51
Ulnar Collateral Ligament Injuries: “Skier’s Thumb”
Kevin D. Plancher
History and Clinical Presentation
A 24-year-old left hand dominant woman presents with a swollen and painful left thumb. While skiing the patient felt a sharp pain in her thumb at the metacarpophalangeal (MP) joint when she put her hand out to stop her fall. She recalls her thumb landed in an outstretched fashion in the snow and was pulled backward and out of the palm. She is unable to use her thumb secondary to pain. She denies any previous history of trauma to her hand or thumb.
Physical Examination
The patient demonstrated tenderness along the ulnar collateral ligament (UCL) of the MP joint of the thumb. She has localized swelling and ecchymosis. Stress testing without lidocaine of the UCL at both full extension and flexion resulted in 35-degree laxity without an end point, and greater than 15 degree difference from the noninjured contralateral side (Fig. 51–1A,B). No crepitus with joint motion can be detected on physical examination.
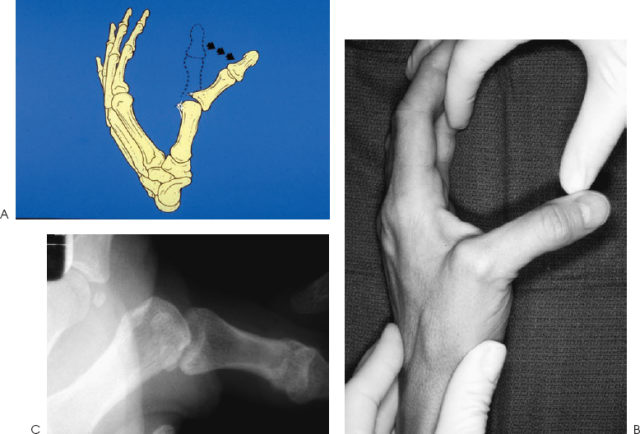
Figure 51–1. (A) Torn ulnar collateral ligament (UCL) of the thumb. (B) Physical exam of incompetent UCL. (C) Corresponding x-ray of incompetent UCL.
PEARLS
- Delay in treatment beyond 3 to 5 weeks promotes instability even with secondary procedures.
- Volar subluxation on the lateral x-ray may be the only clue to this injury.
- Physical exam may show a supinated digit as the only clue to this injury.
- Chronic reconstructions with palmaris longus has conflicting reports in the literature, while an MP fusion for a laborer may be a better alternative.
Diagnostic Studies
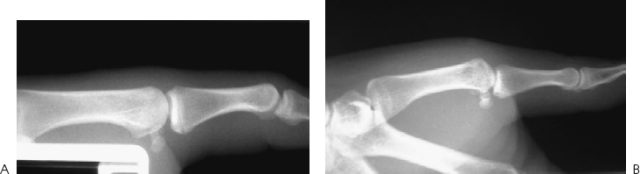
Radiographs, Robert’s view, anteroposterior (AP), and lateral, were obtained, and no fracture was seen in the thumb column. Lateral x-ray revealed volar subluxation of the MP joint (Fig. 51–2), and the stress testing under fluoroscopic guidance reveals abduction of the MP joint without an end point (Fig. 51–3). Local anesthetic may be necessary for accurate stress radiographs if pain is intolerable. An injured thumb that demonstrates more than 30 degrees of instability compared with the contralateral and uninjured side indicates a complete UCL rupture.

Figure 51–3. (A) Stress testing in a normal UCL. (B) Stress testing in a grade III UCL tear.
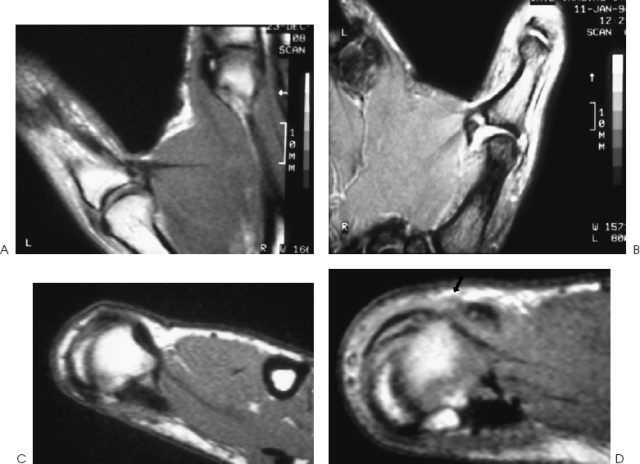
To differentiate between nondisplaced UCL injuries and the presence of a Stener lesion, magnetic resonance imaging (MRI) is helpful because it is both sensitive and specific for this soft tissue injury (UCL). The use of MRI facilitates a more accurate diagnosis and allows the physician to recommend the most optimal course of treatment for each case. The MRI is effective in distinguishing displaced versus non-displaced acute UCL lesions with or without the presence of a Stener lesion. This information is crucial in determining treatment. If a patient has a grade III UCL tear, yet no Stener, one might argue that nonoperative treatment is sufficient with casting. The MRI takes only 20 minutes and is cost efficient (Fig. 51–4).
PITFALLS
- Careful dissection over the SRN will avoid permanent numbness to the inside of the thumb.
- Inadequate conservative treatment and lack of identification of the Stener lesion can lead to instability and require fusion of the MP joint.
- Patients can have stiffness after this injury.
Differential Diagnosis
Radial collateral ligament injury to the MP joint of the thumb
Ulnar collateral ligament injury to the MP joint of the thumb
Fracture of the MP at a carpalphalangeal joint of the thumb
Dorsal capsule avulsion
Superficial radial nerve neuropraxia
Carpometacarpal arthritis
Volar plate injury to the MP joint
Dorsal capsular disruption of the MP joint
Diagnosis
UCL Injury to the MP Joint of the Thumb
An injury to the first MP joint can easily be overlooked in traumatic falls. The injuries to the collateral ligaments and subsequent dislocations can initially appear normal on x-ray. The patient usually describes a mechanism that consists of a sudden valgus force being applied to the MP joint of the thumb. This mechanism may cause disruption of the UCL, and if the joint is left unstable and untreated, a skier’s thumb leads to early degenerative joint disease of the first MP joint (Fig. 51–5).
The incidence of UCL injuries ranges from 35 to 80% of all upper extremity injuries, and is presently the most common upper extremity injury in snow skiing. The most common site of the UCL disruption is at its origin or insertion; however, midsubstance or proximal tears are also possible. Other injuries to the MP joint of the thumb to be aware of are avulsion fractures, dorsal capsular tears of the MP joint, and volar plate injuries.
In 1962, Stener described the interposition of the UCL caught and retracted between the bone and adductor aponeurosis. When the UCL ruptures, a tender palpable prominence may be noted over the ulnar aspect of the MCP (Fig. 51–6). Heyman et al determined that an MP palpable mass was 100% sensitive for the diagnosis of a Stener lesion, but only 46% specific in a prospective clinical study. Determining if a soft or firm end point is present is essential in the diagnosis and grading of UCL tears. This part of the physical exam must be coupled with other tests, such as stress radiographs and an MRI, if necessary, to have the most accurate and specific diagnosis.





