Converse to adults, deformity commands the largest proportion of spine care in children. Back pain, while not infrequent, in most children will have no identifiable cause.
EMBRYOLOGY AND DEVELOPMENT
At the end of the 2nd week, the embryo is trilaminar, composed of endoderm (which gives rise to the gut) adjacent to the yolk sac, ectoderm adjacent to the amnion, and mesoderm in between.
Ectoderm gives rise to the nervous system. The notochord appears during the 3rd week, at the beginning of gastrulation. The notochord (of which the vestige is the nucleus pulposus) induces the formation of the neural plate. The neural plate begins to fold into the neural tube in the 4th week from its center rostrad and caudad, a process known as neurulation. During neurulation, there is disjunction of the superficial ectoderm, which goes on to form the skin.
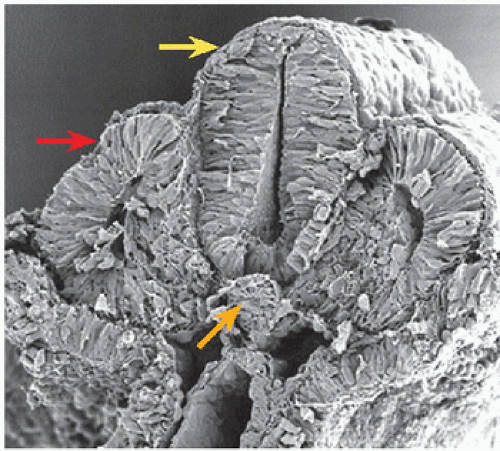
Paired blocks of mesoderm, known as somites, give rise to the musculoskeletal system [A]. The part of a somite that forms bone is known as a sclerotome and that which forms muscle is a myotome. During the 4th week, the sclerotome grows around the notochord to become the vertebral body and anulus fibrosus and around the neural tube to form the vertebral arches.
A Scanning electron micrograph of an embryo Somite, red. Neural tube, yellow. Notochord, orange. [http://php.med.unsw.edu.au]
B Vertebral intersegmental development The vertebral bodies form as intersegmental structures. As blood vessels grow between somites, their final position is midvertebral. The site of blood vessel entry and somite fusion may appear radiographically as an anterior notch in the vertebral body of the child (red).
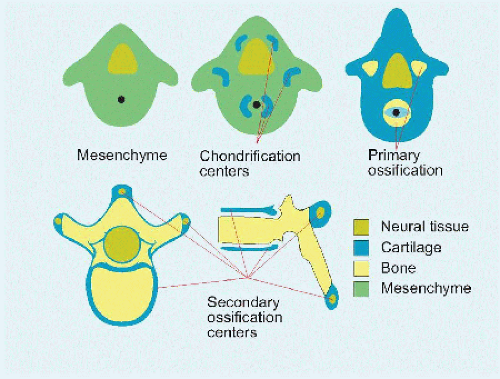
C Vertebral development Chondrification leads to ossification, which is complete by maturity. From Moore KL. The Developing Human. 4th ed. Philadelphia, PA: WB Saunders; 1988.
The rostral half of one sclerotome fuses with the caudal half of the adjacent one to form each vertebra. This intersegmentation means that original vascular ingrowth between somites ends in midvertebral segmental blood vessels. Anterior notching of vertebrae in the immature spine marks the site of somite fusion [B].
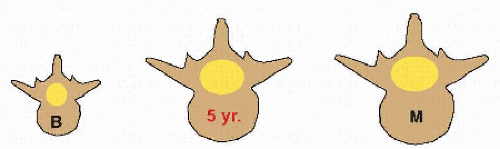
During the 7th to 8th weeks, paired chondrification centers appear around the notochord, which will fuse during the process of ossification to form the centrum of the vertebral body; around the neural tube, where they fuse to form the neural arch; and at each transverse and spinous processes, where their rôle is apophysial [C]. Fusion of the neurocentral junction occurs by 5 years of age, at which time the final capacity of the vertebral canal is determined.
Differential growth of the spinal cord and vertebral column leads to ascension of the conus medullaris to its adult level at L1 by the first few months of age. This is accompanied by formation of the cauda equina, as lumbosacral nerves travel to reach their respective intervertebral foramina. The spinal cord is anchored to the coccyx by the filum terminale.
In the coronal plane, the spine is straight throughout growth. In the sagittal plane, the spine evolves from a single curve at birth to a triple curve.
A knowledge of embryology and its nomenclature aids an understanding of disease.
Dysrrhaphism refers to a “bad” “groove,” a general term for midline, that is, spine anomaly
Schisis refers to “splitting, cleavage, or schism” of the spine. Two types are distinguished, myeloschisis: “splitting of the medulla, or spinal cord,” and rhachischisis: “splitting of the osseous spine.”
Spina bifida is the general term for “splitting of the spine.” This may be aperta: “open,” in which nerve has escaped the confines of bone, or occulta: “closed,” characterized by retention of nerve within an open osseous canal (a benign, often radiographic finding most frequently located at the lumbosacral junction that affects up to ¼ of the normal population).
Spina bifida aperta includes myelomeningocœle, which results from incomplete neurulation.
Premature disjunction leads to migration of mesoderm into the neural tube, where the mesodermal cells are induced to form fat and ultimately a lipomyelomeningocœle.
Failure of disjunction accounts for cutaneous signs of dysrrhaphism, such as hairy patch or sinus.
Failure of ascension may result in tethered cord.
Adhesion between endoderm and ectoderm results in split cord malformation, such as diastematomyelia or neurenteric cyst.
Hyperkyphosis may be observed for the first 2 years for the normal development of sagittal contour during growth.
Fusion of the spine before 5 years of age, that is, before ossification of the neurocentral junction, risks iatrogenic stenosis of the vertebral canal.
Development of the vertebrae is associated most closely with that of the neuraxis, genitourinary system, and heart. As a result, an insult to one system may insult them all, and evaluation of one should include evaluation of the others.
EVALUATION
History and Physical Examination
Sit down, and take some time to gain the confidence of the child (and family): the spine is a site of awkwardness and vulnerability. Examine the whole patient. Is this an isolated problem of the spine, or part of a generalized disorder? Look at other systems, such as the skin, where café au lait spots suggest neurofibromatosis or a midline stigma points to dysrrhaphism.
History Directly and independently include the child, who may express a different complaint from parent or referring physician. For example, the child may be more concerned about the appearance of spine deformity than the pædiatrician, who may be focused on long-term consequences. Ask the family, which may reveal a genetic disorder. Because of the gravity of diagnosis, many other disciplines have become involved in spine care; be considerate as you navigate this world with patient and family.
Physical examination Develop a standard approach, including the following:
Age. This is the most important patient characteristic in any disease.
Other measure(s) of maturity [A].
Progression of spine deformity is proportional to growth.
Gender. Certain conditions are more frequent or have a different natural history according to gender.
Gait. This may be influenced by pain or neural function.
Pain. This traditionally has been underestimated in children and in certain conditions (e.g., scoliosis).
Palpation. In particular tenderness, and step-off (e.g., spondylolisthesis).
Lower limb length discrepancy. This may produce an apparent or secondary spine deformity.
Plane of deformity. Evaluate spine in three dimensions: coronal, transverse, and sagittal.
Trunk asymmetry. Include the shoulder, scapula, ribs, breast, flank, iliac crest.
Spine balance. Plumb line dropped from inion to natal cleft [B].
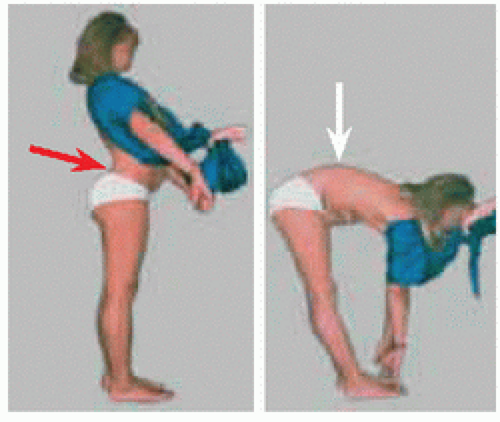
Spine motion, including Adams forward bend test.
Neural examination. Spine deformity may be primary or secondary to a neural lesion.
Skin. Look for cutaneous signs of decompensation in the setting of deformity [B] and for a midline sign of dysrrhaphism.
Imaging
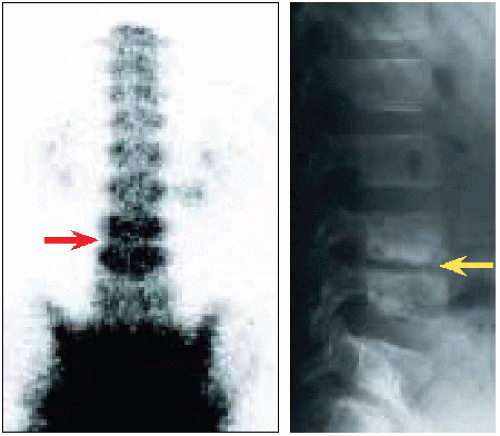
Röntgenogramme is the fundamental screening modality for spine deformity and for back pain. The latter also may be screened with scintigramme, which may detect a radiographically occult lesion [C].
Scintigramme allows a dynamic or physiologic assessment of bone: the phosphorus attached to technetium (99mTc) medronic acid is taken up by bone undergoing turnover, as in an active spondylolysis that has potential to heal or in inflammation induced by infection.
Single photon emission computed tomography (SPECT) allows localization of scintigraphic uptake in a vertebra, for example, the pars interarticularis in spondylolysis.
Computed tomography (CT) gives the best detail of vertebral architecture [D]. It confirms spondylolysis. In neurofibromatosis, it reveals osseous erosion. In tumors, it defines margins. In complex deformity, it allows understanding of the three-dimensional shape of the spine and aids planning of operative treatment.
Magnetic resonance imaging (MRI) shows the soft tissue, in particular neural, intervertebral disc, muscle, ligament. Indications for MRI include abnormality on physical examination, such as weakness or upper motor neuron sign, as well as symptoms or signs of atypia such as thoracic hyperkyphosis, early age of presentation.
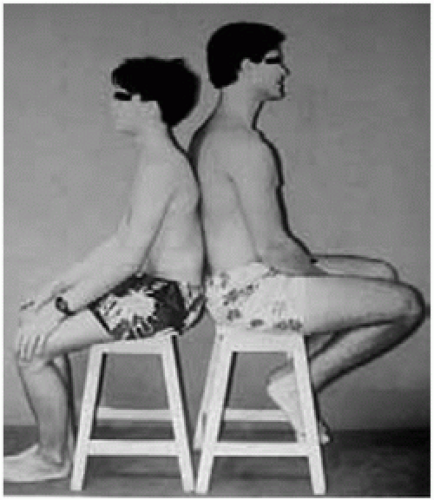
A Maturity Maturation is variable. Girls mature earlier and more predictably than boys. The ethnic spectrum is broad. These two boys are 16 years old.
B Skin decompensation The skin shows stretch marks and callus over an inflexible kyphosis. This is an objective sign that the deformity is significantly impacting (and will impact) the patient’s function, such as sitting against the back of a chair.
Imaging method
Indication
Röntgenogramme
Osseous deformity
Oblique röntgenogramme
Lumbosacral spondylolysis
Ferguson view röntgenogramme
Spondylolysis Lumbosacral fusion
Scintigramme
Back pain—initial screening Osseous activity—spondylolysis, infection, tumor
C Imaging methods and their indications These are not a substitute for history and physical examination. Obtain judiciously: incidental findings may lead to unnecessary intervention.
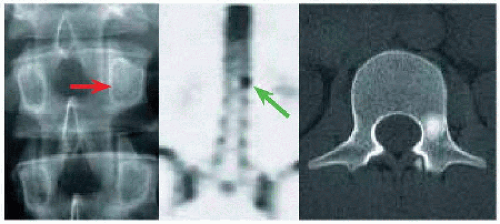
D Osteoid osteoma of the spine Distortion of pedicle on röntgenogramme (red) was associated with focal increased uptake on scintigramme (green). CT scan showed a geographic, sclerotic lesion in the pedicle (yellow), guiding excision.
BACK PAIN
Prevalence
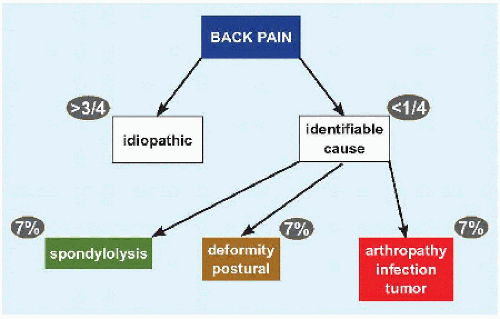
Drawing upon engineering and aviation, in medicine, back pain resembles a “black box.” Up to 1/3 of children complain of back pain; the incidence increases in adults to >2/3 in adults.
Causes
In more than three-quarters of these, no cause can be identified; such children are said to have “overuse” or “growing” or idiopathic pain, in the same way they may complain of other sites in the skeleton [A]. The most common identifiable cause is spondylolysis, followed by deformity such as hyperlordosis. Less than 10% of children will present with a significant arthropathy, infection, neural lesion, or tumor, which should assure the physician to take a measured approach to evaluation and management.
CANDIF
One CANDIF (ferentiate) “good,” or benign or idiopathic, from “bad” back pain, which should raise concern for an identifiable cause.
Constant. Come and go pain typically is mechanical, from overuse.
Associated symptoms or signs. This includes abnormality detected on physical examination, such as neural deficit or deformity.
Nocturnal. Pain that arouses a child from sleep is more concerning than pain that interferes with falling asleep, which is typical of overuse pain.
Duration. Follow-up a patient with pain <3 months. The physician may be at odds with the patient, who may regard duration >3 months to be evidence that something is amiss, since the pain has not resolved spontaneously. Educate the patient that a significant morbid process accounting for pain would manifest in other ways after several months or years.
Intensity. Take note of pain that is worsening inexorably, as opposed to pain that may wax and wane within a stable range.
Focal. Focal pain is more likely to have a structural cause. Pain that is diffuse, or that radiates in a nonanatomic distribution, is more typical of overuse.
Evaluation
History and physical examination are the foundation. Image judiciously: results may be misleading, they may raise anxiety unnecessarily, they may lead to unhelpful “treatment”, and they add cost.
Röntgenogramme. This is the first-line modality, particularly useful for spondylolysis and deformity. It also shows loss of height in discitis.
Scintigraphy (including SPECT). For spondylolysis and occult process. This may be a screening tool for “serious” disease.
MRI. For tumor, infection, or neural lesion (in particular in association with radiculopathy).
CT. In the evaluation of back pain, this often serves a confirmatory rôle, such as to define spondylolysis or to characterize extent of osseous involvement by tumor.
Laboratory analysis is useful for infection, inflammatory arthritis, and blood tumors. C-reactive protein is the best measure of acute infection. Inflammatory arthritis may affect other joints (in particular knee and hand) and shows elevation of erythrocyte sedimentation rate. Complete blood count with differential screen for leukæmia.
A Back pain A simplified ætiologic algorithm.
Management
Idiopathic back pain is best managed according to general principles.
Establish the diagnosis by exclusion.
Educate and reassure the patient and family. Education may include a physiotherapist on modalities for back health.
Activity modification. Avoid what makes it worse, such as a back pack that is >15% body weight.
Light aerobic exercise, including participating in P.E.
Weight reduction and control.
Stretching. This may begin under the guidance of a physiotherapist but should continue as part of a more “holistic” approach, such as yoga.
Encourage “lifestyle” techniques that may be adopted by a child into adulthood, rather than medical interventions with which the child may not be compliant or which will be regarded as temporary. This is of particular importance because the majority of adolescents who complain of back pain and have a family history of such will experience back pain as adults.
Juvenile Idiopathic Arthritis
The majority of patients will be HLA-B27 positive (ANA and RF negative). Up to a third of patients with seronegative spondyloarthropathy will have a family history. Other characteristic signs include the following:
Schober test for spine stiffness. Forward bend is associated with <4 cm of lumbar spine excursion due to syndesmophytes.
Enthesitis, for example, at tendo-Achillis
Cutaneous stigmata, for example, psoriasis
Visceral involvement, for example, uveitis, enteritis
Management of back pain in this setting is secondary to management of the primary disease, by a rheumatologist.
Developmental Lordosis
Strain on facet joints in the hyperlordotic lumbar spine is a cause of back pain around the turn of the decade [B]. It is flexible, transient, and resolves spontaneously. Treatment consists of education and assurance, with postural training by antilordotic exercises.
B Physiologic lordosis of puberty This results from hyperflexibility of the lumbar spine as the trunk settles upon the pelvis.
DISCITIS
Discitis represents infection of the metaphysial region of a vertebra. By contrast with tumor, to which the intervertebral disc may be impervious, infection will traverse and erode the disc. The term places emphasis on the loss of disc height on röntgenogrammes [A].
Clinical Features
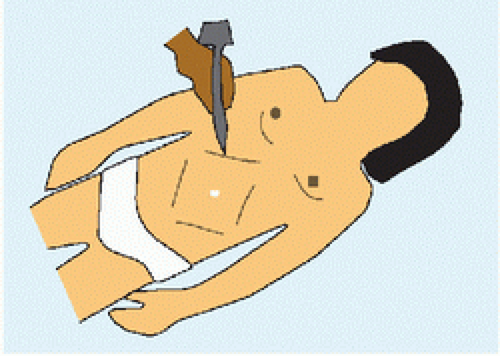
Presentation may be obscure and result in delayed diagnosis. It is one of the causes for refusal to walk in an infant. The preadolescent may complain primarily of abdominal pain; only in the second decade does the complaint reliably localize to the spine. Constitutional symptoms and signs, stiffness of the spine, and elevated inflammatory markers suggest the diagnosis. Paraspinous muscle splinting may be assessed in the prone position with the hips extended and the knees flexed: moving the pelvis from side to side causes a synchronous movement of the lumbar spine (Goldthwaite sign). Severe or untreated disease may be complicated by extension to paravertebral soft tissues, such as psoa abscess.
Imaging Röntgenogrammes take more than a week to show reduced disc height [A]. Scintigramme shows increased uptake of adjacent vertebrae at onset of disease [A] and will hasten diagnosis. MRI is indicated only if uncertainty persists, as it may introduce confusion with more morbid process such as tumor and lead to unnecessary intervention such as aspiration or biopsy.
Management
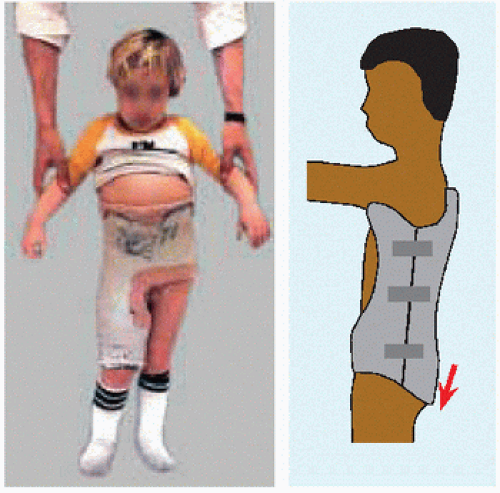
If the child does not present with systemic illness, immobilization alone in brace or pantaloon cast may be sufficient [B], while the spine, well vascularized, in a healthy child recovers spontaneously. Antibiotics may be added to shorten disease duration and avoid complications; they are indicated unequivocally in systemic illness. Regimen follows general principles for musculoskeletal infection.
Initially target gram-positive organisms.
Venous antibiotics for systemic illness and until the disease is controlled.
Conversion to oral antibiotics after clinical and laboratory response.
Continuation of treatment until normalization of ESR.
Change of antibiotics, further imaging, aspiration, or biopsy for atypical course or lack of response.
Prognosis
Disc recovery is inversely proportional to age at presentation [C]. Despite outcomes that include residual disc narrowing, sagittal plane deformity, and spontaneous fusion, function is not significantly impacted during childhood.
A L3-L4 discitis Scintigramme at presentation shows increased uptake (red). After 2 weeks, lateral röntgenogrammes shows narrowing of the disc (yellow).
B Immobilization reduces discomfort Most complete immobilization includes the back and one limb to immobilize the lumbosacral spine (left). A “long” (red) TLSO is better tolerated.
C Outcome of discitis Persistent loss of disc height and mild focal kyphosis 2 years after successful treatment.
Category
Comment
Idiopathic
Cause unknown Most common type Subdivided by age: infantile, juvenile, adolescent
Growth disturbance of anterior column leads to loss of sagittal contour until buckling lateralward and rotation
Serologic
Abnormality of platelets
B Causes of idiopathic scoliosis Scoliosis is multifactorial, and most cases are new spontaneous.
C Growth of the vertebral canal Volume doubles from birth (0) to 5 years of age, at which point volume is 95% of maturity (M).
Characteristic
Comment
Specific and sensitive
Nonspecific: normal variation in population Too sensitive: referral of untreated curves
Applied to at risk population
Applied to all children
Cost:benefit ratio
˜33% increased cost of management ˜0.2% indication for bracing
Early intervention alters natural history
Treatment effect of bracing difficult to quantify Manipulative and alternative modalities debatable
D Screening of scoliosis Essential characteristics of an effective screening test. Screening for scoliosis is recommended twice for girls and once for boys in the first half of the second decade.
SCOLIOSIS
Scoliosis is ancient. It is named and discussed extensively in the Hippocratic Corpus, including the scamnum for correction. It permeates Western literature and art: Shakespeare recounts how the Duke of Gloucester lamented his back, “Where sits deformity to mock my body.” While it is defined as angulation in the coronal plane >10 degrees, scoliosis is a three-dimensional deformity including rotation in the transverse plane and alteration of sagittal alignment. It may be divided into causative categories [A].
IDIOPATHIC SCOLIOSIS
Idiopathic refers to “disease” (Greek παθοζ) that arises on its “own” (Greek ιδιοζ), that is, cause unknown. Despite the name, several causes have been speculated [B]. Idiopathic scoliosis is the most common deformity of the back. It affects approximately 1% of children, approximately 90% of whom never require active treatment. Progression is proportional to growth, necessitating follow-up through maturity. It is defined as ≥5 degrees, and averages 1 degree per mensem during growth and 1 degree per annum after maturity for curves >50 degrees.
Evaluation
Essential to evaluation is exclusion of other cause, determination of growth potential, characterization of curve (including magnitude and flexibility), estimating risk of progression, and by extension likelihood of treatment.
History
Age. This is one measure of growth, which correlates with progression of deformity. Children in the first decade have a higher incidence of neuraxis lesion. Fusion arrests growth. Significant growth of the spinal canal concludes by 5 years of age [C], before which focal operation for vertebral anomaly should be postponed if possible in order to avoid stenosis. Clinically significant growth of the thoracic spine concludes as the child transitions into the second decade, by which point the 50% threshold of thoracic volume has been traversed and before which fusion will have a deleterious effect on pulmonary function.
Gender. Scoliosis affects both genders equally, but progression in girls is approximately five times than in boys.
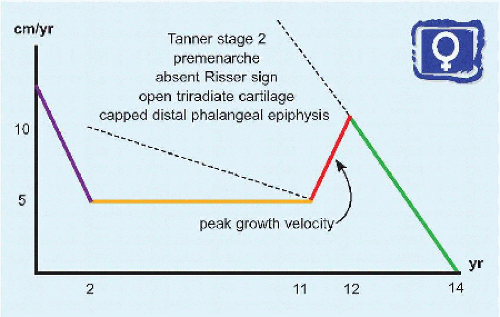
Other measures of growth. Growth amplifies deformity. Girls grow fastest in the 7 months before menarche and stop significant growth 2 years postmenarche. Menarche is variable, including according to activity and ethnicity. It occurs after peak growth velocity, that is, after the curve acceleration phase, the time of greatest risk of progression. It applies to only half of children. Boys grow later and less predictably, in particular a greater variability in cessation of growth.
Complaints. Pain traditionally has been underestimated in children, and in scoliosis in particular, where it affects 2/3 (twice the background rate). This may be related to fatigue of muscles attempting to rectify the spine. On the other hand, abnormal pain or other complaint (e.g., neural change) may be a sign that the scoliosis is not idiopathic.
Family. Such a history may suggest greater risk of progression. A susceptibility to develop scoliosis has been linked to the gene GPR126 on chromosome 6, which is highly expressed in cartilage and is associated with height and trunk growth.
Ethnicity. Caucasians are most affected.
Screening [D]. This developed from the observation that the thoracic spine and its deformity may be seen on röntgenogramme of the chest obtained during tuberculosis screening. It no longer is practised in the United Kingdom or Canada, and in only half the United States. Greater than 99% of referrals consist of normal variants, scoliosis <10 degrees (“schooliosis”) or <25 degrees (no treatment).
Physical examination Develop a standard approach, including the following:
Gait. This may indicate pain (antalgic), a generalized disease or associated findings (e.g., ataxia).
Maturity. Tanner scale of secondary sex characteristics has not been bettered by any other system [A]. It is the simplest, fastest, and cheapest method. It may be performed in office (not off-site) and is least morbid (e.g., no radiation from röntgenogrammes). Progression is greatest in the first two stages. Stage 3 coincides with menarche. Stage 4 marks end of significant spine growth. Plane of deformity. Examine coronal (from back and front), transverse (forward bend), and sagittal (from side) planes.
Palpation. For tenderness, step-off, crepitus, and including the paraspinous soft tissues.
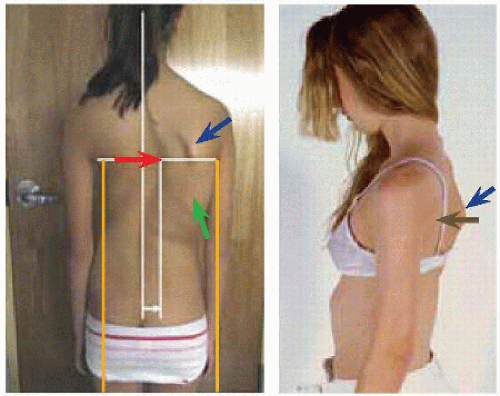
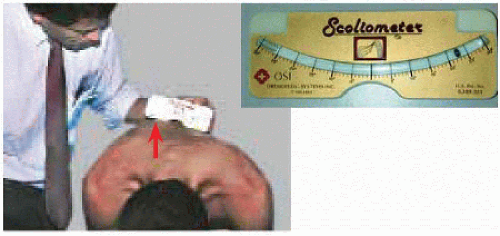
Trunk asymmetry, including the shoulder, scapula, rib, breast, flank, iliac crest. Asymmetry may be a secondary sign of spine deformity, or it may be a normal variant (5 to 15 mm). Correlate trunk asymmetry with other signs, including direct palpation of the spinous processes. Coronal curvature in the chest elevates the shoulder and below the chest will indent the flank [B]. Rotation will push the scapula, breast, and ribs out, which may be accentuated by sagittal plane deformity such as loss of thoracic kyphosis. Rotation is proportional to risk of deformity progression. Angle of trunk rotation may be measured on forward bending with a scoliometer [C].
Trunk shift [B]. Project the surface of thorax vertically relative to the iliac crests. This carries an increased risk of deformity progression.
Spine balance [B]. Even in the setting of trunk shift, a child with idiopathic scoliosis will bring the head back toward midline to balance it on the pelvis. Imbalance may be a subtle indicator of neural abnormality.
Spine motion, including Adams forward bend test. This is performed ideally from the front (not the back) so that the entire coronal contour may be evaluated by varying the degree of bend without changing the examiner’s position, as well as from the side. Asymmetry or limitation may be a sign of pain, neural lesion, or associated abnormality such as hamstring tightness.
Neural examination, including central signs such as altered gait, lower limb hyperreflexia, clonus, and abnormal abdominal reflex [D]. The latter is a superficial reflex for the thoracic spinal cord. Presence or absence is normal; asymmetry suggests a spinal cord lesion. It is explained evolutionarily as a mechanism to thicken the abdominal wall to protect subjacent viscera.
Other deformity. For example, in cavus, the arch may point to the primary problem (proximalward to the spinal cord).
Skin. Note the apothegm that “the skin tells the story.” Look for cutaneous signs of decompensation in the setting of deformity, such as stretch marks (rapidity of change in back shape) and callus (in response to unrelieved pressure due to lack of flexibility). Look for a midline stigma of underlying neural lesion, such as hairy patch or sinus. The former may be regarded as an early functional outcome sign, which may influence intervention. The latter is an indication for magnetic resonance imaging.
Laxity. Signs of hyperlaxity may be present, including elbow extension <0 degrees, placement of the thumb on volar forearm, extension of metacarpophalangeal joints >90 degrees, extension of the knee <0 degrees, flexion of the ankle >30 degrees, and the ability to place palms flat on floor during forward bending with knees straight. As an example, an increased incidence of private variants in fibrillin-1 gene, causing nonsynonymous amino acid substitutions, has been found in a subset (4%) of children with adolescent idiopathic scoliosis who present with more severe and more progressive curves, as well as hyperlaxity without other sign of Marfan syndrome (cf. Syndromes chapter).
A Tanner scale consists of five stages Distinctive and practical features. P: progression of spine deformity.
B Trunk asymmetry Apex dextrad curvature (red) produces a right posterior thoracic prominence (green) and scapular protraction (blue). The trunk shifts dextrad (orange) relative to the pelvis. Despite trunk shift, balance is maintained, as evidenced by a plumb line (white) dropped from inion to natal cleft. Sagittal alignment is changed as the thoracic spine rotates out of kyphosis (brown).
C Trunk inclination The scoliometer is grooved in its center to accommodate spinous processes as the examiner runs it continually along the entire spine. Observe inclination of a silver ball along a curvilinear slot marked in degrees.
D Abdominal reflex Stroke each quadrant of the relaxed abdomen. Reflex contraction of abdominal muscles draws umbilicus toward the stimulation.
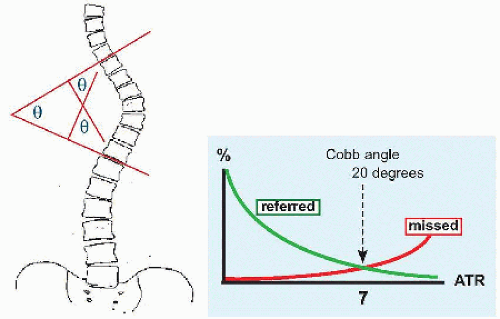
E Angles of Cobb and trunk rotation (ATR) Measure the maximum angle from end vertebra to end vertebra (θ). Draw a line tangent to end plates. Because lines may meet beyond field of view, draw orthogonal lines to obtain the angle. Missed rate begins to rise significantly after 7 degrees of ATR, equivalent to 20-degree Cobb angle.
Sign
Comment
Risser
Divide iliac apophysis into quarters 1-4; fusion of apophysis is 5.
Most progression occurs before appearance of iliac apophysis.
Triradiate cartilage
Closed marks cessation of spine growth. Open allows no differentiation of maturation stage.
Distal phalangeal epiphysis
Capping of distal phalanges by epiphysis marks beginning of curve acceleration phase. Fusion marks end of significant progression. Fusion coincides with menarche, triradiate closure, absent Risser.
Tanner-Whitehouse RUS
Complex method based upon multiple sites in radius, ulna, and small bones of the hand.
Selection of distal phalangeal epiphysis is a simplification.
F Radiographic signs of maturity This is in constant flux. Risser noted that the iliac apophysis could be seen serendipitously at the bottom of spine röntgenogrammes. Evaluation of the distal phalangeal epiphysis is the current favorite method.
G Growth curve for a girl Note the features associated with peak growth velocity, during which the spine goes through the curve acceleration phase.
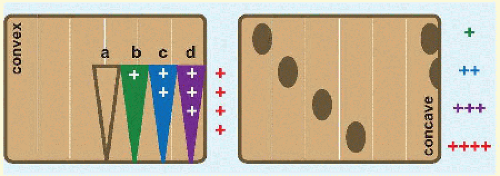
H Vertebral rotation This may be graded according to location of spinous process and of pedicles as viewed in coronal plane. Beyond d, or grade ++++, spinous process projects beyond vertebral body. In grade +++ and ++++, concave pedicle has disappeared.
Imaging Röntgenogrammes are the foundation. Measure curve magnitude in degrees after the method of Cobb [E]. Note that measurement error is approximately 5 degrees, which has not been improved by digital imaging. In order to reduce referrals for which orthopædic management is not indicated, a minimum of 7 degrees on scoliometer has been identified to correspond with a Cobb angle of 20 degrees.
Obtain full-length röntgenogrammes to determine spine balance. Sagittal balance is represented by a vertical line between midpoint of C7 and superoposterior corner of S1. In the coronal plane, this vertical line should pass through S1 spinous process. Imbalance is measured in centimeters: ≤2 cm is within normal range.
Posteroanterior projection reduces breast exposure to radiation, which, after reflection of its majority off the skin, declines with travel through tissue, reaching the breasts last. Shield the breasts when it does not impact analysis of the deformity. Include the clavicles to assess shoulder height, which influences operative technique and outcomes. Include the iliac apophysis and triradiate cartilages to aid determination of maturity [F]. Add röntgenogramme of the hand for evaluation of the distal phalangeal epiphysis. Note that calculation of maturity is nuanced and multifactorial [G]. The iliac crests also allow assessment of limb length discrepancy.
Röntgenogrammes identify stable and neutral vertebrae. The former is bisected by the central sacral line. The latter show no rotation, defined as symmetric pedicles and midline spinous process [H]. Rotation is a risk factor for progression and must be considered in addition to curve magnitude. The apical vertebra is least stable and most rotated. Limit fusion to vertebrae that at least are crossed by the central sacral line. Pedicle screws have promoted fusion before reaching the neutral vertebra, because of direct vertebral rotation.
Determine flexibility on röntgenogrammes. Prone posteroanterior view simulates the operating room. Bending views will show opposite inclination at flexible discs, which may be spared fusion. Bending views also show whether the planned lowest instrumented vertebra can become <15 degrees oblique (greater associated with progression) and enters the stable zone.
Computed tomography is useful for complex osseous architecture. In idiopathic scoliosis, this applies to severe deformity rather than vertebral anomaly, which is not a feature. CT provides detail in the postoperative spine, for example, for pseudarthrosis. CT with myelogramme evaluates the instrumented spine for vertebral canal encroachment, for example, by implants in the setting of neural compromise. For other neurologic evaluation, myelography has been replaced by magnetic resonance imaging. Pedicle dimensions may be measured on CT to aid operative planning.
Magnetic resonance imaging is indicated when an abnormality of the neuraxis is suspected in the so-called “idiopathic” setting. Principal risk factors are as follows:
abnormal physical examination
age <10 years
kyphosis >40 degrees for thoracic curves
There is debate about association between neural lesion and other signs of atypia, such as apex left thoracic curve, rapid progression (moderate estimate >3 degrees per mensem), male gender, dystrophic curve (short and sharp, Harrington factor >5 degrees/segment), or otherwise unusual appearance curve (e.g., long and sweeping akin to a neuromuscular presentation).
Classification
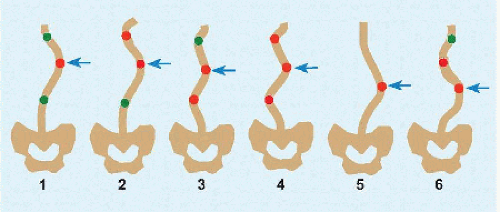
Morphologic Curves are divided into six types [I]. Main refers to a structural thoracic curve in the setting of an upper structural thoracic curve. Major refers to a structural curve when thoracic and lumbar regions are affected independently, and the largest of two or three structural curves. Nonstructural refers to a compensatory curve that may be spared fusion.
Triple major. Two thoracic + thoracolumbar/lumbar structural curves.
Thoracolumbar or lumbar curve.
Thoracolumbar or lumbar + thoracic structural curves.
Thoracic curves are modified based upon kyphosis:
– hypo-, defined as <10 degrees
N, normal
+ hyper-, defined as >40 degrees
Lumbar curves are modified based upon whether central sacral line:
A bisects the apical pedicles.
B touches apical vertebral pedicles.
C is medial to the apical vertebra.
Classification applies order based upon pattern recognition, but variability argues against dogma. An alternative is the descriptive approach.
Curve magnitude. This is defined in the coronal plane. Sagittal plane is most predictive of functional outcome. Appearance is most influenced by rotation in the transverse plane.
Type of curve. This is a geographic assessment based upon location of apical vertebra: thoracic, which may be single or double (termed main and upper); lumbar; combined thoracic and lumbar; and thoracolumbar (T12-L1 apex).
Flexibility of curve. This is based upon intervertebral disc inclination. Discs that are inflexible are part of a structural curve. Flexible discs are part of what may be a compensatory curve that rectifies or does not progress upon treatment of the structural curve and as such may be spared direct treatment. Curves flexible to <25 degrees also may be excluded.
Relation to midline. A curve that crosses the midline is structural. A curve that is returning to the midline from a structural curve, for example, the lumbar spine returning to the pelvis, represents compensation by the flexible spine.
Sagittal contour. Thoracic curves may be associated with hypokyphosis, lordosis, or hyperkyphosis. This is more difficult to correct than coronal curvature. Increased power of instrumentation exposes anterior overgrowth and loss of thoracic kyphosis with increasing coronal correction. Sagittal contour is essential to determination of end instrumented vertebrae. Sagittal balance correlates more directly with functional outcome than coronal balance. Hyperkyphosis of the thoracic spine may be the most sensitive predictor of associated neural lesion.
Coronal and sagittal balance. Imbalance is associated with poor functional outcome, most in the sagittal plane.
Rotation in the transverse plane. This is predictive of progression, in addition to curve magnitude. It may serve as an alert that a flexible curve may not be compensatory.
Atypia. This may be an indication for MRI of the neuraxis.
I Classification of scoliosis—morphologic Fusion is indicated for structural curve, represented by red. Green signifies a compensatory curve that may be spared. Main and major curves are structural and largest (blue).
Type
Comment
Infantile <3 years
<5%
Boys 2 times girls
Most thoracic curves apex left
Extrinsic cause suggested by associated “packaging” signs including torticollis, plagiocephaly, hip dysplasia
Resolving or progressive—calculate Rib-Vertebral Angle Difference and Phase
Juvenile 3-10 years
High rate of associated neural lesion ≤1/3
High rate of progression ≤2/3
Adolescent >10 years
>80% of all cases
J Classification of scoliosis—clinical Three types are distinguished according to age.
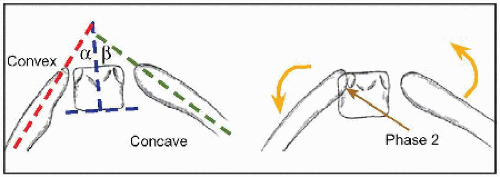
K Rib-vertebral angle difference (RVAD) and phase Determine angle subtended by the axis of the rib (red, green) and vertical axis of the body of the apical vertebra (blue). RVAD = α – β. The difference results from hinging of the ribs as the spine curves away from the convex set toward the convex set. Greater than 80% of curves with RVAD <20 degrees will not progress. RVAD >20 degrees is associated with >80% progression.
On the right, the curve is in phase 2, which is defined as overlap of the convex rib head with apical vertebra (brown) and in which progression is certain. Such a curve is termed “progressive” type. Phase 2 is a manifestation of rotation displacing the apical vertebra anterior to the apical rib so far that the overlap becomes radiographically visible even in the incompletely ossified skeleton. Phase 1, exemplified by the figure on the left, is defined as no overlap: such curves do not progress and are known as “resolving.”
Clinical Idiopathic scoliosis may be classified according to age [J].
INFANTILE This is rare and distinct from juvenile, which may be considered a graver form of adolescent. It may be divided into two types: resolving and progressive. The former is unique in potential for spontaneous correction, which along with associated packaging signs suggest a unique cause, at least for this subgroup. Progression may be predicted by the rib-vertebra angle difference and phase [K].
JUVENILE This is distinguished by a high rate of associated neural lesion (up to 1/3) and the highest rate of progression (up to 2/3). The former is an indication for MRI of the neuraxis. The latter adds urgency: more patients will require treatment, earlier and more aggressively.
Natural History
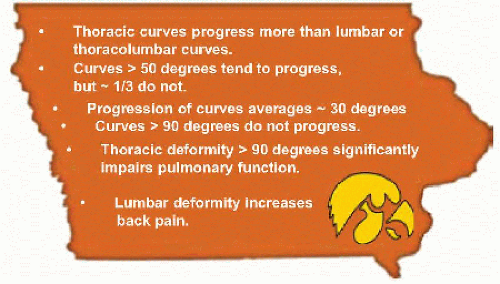
Understanding of natural history is founded in the classic studies from the University of Iowa [A]. While they are revered due to their 50-year follow-up, which is unrivaled in orthopædic surgery, there is not absolute clarity.
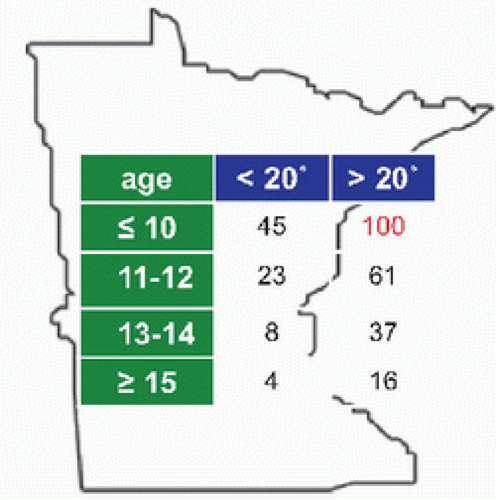
Progression The principal determinants of progression are growth and curve magnitude. Risk of progression to surgery is what patients and parents most want to know. Progression has been the most consistent outcome measure in the literature of idiopathic scoliosis. Deformity has the potential to progress during growth. All juvenile idiopathic scoliosis >20 degrees progresses [B]. If the threshold of 30 degrees is crossed in the first decade, scoliosis will progress beyond 50 degrees (to fusion) despite nonoperative treatment (bracing).
Pulmonary function This is the principal concern of thoracic scoliosis. Curve magnitude, location, and rotation conspire to produce pulmonary disease, of which essential features are spinal encroachment upon thoracic viscera, reduced thoracic dimensions, and disruption of mechanics of ribs and respiratory muscles (intercostal and diaphragm). Alveolar and pulmonary vascular hyperplasia cedes to hypertrophy toward the end of the first decade, as growth moves from increasing numbers to increasing size of preexisting structure.
Diminution in pulmonary function testing, in particular total lung capacity and forced vital capacity as measures of restrictive lung disease, may be observed at 60 degrees of scoliosis. Clinically apparent pulmonary dysfunction, such as dyspnœa on exertion and sleep hypopnœa or apnœa, occurs at 90 degrees. Spine fusion with instrumented correction of deformity in idiopathic scoliosis may arrest pulmonary decline or even improve function by up to 10%. By contrast, costal osteotomy or thoracotomy, for example, for anterior approach, may reduce pulmonary function by a similar amount, although the effect may be temporary.
Back pain This is the principal concern of lumbar scoliosis. Back pain affects 2/3 of children with scoliosis. It is related to fatigue of muscles resisting progressive deformity and imbalance. Spine fusion reduces pain but not for every patient and not always completely. Longterm pain is related to degenerative changes at facet joints and intervertebral discs that are malaligned (abnormal force vector) or spared fusion (force concentration). Untreated severe scoliosis is associated with increased pain quantitatively; for example, in the Iowa experience, it occurred “frequently or daily” 50% more than controls. There is a qualitative increase in back pain as well, such as less physically demanding employment and more frequent disability claims. Controversy and lack of further granularity remain, in large part due to the difficulty of measuring an effect when back pain is so prevalent in the general population.
A Natural history of scoliosis The Iowa experience.
B Progression is influenced by growth and curve magnitude The Minnesota experience drew attention to the at-risk group of juvenile scoliosis with significant curvature. This has been refined to progression in <10 years of age >30 degrees to severe deformity and fusion.
Appearance The Iowa studies noted that untreated patients with scoliosis were more self-conscious of appearance. For surgically treated patients, the Spinal Appearance Questionnaire and the Scoliosis Research Society Appearance domain show large effect size, demonstrating that they are sensitive enough to measure treatment effects. By contrast, Scoliosis Research Society Activity, Pain and Mental domains show small effect sizes and standardized response means, demonstrating an immeasurable effect on these functional outcomes by operation. Appearance matters, both to patients and because it is the factor most effectively treated.
Management
The pillars of management are education, observation, bracing, and surgery. Education is all encompassing. For example, educate parents that “doing nothing” by observation is a legitimate form of treatment, as most curves do not progress significantly and as such do not cause long-term disability. Patient characteristics that drive management are curve magnitude and age.
Observation 10 to 30 degrees Obtain röntgenogrammes every 6 months through maturity.
Bracing 30 to 50 degrees Institute at 25 degrees for the high-risk child, in particular in the first decade. This is the standard of care for the growing skeleton. The principle that underpins bracing is application of contralateral forces through the ribs or flank against the limbs of the spine on either side of the apex. The multiplicity of braces and regimens exemplifies the axiom that permeates surgery: “Where there is variability there is uncertainty.” The Boston brace as well as full-time wear (as opposed to night time) have the broadest experience [A]. While a curve may be corrected in a brace, success of bracing is defined as arrest of progression. Factors associated with brace failure include thoracic lordosis, high thoracic apex, obesity and poor compliance, as well as curve >30 degrees in the first decade.
Custom brace fabrication to the patient and röntgenogramme.
Wean to full-time wear, defined as >20 hours per diem.
Doff brace day before serial follow-up röntgenogrammes.
Don brace until maturity.
Such treatment at such a critical developmental period carries a psychosocial cost that, while difficult to measure (unlike, e.g., angle of scoliosis), is real and may endure after cessation of active care.
Casting 30 to 50 degrees This is indicated for infantile idiopathic scoliosis. Serial casts are applied every 2 to 4 months from 2 to 4 years of age under general anæsthesia. Reduction of spine deformity is based upon derotation as opposed to direct force. Distinctive features of the cast include minimal padding, stable purchase on the pelvis as the foundation, and windows to allow for dynamic correction. Success is defined as continual curve correction to resolution (cure), arrest of progression that is maintained by casting followed by bracing, or delay of operation. Assessment of efficacy is impacted by limited experience given rarity of condition, uncertainty about natural history, as well as significant intra- and interobserver error in RVAD and phase determination.
Operation 30 to 50 degrees fusionless Patients in the first decade with a curve >30 degrees, and premenarcheal girls with curves >40 degrees, have a high likelihood of progression to fusion despite bracing. In the former group, fusion in the first decade limits growth of the spine and thereby reduces thoracic volume enough to negatively impact clinical pulmonary function. The latter group is approaching the magnitude for fusion with significant growth remaining, including the curve acceleration phase before menarche. For these groups, operation is an alternative. The goal of fusionless surgery is to tether the convexity of a curve, which is growing more rapidly. This may arrest progression (as an internal brace) or allow for correction with concave growth, at which point the tether may removed. The latter distinguishes this modality from bracing.
Growth modulation by physial tethering is well established, in particular at the distal femur and proximal tibia for genu valgum et varum. Application of the technique in the spine differs in that implants are placed between bones across a motion segment, which theoretically increases the risk of failure. There are two types of fusionless operations, performed by telescope or open on the anterior spine, which may restore kyphosis in the thoracic region but has the potential to reduce lordosis in the lumbar region. As with genu valgum et varum, implant removal is indicated if there is anatomic correction.
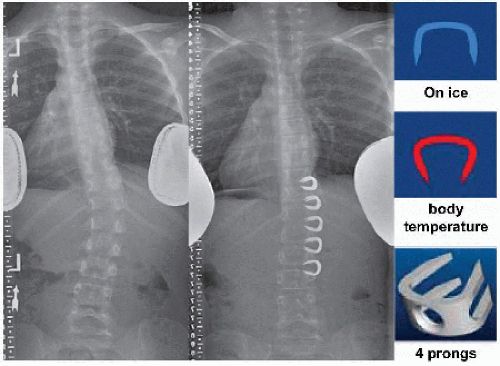
VERTEBRAL BODY STAPLING [B] This is indicated for juvenile idiopathic scoliosis 30 to 39 degrees. Vertebral end plates and intervertebral discs are spanned by a two- or four-pronged NiTiNOL staple, which is inserted ice-cold and with straight tines that return to the original curved shape as the memory metal warms to body temperature. The innovation of curved NiTiNOL has eliminated the complication of staple back out. The procedure has the advantage of sparing the intercostal vessels, which may be mobilized away during insertion of, and rest between, staples.
SCREW AND CORD [C] The ideal candidate is a child with a curve 40 to 60 degrees and having more than 2 years of growth remaining. The latter may be estimated as premenarche in a girl and no facial hair in a boy, or according to the arithmetic method as under 12 years for a girl and under 14 years for a boy. Other measures of significant growth potential include open triradiate cartilage and no Risser sign.
Hydroxyapatite coating of vertebral body screws is designed to reduce pullout. Screw insertion requires intercostal vessels ligation. Washers support screw fixation. A flexible polyester cord fixed to the screws is tensioned to effect a partial reduction and resist convexity growth.
A Boston brace Thoracolumbosacral orthotic (TLSO) is custom fabricated based upon patient shape and röntgenogramme from hard plastic lined by dense foam with pads placed according to morphology of curve. It opens in the back (green), is indented to fit the waist above the iliac crests, and includes opening (orange) and greater trochanteric extension (red) to allow three-point bend. Note that the highest extension is axillary (pink) reducing effectiveness for curves with apex above T6.
Wean to full-time wear, defined as >20 hours per diem. Doff brace day before serial follow-up röntgenogrammes. Don brace until maturity.
B Vertebral body stapling Correction in 7-year-old girl with 32-degree thoracolumbar curve. NiTiNOL (NIckel-TItanium Naval Ordnance Laboratory), a memory metal, has eliminated implant back out.
C Screw and cord Correction by tethering the convex side of the spine, which is growing more rapidly. While overall correction is complete, segmental correction varies because segmental growth – normal and asymmetric – is variable.
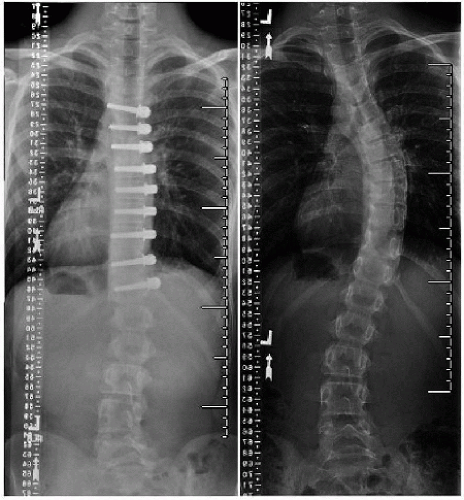
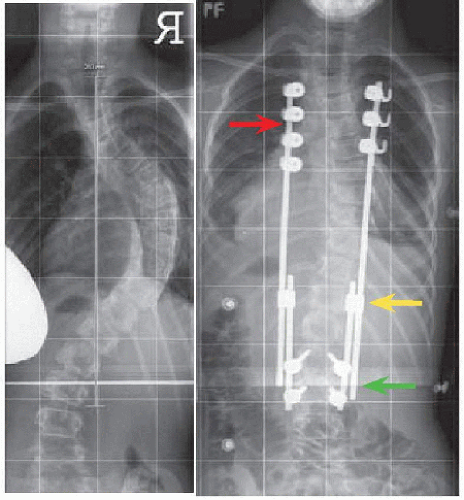
D Growing rods A 7-year-old girl with 75-degree thoracic curve. Two rods and pedicle screws at a lower end fusion (green) improve stability. Modification of upper anchors to the ribs (red) increases number of anchors at flexible sites and reduces spine dissection, potentially reducing implant failure and fibrosis. Use of standard implants lengthened at side-side connectors (yellow) simplifies index procedure and procedure at maturity.
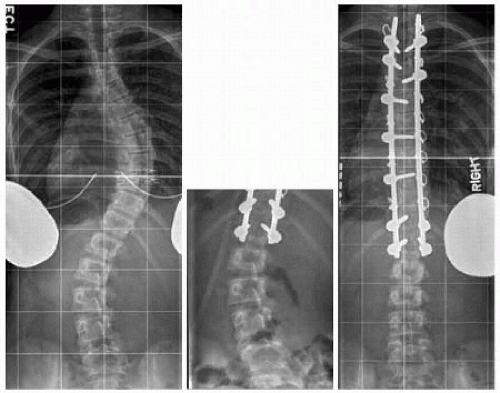
E Selective fusion The lumbar curve was spared because it was flexible <25 degrees. Early residual curvature spontaneously corrected by 1 year. Transverse process wires at the top instrumented vertebra avoid interference with superjacent facet joints and midline dissection. Screws at the ends reduce construct pullout. Apical screws aid reduction of deformity. There are two anchors at every level, including transverse process wires that are safe and cheap.
Principle
Comment
Structural curve
Fuse.
Compensatory curve
Bending röntgenogrammes show opposite bending of intervertebral discs and curve <25 degrees. Spare.
Stable vertebra
Each end vertebra must be crossed by center sacral line.
Neutral vertebra
Pedicle screw instrumentation may shift this by vertebral derotation to limit fusion.
Sagittal contour
End vertebrae must be out of kyphosis.
Rotation
May represent a structural component independent of coronal magnitude or flexibility
Shoulder height
Extend fusion proximalward in order to pull down a shoulder elevated opposite apex of thoracic curve.
Thoracolumbar junction
T12 lowest instrumented vertebra associated with increased risk of junctional kyphosis-stop at L1
Obliquity
Obliquity of lowest instrumented vertebra >15 degrees may be associated with progression and poor long term outcome.
F Selection of fusion levels
Operation >50-degree fusionless Indication for fusionless operation is juvenile scoliosis having curve magnitude too great for vertebral body stapling or screw and cable.
GROWING RODS [D] This is the original fusionless operation. The goal is deformity correction and its maintenance while allowing growth of the spine. It is mechanically disadvantaged: end fixation with intervening motion fails approximately 15% of the time. Advances to enhance stability include the following:
Two contoured rods with or without cross-links, compared with one straight rod
End fusion of two vertebrae, compared with anchoring to a single vertebra at each end
Pedicle screws, compared with laminar hooks
Unlike vertebral body stapling or screw and cable, which rely on spontaneous growth of the concave spine, growing rods lengthen the spine by active distraction. It is biologically disadvantaged: after implantation and initial distraction (which achieves the most elongation), the rods are distracted every 4 months through the same incision. Repeated opening of a scarred wound results in an infection rate up to 10%. Multiple procedures, prolonged instrumentation, and infection lead to fibrosis, possible heterotopic ossification, and stiffening of the spine. At maturity, or as close as is reasonable based upon patient tolerance of multiple procedures and complications, definitive fusion is performed.
Only gold members can continue reading. Log In or Register to continue