Participation in sports is on an inexorable rise in Western culture. At play in this trend are the societal prioritization of physical fitness; a zeal for competition; the building of character, for example, confidence, self-image, discipline, and teamwork; a recognition that occupying a child’s time with sports is diverting from other allurements of youth, for example, the “screen-refrigerator” complex; and the financial incentives for sports industry and participant, for example, the promise of remuneration in college and beyond. Fueling the frenzy is the presumption that enjoyment is not enough: excellence and success are the driving goals, which may be achieved only by means of early adoption and specialization, for example, preschool, and long hours.
This chapter focuses on the distinctive aspects of sports in the immature skeleton, in contrast with the late teenager, who blends with the adult.
Physis
This provides the single sharpest contrast between children and adults with regard to injury and treatment (cf. Trauma chapter).
Maturation
Age is a stricter defining criterion in children than in adults, for example, 1 year separates middle school from high school, yet an ocean separates them socially, psychologically, and physically. Children mature at different rates, whereas adults are mature by definition. Differences are amplified by the growth acceleration of puberty, which correlates with the peak of serious injuries presenting to an emergency facility. The principal stratifier in sports participation during childhood is chronologic age. These factors account for unanticipated psychic and physical risks to children finding their place in sports. A method of stratification based upon assessment of biologic maturity, including such factors as Tanner stage, is more appropriate and safer.
Numbers
Comment
3%
High-school participants in soccer, basketball and American football who go on to play in division I or II
1%
Obtain a college scholarship for athletics
$10,000
Average scholarship
1/5000
Play at the professional level
A Success in youth sports The average scholarship covers half the cost of a state school and <1/4 the cost of a private institution. This must be balanced against the costs of lessons, camps, and time raising the elite athlete.
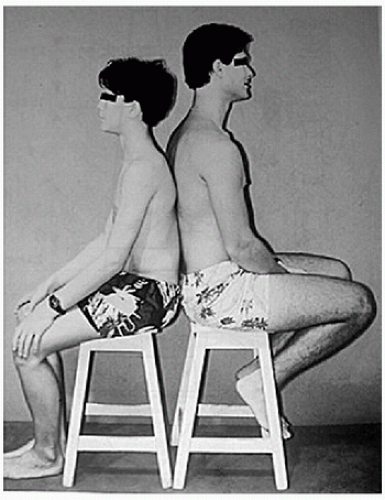
B Differential maturation Even though both are the same age, a boy sits next to a man. This has far-reaching implications on sports participation and performance [Blount].
Age
70’s
00’s
Preschool
5%
10%
Prepuberty
4%
15%
Adolescents
6%
15%
Food
Cost 1990 → 2007
Energy dense
Cola: ↓ 35%
Fast food: ↓ 10%
Vegetables
↓ 10%
C Childhood obesity Childhood obesity was stable until the early 1970s. Its rise coincides with the crossing of child per diem consumption of milk (decline) and cola (increase). It has doubled or tripled in a generation. Reductions in the price of food account for 1/3 of the rise in body mass index in children and young adults. There is no evidence that family income impacts obesity. However, maternal employment does (e.g., less time, more prepared food), correlating with a 10% to 33% rise in obesity of children in upper socioeconomic strata.
Gender
Vigorous physical activity delays menarche. A practical outcome is elimination of this as a measure of maturity in the management of conditions affected by growth, for example, scoliosis. Beware of the triad of amenorrhœa, eating disorder, and osteoporosis, which puts the female athlete at increased risk of overuse injuries or stress fractures. Maturation has a narrower window in girls than in boys, in whom it has a long tail, for example, running performance plateaus after puberty in girls whereas it continues to increase in boys.
Thermoregulation
Children’s capacity to regulate body temperature is less developed compared with that of adults. A greater surface area to body mass means greater heat absorption from the environment. A growing body produces more metabolic heat per mass unit during physical activity. Children sweat less, reducing heat dissipation by evaporation. They have a duller thirst response and so replenish fluid loss later than adults. These characteristics increase the risk of heat-related illness.
Obesity
Childhood obesity is multifactorial and in tumultuous evolution. Obesity may be defined as body mass index >95th percentile. Risk factors include urban residence, which highlights the effects of a sedentary lifestyle with greater access to food, uterine exposure to maternal diabetes and adiposity, and genetic factors in association with certain diseases, for example, Prader-Willi. Musculoskeletal complications include accelerated maturation, lower limb deformity such as Blount disease and slipped capital femoral epiphysis, and increased musculoskeletal complaints such as back pain, all of which may limit activity.
Even though input, for example, eating, and all the forces that influence it, including the economics of food, are ultimately more influential than is output, for example, exercise, sports are intimately intertwined and integral to abatement of the obesity epidemic.
Genetics
The type of sport in which a child participates is determined by interest (of child and parent), social environment, and continual competitive selection. The genetic basis for physical ability and psychological aptitude has remained veiled except for the most rudimentary characteristics such as height for basketball or weight for wrestling. An expanding body of research is uncovering gene polymorphisms that will allow a much more sophisticated understanding. For example, polymorphism in the gene encoding actin-binding protein α-actinin-3, a highly conserved component of fast-twitch skeletal muscle fibers, may separate power and speed athletes from endurance athletes. A recognition that genetics is an immutable component of the performance phenotype may decompress the family when the child does not meet expectations. Genetic testing to identify child aptitude, and the development of sports profiles, will enable more informed and rational decision making.
EPIDEMIOLOGY
Reporting (e.g., in sports that place a premium on toughness) and definitions (e.g., by a coach vs. trainer vs. physician) introduce imprecision in statistical analysis of sports injuries.
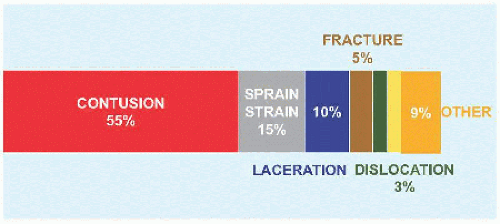
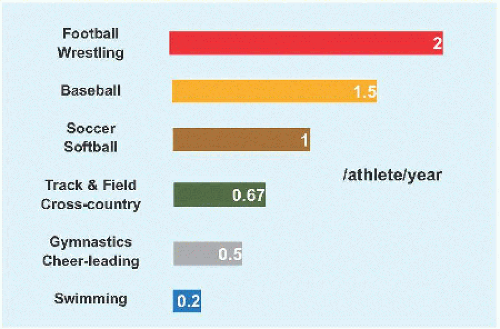
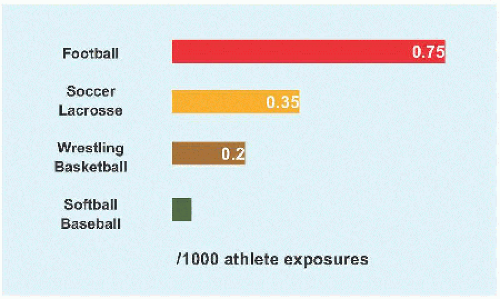
Two million children per annum are seen in an emergency setting for a sports-related injury. Another 2 million receive nonemergency medical care. Total cost of management of pædiatric sports injuries is $2 billion per annum. Most injuries are benign [A]. American football is most injurious [B] and most dangerous, having a 10 times greater rate of catastrophic event, such as permanent nerve deficit, than do other sports. Annual attrition from organized sports is 1/3, while total attrition by adolescence is 3/4. Boys sustain more injuries than do girls, whose rate is increasing more steeply due to more rapid increase in sports participation. Fractures and physial overuse injuries predominate in preteens, whereas ligamentous injuries come to the forefront in teenagers.
Injury Prevention
Sports and play injuries are unique in that exposure is elective, recurrence is not unusual, and prevention is possible. There are several strategies that may be taken to make these activities safer for children [C]. Threefourths of school playground fractures involve the upper limb, of which >1/2 are supracondylar humerus fractures (cf. Trauma chapter).
THE DISABLED CHILD
The International Wheelchair Games were hosted by Dr. Ludwig Guttmann (German-born refugee to England) on the opening day of the 1948 Summer Olympics in London, for World War II veterans with spinal cord injury. The first Paralympic (Greek παρα: “beside”) Games took place in Rome in 1960. There are six categories of disability: limited mobility or wheelchair, amputation, blindness, cerebral palsy, intellectual impairment, and other. The disabled realize the same benefits of sports as able-bodied children. Because they are less active at baseline, sports and strength training are essential for the disabled, including to control obesity, reduce contractures, increase muscle strength, build bone mass, and integrate into the society around them.
In children with Down syndrome, a requirement for participation in Special Olympics is no evidence of instability on lateral flexion-extension röntgenogrammes of the cervical spine. Special considerations for patients with spina bifida relate to vulnerability of skin to breakdown, including from brace wear; fractures, which restrict them from high-contact sports; and wheelchair use. For cerebral palsy, seizure control is essential.
Wheelchair injuries are primarily soft tissue. This ranges from blisters on the hand to decubitus ulcer, due to the design that raises the knees above the pelvis. Overuse injuries are common, in particular of the shoulders.
A Sports injuries in children Most are benign. Yellow represents concussion at 3%, which will command a larger proportion as focus is brought upon it.
B Injuries brought to medical attention by sport American football leads, followed closely by wrestling. Categories are simplified: in each, the upper has a slightly greater rate. For bigender sports, there are no significant differences. Softball approximates soccer rather than baseball.
6” between bars to avoid entrapment of limb or head No open hooks that may catch clothing
PRACTICE & GAME
Athlete
Fitness Strength training Rest Hydration Protective clothing
Coach
Use and maintenance of correct equipment Education, e.g., first aid, CPR, injury protocols Enforcement of safety rules Reporting of injury Multiple sports with no specialization
Community
Pre-participation assessment Funding, e.g., facilities, monitoring, medical care Evidence based rules and regulations Behavior modification
C Injury prevention in youth sports Recommendations in an evolving landscape. Some are straightforward, others nebulous. An example of the latter is behavior modification, yet 1/3 of athletes who quit include negative interactions with a coach or parent as a reason. Softness of wood chips is debated.
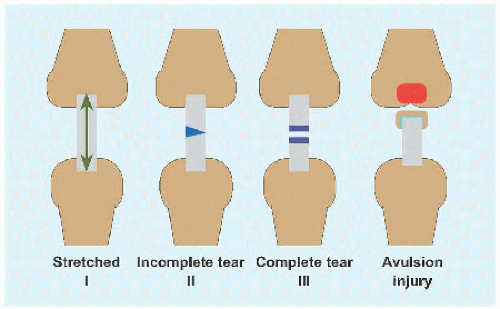
A Grading of ligamentous injury In type I, there is injury and pain but no instability. In type II, there is more motion but a clear endpoint on manual testing. Type III is characterized by instability, is associated with capsular injury, and lacks an endpoint. Avulsion is a reflection that ligament is stronger than bone in the immature child. The quintessential example is fracture of the intercondylar eminence of tibia.
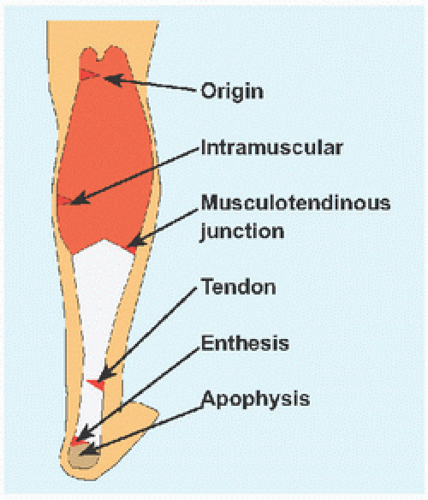
B Triceps suræ injury Different levels of injury present a constellation: muscle strain; tendinitis, including in association with retrocalcaneal bursitis; enthesitis, for example, associated with ankylosing spondylitis; and apophysitis (Sever).
Common Sites
Sport
Medial epicondyle
Throwing, (e.g., baseball)
Iliac spine
Kicking, (e.g., soccer)
Ischial apophysis
Jumping and landing, (e.g., gymnastics)
Apex of patella
Jumping, (e.g., basketball)
Tibial tubercle
Jumping, (e.g., basketball)
Calcaneal apophysis
Running and jumping, (e.g., soccer)
C Apophysial injury These result from traction during activities exemplified by the most common sports with which they are associated. The knee dominates in frequency.
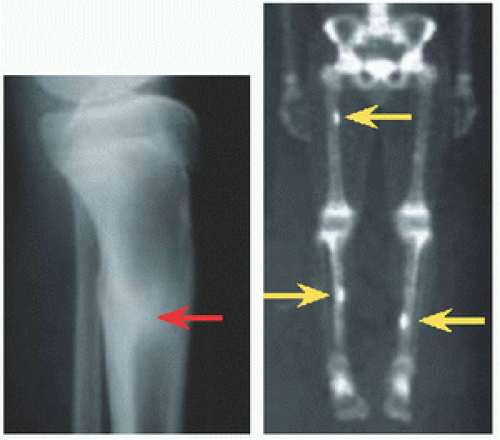
D Stress fracture Multiple may occur, as in this cross-country runner. Röntgenogramme shows hyperostosis (red). Scintigramme reveals involvement of both tibia and femur (yellow).
TYPE OF INJURY
Sports injuries may be acute or chronic, which may be described as overuse. Overuse injury results from repetitive submaximal loading, leading to microtrauma that may be reversed by rest. In the absence of rest, cumulative microtrauma results in stress injury. It is a diagnosis of exclusion:
Pain is intermittent, punctuated by periods of normal function. It does not awaken the child from sleep, even though it may delay falling asleep and require the comfort of a parent. It is not localized, for example, child cups the patella with the hand.
There are no objective signs of macroinjury, such as joint effusion or other inflammatory sign, deformity, instability, or atrophy.
While initially more benign than acute injury, overuse may take longer to heal; requires active involvement of the child for recovery and future prevention, for example, stretching program and other behavior modifications; and may result in more time away from sports. Rest is simple and cheap and effective, yet may be the most vexing prescription to child and family.
Sports injuries may be divided anatomically into ligament, muscle, physis, fibrocartilage and bone.
Ligament
Ligaments fail suddenly in most cases, by contrast with physial injuries, which tend to result from repetitive stress. Ligament injuries may be classified [A]. Ligament injuries are most common around the ankle and knee. They may coexist with bony injuries, as seen in tibial spine fractures.
Muscle
Injuries may be of muscle belly, tendon, or enthesis [B].
Physis
In addition to acute fracture (cf. Trauma chapter), children involved in sports may present with chronic repetitive stress injuries, for example, Little League shoulder (q.v.). Unlike acute fracture, the physis becomes widened, irregular, and tender, but not grossly unstable. One type of injury may usher in the other, for example, Osgood-Schlatter condition preceding fracture of the tibial apophysis. Certain synchondrosis disruptions are classified separately, for example, accessory navicular (cf. Foot chapter).
Fibrocartilage
This consists of meniscus and labrum. In the knee, the medial meniscus is more contrained (2-3 mm excursion) compared with the lateral meniscus (10 mm). The medial meniscus is more susceptible to trauma, leading to tear, while the lateral meniscus is more susceptible to reactive hypertrophy, as in the genesis of the discoid form. In the shoulder, the labrum is essential to stability, while in the hip the rôle of the labrum is less clear (cf. Hip chapter).
Bone
Acute fractures are discussed in Trauma. Chronic injuries may result from traction [C] or compression, for example, stress fracture and osteochondritis dissecans.
Stress fractures occur most frequently in the tibia (cf. Trauma chapter), metatarsal bones, and femur, for example, in runners [D], and the distal radius and at the pars interarticularis, producing spondylolysis, for example, in gymnasts (cf. Spine chapter).
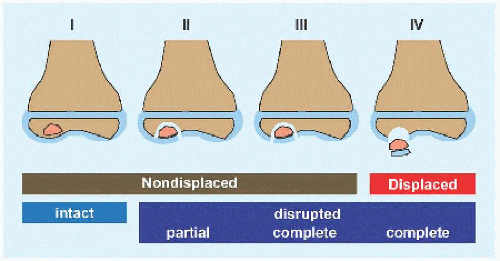
Osteochondritis dissecans represents segmental avascular necrosis of subchondral bone with injury to overlying cartilage. Causes include repetitive microtrauma and a genetic predisposition to localized juxta-articular ischæmia. A subgroup of patients may have been given this diagnosis for disordered epiphysial maturation. It is classified based upon the geographic extent of injury, as determined by injury and at time of operation [E]. Cartilage and stability guide treatment.
Stage I. Cartilage is intact and fragment is stable. Manage closed.
Stage II. Cartilage is partially disrupted but fragment is stable. Manage closed or open.
Stage III. Cartilage is completely disrupted. Fragment remains in place but is loose and at risk for displacement. Manage open, and include fixation.
Stage IV. Osteochondral fragment has displaced. In the acute setting, it may be returned to the donor site and fixed, with the expectation that it will heal. In the chronic setting, the fragment becomes eroded such that it cannot be put back. Reconstruct the donor site.
CONCUSSION
This also may be referred to as mild traumatic brain injury. Rapid short-duration neural impairment results from biomechanical force applied or transmitted to the head. The pathophysiology includes force resulting in ion dysregulation and vasoconstriction that lead to an energy crisis in the brain. Grading is retrospective, with severity determinable only after recovery. By definition, brain imaging is negative. It is impossible to estimate the scope of the problem because definition, classification, and diagnosis are in flux; however, there is universal agreement that concussion has been underestimated and is increasing.
Preparticipation screening is essential to establish a child’s baseline cognitive function. Concussion varies by sport [A]. Symptoms and signs may not appear until hours after the inciting event [B]. Loss of consciousness is rare, and if it lasts more than 30 seconds, should raise concern for a significant intracranial lesion. Assess an athlete away from the field in an environment that will be used for follow-up, such as a quiet room. Any evidence of a structural brain injury is an indication for brain imaging. Postconcussive symptoms and signs typically resolve after a week.
Remove a concussed athlete from the game, from physical exertion, and from school, for a period of “cognitive rest.” Allow a return to sports after resolution of signs and symptoms, but not sooner than a week. Because most repeat concussions occur within the first 2 weeks after injury, this may be regarded as a window of vulnerability and a guide for return to sports [C]. Recurrence of symptoms after exertion indicates incomplete recovery. There is no consensus on retirement of an athlete from a sport. This may be considered for the athlete who sustains three concussions in the same season or in whom postconcussive symptoms and signs persist beyond 3 months.
STRENGTH TRAINING
This also is known as resistance or weight training. Strength training enhances muscle power (by resistance) and endurance (by repetition). Strength training differs from body building, which is occupied with æsthetics and stands on its own as a competitive sport. Goals of strength training include both improved performance and reduced injury.
Weights may be free, for example, dumbbell, or static, for example, machine. By requiring control of a limb in space, free weight improves coordination and balance as well as strength. Static weight, in a supported position, is safer. Closed chain exercises are performed with the hand or foot stabilized. A free hand or foot opens the chain. Isotonic exercise maintains a fixed resistance while muscle length varies. In isometric exercise, a muscle contracts without changing its length, for example, in an immobilized limb. Muscle contraction may be concentric, in which length decreases, or eccentric, characterized by lengthening of the muscle during resistance. The latter may accelerate power acquisition at the expense of an increase in injury rate. Alternating concentric and eccentric contraction in rapid succession forms the basis of plyometrics, or jump training, which may reduce the rate of anterior cruciate ligament tears in female athletes.
Strength training in prepubertal children is effective without muscle hypertrophy by recruitment of motor neurons for a given muscle mass.
Begin strength training after 7 years of age, by when a child has developed adult balance and posture control. A schedule of 2 to 3 times/week for 3 months will yield significant results safely. Start with large muscle groups and transition to small. Maintain high repetitions (10) and titrate resistance in 10% increments. Perform 1 to 3 sets with 1 to 3 minutes of rest between them. Book end each session with a 10-minute period of warm up, including stretching, and a 10-minute cool down. “Detraining,” or loss of strength, occurs at 5% to 10%/week. There is no deleterious effect on growth. With proper technique and supervision at no lower than 1:10 instructor:student ratio, there is no increase in injury.
E Classification of osteochondritis dissecans I: Osteonecrosis. II: Dead bone has become separated from surrounding bone, as evidenced by a “halo.” Cartilage (blue) is partially injured. III: Overlying cartilage is completely broken. Fragment remains in place but is loose and at risk for displacement. IV: Osteochondral fragment has separated or become “dissected” (König) to become a mobile body. There is no desiccation, or “drying.”
A Concussion by sport American football leads. Data for certain high-risk sports, for example, ice hockey, are limited.
B Symptoms and signs of concussion Balance may be tested by three positions: standing on both feet with hands on iliac crests with open and shut eyes and standing on the nondominant foot.
Concussion rehabilitation
No physical activity + cognitive rest
Light aerobic exercise
Sports-specific exercise
Noncontact drills
Full-contact practice
Game
C Concussion rehabilitation Return to sports is gradual. Once symptoms and signs have resolved, the athlete may progress through each stage no faster than every 24 hours.
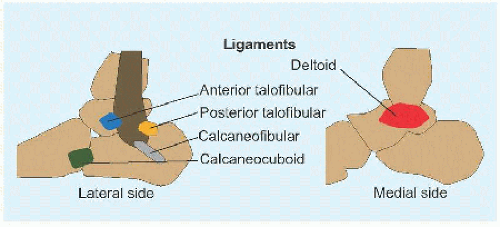
A Ankle ligaments The anterior talofibular ligament, extending from anterior margin of the fibular malleolus to the talus distal to its lateral articular facet, is most frequently injured. The calcaneofibular ligament, the longest, is a rounded cord that courses from fibular malleolus to a tubercle on the lateral surface of the calcaneus, where the peronei longus and brevis run over it. The posterior talofibular ligament, the strongest of the lateral complex, runs from fibular malleolus to a tubercle on the posterior surface of the talus lateral to the groove for flexor hallucis longus. The deltoid drapes over the tibial malleolus and has two laminæ. Superficial consists of tibionavicular, calcaneotibial, and posterior talotibial. Deep consists of anterior talotibial fibers.
Attenuation
Mild swelling and tenderness
Partial tear
Moderate swelling, unable to bear weight
Complete tear
Marked swelling, bleeding, instability, and disability
B Grading of ankle sprains.
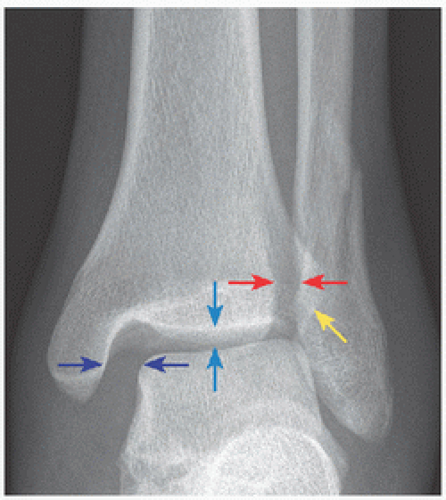
C Deltoid disruption The ankle of this mature teenager was stepped on, resulting in an acceptably displaced distal fibula fracture. The force emerged through the deltoid ligament, widening the medial joint (navy) compared with the superior tibiotalar distance (blue). Normal clear space is <6 mm (red) and normal overlap of fibula and tibia is >1 mm (yellow) on mortise view.
ANKLE
The ankle accounts for the largest number of orthopædic complaints in the child athlete. Sports as a stress test may awaken silent conditions, such as tarsal coalition, or turn normal into abnormal, such as irritation of the calcaneal apophysis.
Ankle Sprain
This represents tear of one or more ankle ligaments, which may be divided into medial and lateral [A]. The medial is termed deltoid, after its resemblance to an upside-down Greek letter delta, Δ. The lateral group consists of three independently named ligaments. Ankle sprains may be classified by severity [B]. With increasing severity, more of the ligamentous complex is torn, bearing with it more pain and instability. The peak incidence of ankle sprain is in latter teenage years. Basketball is the most abundant source (25%), followed by soccer (20%) and American football (15%).
Ankle sprains may be recurrent, due to excessive force in the coronal plane transmitted to the ankle by a tarsal coalition that limits subtalar motion. Also in the differential diagnosis are peroneal retinacular tear and traction on an accessory os subfibulare.
Most ankle sprains are produced by an inversion mechanism. Eversion (1%) produces the high ankle sprain, in which there is disruption of the tibiofibular syndesmosis. Direct force to the lateral leg results in a valgus moment on the knee and external rotation of the ankle.
Evaluation Ask about the mechanism of injury, such as “rolling” the ankle. Swelling may be focal, for example, anterolateral at the anterior talofibular ligament, or diffuse, suggesting a more complete injury that includes the entire lateral ligamentous complex. The deltoid ligament is injured rarely in children. Cutaneous change, for example, ecchymosis, may track beyond the ankle, marking the extent of soft tissue disruption. Look for foot deformity, and range the subtalar joint, to rule out tarsal coalition. Percussion, which will transmit force to bone while minimizing stretch to injured soft tissues, above the tip of fibula may reveal physial injury; immediately beyond the tip, it may reveal os fibulare avulsion.
Only gold members can continue reading. Log In or Register to continue