine manipulative movements of the fingers.
The five nerves enter the arm. The axillary nerve terminates at the shoulder. The other four nerves continue through the arm and on to the forearm, where the radial and the median nerves divide into two. The muscular branches of the musculocutaneous nerve terminate at the elbow, and those of the radial nerve end at the wrist. The median, ulnar and radial nerves (cutaneous branch only) enter the hand.
Look at Figure 7.2 to see how the radial nerve originates from all the roots of the plexus, and the ulnar nerve from the lower roots (C8 and T1).
Axillary nerve: shoulder movement
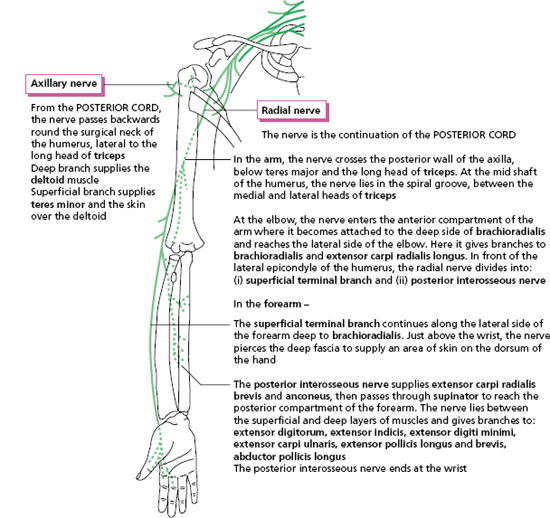
The axillary nerve nerve is important in all movements that lift the arm away from the side of the body, since it supplies the deltoid muscle and teres minor (Figure 7.3). From the posterior cord, the axillary nerve branches backwards under the capsule of the shoulder joint, and winds round the surgical neck of the humerus to supply the whole of the deltoid muscle. A branch to the teres minor continues as a cutaneous nerve supplying the skin over the deltoid muscle.
The other muscles moving the shoulder (except for the trapezius) are supplied by direct branches of the plexus in the neck.
Radial nerve: posterior extensor nerve
The radial nerve is the largest branch of the brachial plexus, formed as the continuation of the posterior cord (Figure 7.3). In the arm, the radial nerve supplies the whole of the triceps muscle. The nerve is essential for extension movement of the elbow, since the triceps is the only muscle capable of this movement with any power (see Chapter 5).
In front of the lateral epicondyle of the humerus at the elbow, the nerve divides into two.
- The superficial terminal branch continues along the lateral side of the forearm under the brachioradialis. Just above the wrist, the nerve pierces the deep fascia to supply a variable area of skin over the dorsal surface of the hand on the thumb side (Figure 7.4).
- The posterior interosseous nerve supplies the extensor muscles in the forearm, ending at the wrist, where it supplies all of the joints of the wrist.
Figure 7.3 Axillary nerve and radial nerve: course and distribution, right anterior view.
The radial nerve as a whole supplies all of the extensor muscles of the arm and forearm. The nerve has no motor role in hand function. Extension movements of the elbow are important for reaching above the head. Extension of the wrist is important in maintaining the functional position of the hand (Figure 7.5a) for all movements of the fingers and thumb.
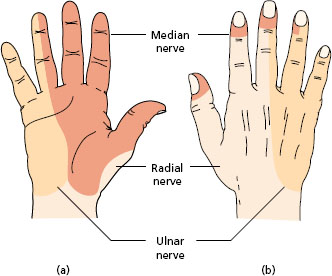
Figure 7.4 Areas of skin supplied by the radial, median and ulnar nerves: (a) palmar; (b) dorsal.