76
Radial Deficiency (Radial Clubhand)
Alexander D. Mih
History and Clinical Presentation
A 4-month-old girl was seen for evaluation of right upper extremity deformity. She was the product of a full-term delivery to a 30-year-old mother. The mother recalls no specific problems with pregnancy or medication requirement. There was no family history of orthopaedic problems. The patient’s history included a known ventricular septal defect.
Physical Examination
The patient’s right upper extremity was remarkable for an elbow with a fixed contracture at 20 degrees, a shortened right forearm compared with the uninvolved opposite side, severe radial deviation at the level of the wrist, and absent thumb.
No passive motion of the elbow was present. The wrist was passively correctable to neutral in the radioulnar plane as well as to 10 degrees extension in the anteroposterior plane.
Radiographic Findings
Radiographs of the upper extremity showed a reduced ulnohumeral joint with the complete absence of the radius. The carpal bones were deviated 70 degrees from the long axis of the ulna, with the capitate ossification center found directly radial to the end of the ulna. There was complete absence of the thumb metacarpal and phalanges (Fig. 76–1).
Differential Diagnosis
Radial clubhead
Transverse deficiency
Ulnar deficiency
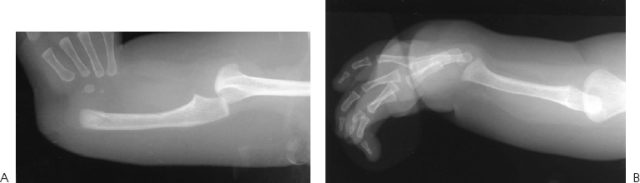
Figure 76–1 (A) Anteroposterior radiograph of wrist showing radial deviation and complete radial absence. (B) Lateral radiograph of wrist showing flexion deformity.
Diagnosis
Radial Clubhead
This patient shows complete absence of radius with the frequently associated findings of an elbow contracture combined with complete absence of the thumb. The diagnosis is radial longitudinal deficiency.
Radial longitudinal deficiency is seen in ∼1 in 50,000 births. This condition is seen more often in males than females and is bilateral in almost 50% of the cases. Classification of this deformity is as follows: type I, short distal radius; type II, hypoplastic radius; type III, partial absence of radius; type IV, complete absence of radius. The type IV deficiency is the most common. Radial longitudinal deficiency occurs frequently in association with other malformations involving the cardiac, gastrointestinal, pulmonary, genitourinary, neurologic, and skeletal systems. Syndromes that involve radial longitudinal deficiency include Fanconi’s anemia, the thrombocytopenia absent radius syndrome, the Holt-Oram syndrome, and the VATER association (vertebral defects, imperforate anus, tracheoesophageal fistula, and radial and renal dysplasia).
In this disorder, the preaxial muscles along the radial aspect of the forearm are severely affected or absent. A common flexor/extensor carpi radialis may be found and provides a significant deforming force. Although the ulnar artery is present, the radial artery is usually absent. The radial nerve is also absent with an anomalous branch of the median nerve often found to be a tethering structure when surgery is performed.
PEARLS
- Partial carpal bone excision to achieve wrist reduction is preferable to excessive pressure on the distal ulnar physis. In some cases the lunate may require complete excision. Complete radial-side soft tissue release is necessary for reduction. The radial-side Z-plasty may be required in cases of inadequate skin, with redundant skin excised from the ulnar side of the wrist.
PITFALLS
- Although some authors have not recommended wrist reconstruction in these patients, it is possible to achieve elbow flexion through triceps lengthening and capsulectomy. Pins should be cut off beneath the skin to allow more prolonged retention, and ulnar osteotomy may be required in cases of severe bowing.
Surgical Management
At age 6 months the patient underwent surgery for correction of the elbow contracture as well as wrist deformity. With the patient supine on the operating table and the arm on a short-arm board, a general anesthetic was administered. A sterile tourniquet was utilized with elevation to 200 mm Hg.
The elbow was approached through a straight midline incision directly over the triceps. The ulnar nerve was identified and retracted. The triceps was Z lengthened using a step-cut technique and a posterior elbow capsulectomy was performed. This allowed passive motion of the elbow to 120 degrees of flexion. The triceps was then reapproximated using nonabsorbable sutures.
The wrist was approached through a gently curving incision, which allowed exposure of the distal ulna. A capsulotomy was performed to allow reduction of the carpal bones over the end of the ulna under direct vision. Radical radial soft tissue release was required. The nonossified lunate could be reduced on the end of the ulna without pressure. A conjoined flexor and extensor carpi radialis tendon was identified and was detached from its insertion into the radial soft tissues and transferred to the ulnar side of the wrist, where it was sewn into the extensor carpi ulnaris tendon. A single 2.0-mm Steinmann pin was advanced retrograde through the end of the ulna and out the ulnar shaft. It was then advanced antegrade into the index metacarpal to achieve radialization. The Steinmann pin was cut off and advanced beneath the skin but left prominent to allow for removal at a future date (Fig. 76–2).
Postoperative Management
The patient was placed in a long-arm cast with the elbow at 120 degrees of flexion. The cast was extended the entire length of the forearm to include the hand. Immobilization was continued for 3 months using a thermomold splint.





