DEVELOPMENT
Morphologic description of the embryo provides a gross understanding of development [A]. Lodged within this is an orderly, sequential expression of genes known as a developmental cascade, which is under the control of HOXD genes expressed in successive overlapping fields. The apical ectodermal ridge releases fibroblast growth factors that induce the zone of polarizing activity, located in the posterior mesenchyme of the bud, to secrete sonic hedgehog to establish anteroposterior (radioulnar) polarity in the developing limb. Dorsal ectodermal expression of the WNT7A, which induces mesodermal LMX1B, and suppression of WNT7A in the ventral ectoderm by EN1 determine the dorsoventral axis of the limb.
Anomalies may be classified according to abnormality of development [B]. Upper limb anomalies are features of several syndromes [C].
EVALUATION
Observation
Hand function progresses in an orderly fashion [D]. The function of each upper limb is more independent than that of the lower limbs; thus, a short arm causes less functional difficulty than a short leg. Look for deformity, asymmetry, anomaly. What is the resting position? Watch how the child uses the upper limb—toys are helpful. Does the child have bimanual function? Does the child guard? Does the child express hand dominance? Determine functional limitations, such as bringing the hand to the mouth. What is the muscular tone? Are there contractures or spasticity? Ask about medical comorbidities that may be features of a generalized condition.
Physical Examination
A detailed motor and sensory assessment may not be possible in a young child. Ask the parents. Perform gross tests, such as distinguishing textures. Check passive and active motion. Look for signs of laxity, including elbow and metacarpophalangeal hyperextension, and thumb on volar forearm. Examine the entire child for other anomalies that may suggest a syndrome. Bring the child back for a second evaluation.
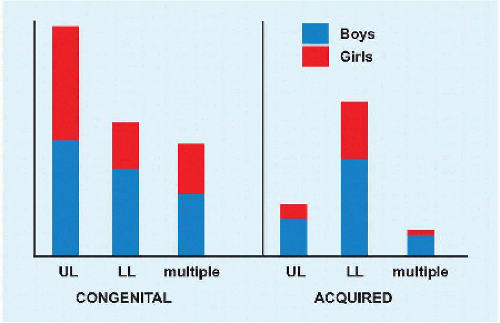
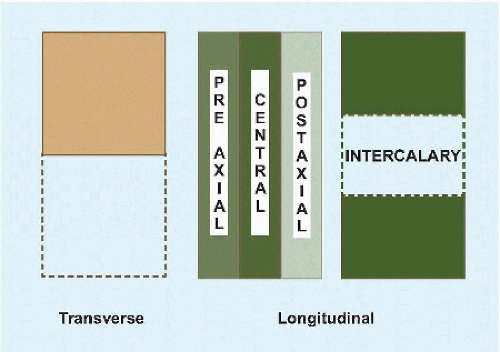
DEFICIENCY
Distinguish congenital from acquired deficiency [E]. Failure of formation may be transverse or longitudinal [F]. Symbrachydactyly is a transverse deficiency. Examples of longitudinal deficiency is radial clubhand, of central is split hand, and of postaxial is ulnar clubhand, and of intercalary is phocomelia.
Symbrachydactyly
Cause may be disruption of vascular ingrowth during limb development. Digits are “short” (Greek βραχvζ) and webbed “together” (Greek σvv-). Mildest is short, webbed but well-formed fingers. Cleft hand is characterized by absence of central digits [G]. Monodactyly refers to loss of fingers, marked by remnants or “nubbins,” with preservation of the thumb. Digital remnants lack a nail remnant, distinguishing this from constriction deficit. Peromelia (Greek πηροζ: “disabled, incapacitated”) is most severe, with absence of all digits.
Treatment depends upon what remains. Metacarpal spaces may be created for basic pinch. A hand plate may be fitted to a mobile wrist. Free vascularized toe transfer has variable success.
Preaxial Deficiency
There are six types.
N. Hypoplasia or absence of thumb. Wrist and radius are normal.
0. Hypoplasia or absence of thumb. Carpal anomaly. Normal distal radius. Proximal radius may be normal, dislocated, or synostosed with the ulna.
1. As 0, except distal radius shortening >2 mm.
2. Hypoplasia or absence of thumb. Carpal anomaly. Distal and proximal radial hypoplasia.
3. As 2, except absence of distal epiphysis of radius.
4. Hypoplasia or absence of thumb. Carpal anomaly. Absent radius [H].
The radial nerve and artery follow bone deficiency. Tethering by the radial anlage may dislocate the ulna. Half of cases are bilateral, most of which are associated with a syndrome, for example, Holt-Oram, thrombocytopenia-absent radius, and VACTERL.
Soft tissue stretching may be achieved by serial splinting or casting. Pollicization of the index substitutes for nonfunctional thumb. Centralization or radialization of the ulna supports the hand when there is significant radial hypoplasia. This is contraindicated in elbow stiffness, which may prevent accessing the mouth by a straightened hand and wrist, which previously were more functional in the deviated and shortened position.
Postaxial Deficiency
Ulnar deficiency differs from radial deficiency in being 1/10 as common, in showing autosomal dominant inheritance, in rarely being associated with a syndrome, and in being typically unilateral. In addition, the consequences to the hand are milder, whereas the elbow is more severely affected. There are four types.
I. Hypoplasia of the ulna, with preservation of proximal distal physis and minimal deformity.
II. Absent distal ulna, with radial bowing. This is most common.
III. Complete absence of ulna.
IV. Absent ulna with humeroradial synostosis.
Thumb and carpal anomalies occur variably. Excise the ulnar anlage and perform a corrective radial osteotomy for ulnad deviation of the wrist. Fuse the proximal ulna to radius to create a single bone forearm: this stabilizes the head of the radius, thereby improving elbow function, and reduces bowing of the forearm.
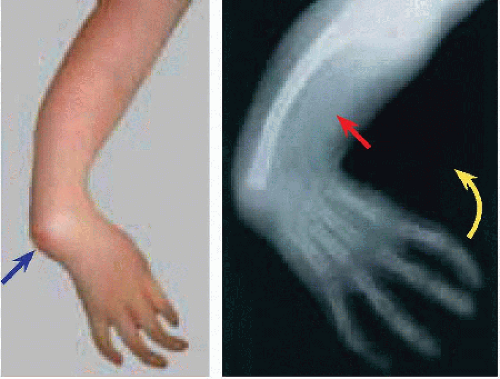
Phocomelia
The appellation describes resemblance of the severely shortened limb to that of a “seal” (Greek φεκη). An epidemic in Europe developed after thalidomide became an over-the-counter drug in Germany (1957) for nausea in pregnancy. It is rare today and may be due to true intercalary deficiency or severe axial deficiency [I].
FAILURE OF DIFFERENTIATION
Syndactyly
The upper limb develops as a zeugopod (arm), then stylopod (forearm), and then autopod (hand). This is associated with sequential expression of HOXD9 and HOXD10 (zeugopod) followed by HOXD11 and HOXD12 (stylopod), which in turn give way to HOXD13 (autopod). Mutation in HOXD13 on 2q31.1 results in failure of programmed interdigital apoptosis and syndactyly.
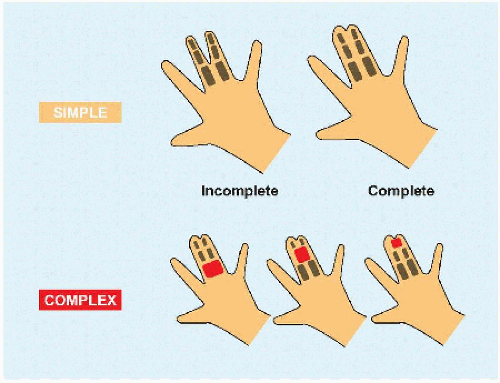
Syndactyly has been classified according to affected tissue and extent of joining [A]. When osseous abnormalities are more than side-to-side fusion, such as accessory bones, it is referred to as “complicated.” Syndactyly is most common in the third web, by contrast with the second web in the foot. It may be associated with syndromes such as Apert.
There are several principles of surgical separation [B].
Full-thickness, local, dorsal, or volar skin flaps to avoid contracture and “web creep.”
Zigzag incisions to avoid longitudinal contracture.
Operate on only one side of a digit, to avoid vascular insufficiency.
Correct underlying osseous deformity.
Relaxed closure to avoid vascular constriction.
Symphalangism
This refers to failure of cavitation of the interphalangeal joints, usually of the ulnar digits. Three types have been distinguished:
Affected digits is normal in length.
Brachysymphalangism, in which the digit is “short” (Greek βραχvζ).
Symphalangism associated with syndromes.
Digits are gracile and lack cutaneous creases. There is loss of motion and narrowing of the joint on röntgenogramme, to which the cartilaginous bridge is invisible. Release, for example, by capsulectomy, has limited success. Arthrodesis is unnecessary. Children adapt to the stiffness.
Camptodactyly
This refers to contracture of the finger in the sagittal plane [C]. Smallest finger and proximal interphalangeal joint are most affected. In a subset of patients, the condition is genetic, linked to 3q11.2-q13.12. This also is known as streblomicrodactyly (Greek στρεβλοζ: “bent, crooked”). There are three types of camptodactyly.
I. Congenital
II. Progressive, presenting in the second decade
III. Affecting multiple digits and associated with other conditions, in particular arthrogryposis
Intrinsic imbalance due to muscle anomaly, for example, errant lumbrical insertion or hypoplastic tight flexor digitorum superficialis, produces secondary soft tissue contracture and osseous deformity, such as condylar blunting.
Initial management is stretching and splinting. If this is unsuccessful, release anomalous muscle insertion or transfer flexor digitorum super-ficialis to the extensor retinaculum when the deformity is flexible. For rigid deformity, add wide capsular release and consider osteotomy.
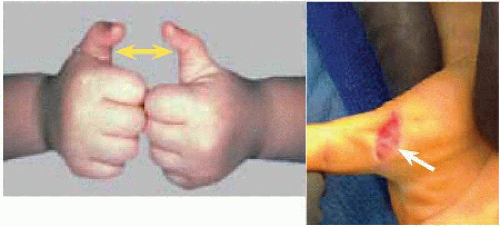
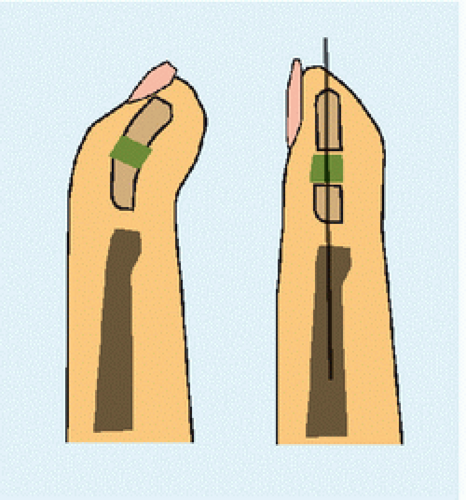
Trigger Thumb
The flexor pollicis longus develops a nodular swelling (Notta) that restricts and ultimately obstructs excursion at the entrance of the tendon sheath. This is not congenital. Cause is unknown. One-fourth are bilateral. The thumb may click and hurt with forcible interphalangeal extension, as the nodule squeezes abruptly past the first anular pulley, or it may be held in fixed flexion. The mobile nodule is palpable as the interphalangeal joint is manipulated. To compensate for lack of interphalangeal extension, the metacarpophalangeal joint may become hypermobile, extending abnormally to better position the pulp of the thumb during opening of the hand.
Observe trigger thumb during the 1st year of life, as most resolve spontaneously. Resolution is unlikely after the 2nd year, which is an indication for operative section of the first anular pulley. Demonstrate full interphalangeal extension to confirm acceptable release. The surgical site may be traversed by the radial digital nerve [D], which may be endangered by a percutaneous method. By 3 years of age, development of diffuse contracture at a flexed interphalangeal may limit surgical result. For patients with hyperextension of the metacarpophalangeal > 60 degrees, some advocate concomitant advancement of the volar plate.
Clinodactyly
In contrast with camptodactyly, the finger in clinodactyly (Greek κλιvη: “that upon which one reclines, a couch,” whence “clinic”) is deformed in the coronal plane [E]. Most affected is the smallest finger. This deformity tends to be bilateral and associated with syndromes, for example, 80% of children with trisomy 21. It is classified.
Simple, due to osseous deformity, or complex, which has associated soft tissue contracture.
Uncomplicated, when the deformity is < 45 degrees, or complicated when > 45 degrees associated with rotation.
Because of the plane of deformity, this leads to dysfunction when severe. For significant digital overlap, perform an opening wedge osteotomy rather than closing, which may relax the extensor to produce a mallet finger.
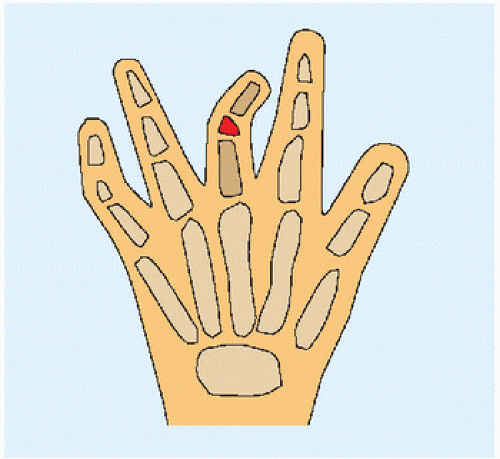
Delta Phalanx
The name describes the shape of a triangular bone, like the Greek letter delta (Δ), which on its short side is flanked by a C-shaped bracket epiphysis (cf. Foot chapter). Most affected are the middle phalanx of the longest finger [F] and the thumb, where it may form a triphalangeal thumb. The bone produces a coronal plane deformity.
Excise an accessory delta phalanx in triphalangeal thumb early, before secondary deformity sets in. Physiolysis with fat interposition is an effective detethering in the child who has enough growth remaining to overcome a deformity that is not severe. For severe deformity in the older child, opening osteotomy with bone graft is indicated.
Kirner Deformity
Progressive volad and radiad curving of the distal phalanx of the smallest finger [G]. Cause of this growth disturbance is unknown. It tends to be bilateral and affects girls more than boys toward the end of the first decade. It is characteristic in appearance, which is the principal problem it poses because it causes no disability. Phalangeal osteotomy at the end of growth is indicated rarely.
DUPLICATION
Polydactyly
This is the most common anomaly of the upper limb. It may be preaxial, central, or postaxial [A]. It may be subtyped as A: full digital development, and B: rudimentary or pedunculated digit. Central lesions often are polysyndactylies.
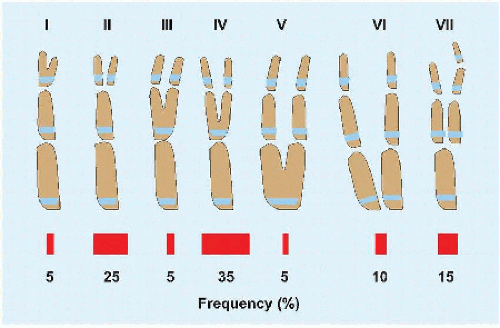
Thumb polydactyly has been classified according to osseous involvement [B]. While most are sporadic, type VII may be syndromic. A subset of triphalangeal thumb is caused by an autosomal dominant heterozygous mutation in a sonic hedgehog regulatory element (ZRS) that resides in intron 5 of the LMBR1 gene on 7q36.3.
For postaxial polydactyly, type B may be suture ligated or excised. Counsel family that the former, which is performed simply in the neonatal nursery, may be followed by a residual bump that does not interfere with function. For type A, reconstruct collateral ligament and hypothenar muscle attachments as indicated.
Principles of thumb polydactyly reconstruction include the following:
Timing is influenced by the development of pinch, toward the end of the 1st year.
Reconstruct the collateral ligament connected to the excised thumb.
Transfer thenar muscles, for example, in type IV, opponens and abductor insert on radial digit while adductor inserts on ulnar digit.
Perform chondroplasty of a widened metacarpal of metatarsal.
Recognize pollex abductus, and release the abnormal connexion between flexor pollicis longus and extensor pollicis longus. This is one cause of postoperative angulation, which is the most common complication of excision of thumb polydactyly.
UNDERGROWTH
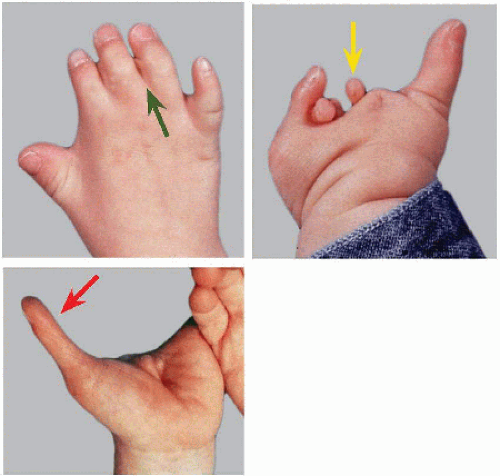
Thumb Hypo-/a-plasia
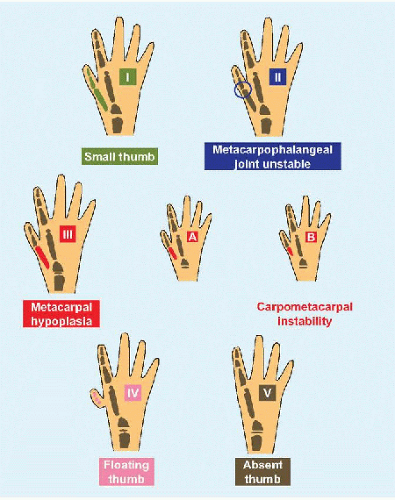
This also may be considered within the spectrum of preaxial deficiency. It is classified according to severity [C].
I. The thumb is small but otherwise muscles and joints are normal.
II. Metacarpophalangeal joint is unstable. Thumb is adducted. Thenar muscles are underdeveloped.
III. This is subtyped according to degree of metacarpophalangeal hypoplasia and presence of carpometacarpal instability (B and C).
Thenar muscles are absent. There is dysplasia of trapezium and scaphoid, as well as styloid process of radius.
IV. The thumb, consisting of rudimentary phalanges, floats at the side of the hand, connected by its neurovascular pedicle. Thenar muscles are absent. There is dysplasia of trapezium and scaphoid, as well as styloid process of radius.
V. Thumb is absent. This is most common.
Type I needs no treatment. Central to surgical decision making is the metacarpophalangeal joint. Reconstruction is possible when the joint is stable. An unstable joint is an indication for pollicization.
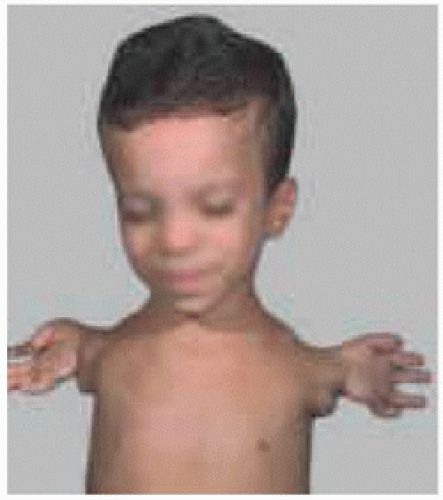
Poland Syndrome
This autosomal dominant disorder is characterized by unilateral chest hypoplasia, including unilateral hypoplasia or absence of pectoralis major muscle, most commonly the sternocostal head [D], as well as digital anomalies, including brachydactyly, oligodactyly, and syndactyly.
Other features include costal and vertebral anomalies, as well as absence of hypoplasia of shoulder muscles, including latissimus dorsi, serratus anterior muscle, and rotator cuff. It occurs on the right side in three-fourths of cases. Boys are affected thrice as often as girls. Most are sporadic, with a small subset demonstrating autosomal dominant inheritance.
The disorder may be regarded as part of the subclavian artery dysplasia complex, as evidenced by reports of dextrocardia in left-side cases (cf. Pseudarthrosis of the Clavicle).
A lower limb counterpart includes gluteal hypoplasia with brachysyndactyly of the toes.
Orthopædic management resides in the hand. Plastic reconstruction of the chest may be necessary, in particular for breast asymmetry and nipple absence.