24
Arterial Aneurysms
Kevin D. Plancher
History and Clinical Presentation
A 38-year-old left hand dominant woman is seeking treatment for a tender mass in the palm of her hand. The patient had fallen with a glass bottle in her hand 2 weeks earlier and had sustained a puncture wound to the ulnar aspect of her right palm. At that time active arterial bleeding persisted despite direct pressure on the wound with a compressive dressing. She was originally treated in the emergency department with irrigation and exploration with cauterization of a “superficial” vessel and wound closure.
Physical Examination
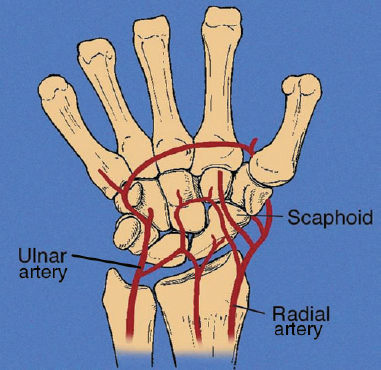
Removal of her sutures of the skin resulted in pulsatile bleeding from the wound. The bleeding continued despite direct manual compression on the wound (Fig. 24–1). Manual compression of the ulnar and radial arteries individually at the wrist crease did not stop the bleeding. Bleeding only ceased with manual compression of both arteries. The Allen’s test was performed and found the ulnar artery not patent. The color of the hand when performing the Allen’s test, to the ulnar side of the wrist, showed lack of perfusion to the radial side of the wrist (Fig. 24–2).
PEARLS
- Use of a tourniquet and appropriate anesthesia for adequate visualization and microscopic dissection of the artery
- Meticulous microscopic dissection with tension-free anastomosis
- Postoperative supervised therapy and appropriate incision care
PITFALLS
- Vein graft selection too small
- Inadequate graft length or anastomosis sewn under tension
- Failure to maintain proper graft orientation
Diagnostic Studies
Radiographs of the patient’s hand were obtained. Doppler flow assessment, pulse volume recordings, and angiography were also obtained. Angiography provided definitive information regarding the location and extent of arterial injury (Fig. 24–3).

Figure 24–1. Manual compression of the wrist with a saturated dressing in the patient with persistent bleeding.
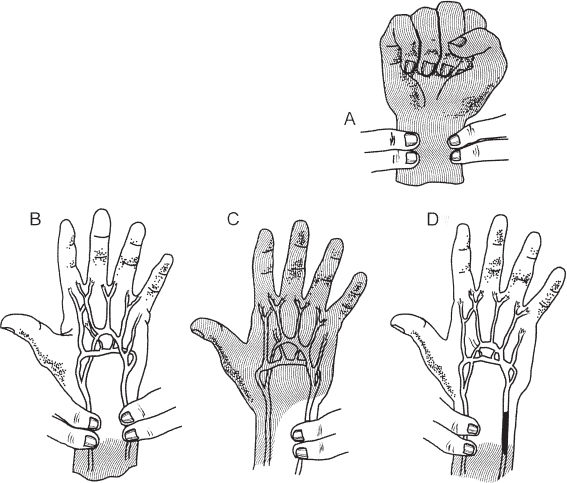

Figure 24–3. (A) Arteriography of the forearm and digital subtraction angiography of the palm. (B) Close-up view of the palm.
Differential Diagnosis
Ganglions
Nerve tumors
Other soft tissue masses
Raynaud’s disease
Pseudoanerysm of the palm
Diagnosis
Pseudoaneurysm of the Palm
Aneurysms are classified into two groups: traumatic and nontraumatic. Traumatic aneurysms can be subgrouped into true and false aneurysms. True aneurysms occur after blunt trauma to the upper extremity. These arise from occupational hazards, thoracic outlet syndrome, or a malignancy. Damage occurs to the arterial wall media to cause vessel dilation.
False aneurysms occur from a penetrating arterial injury or from a complete rupture of the vessel wall when continuity is maintained by the surrounding soft tissue. Hemorrhage from the vessel forms a contiguous hematoma that forms a fibrous shell adjacent to the vessel. Stab wounds, gunshots, and displaced fractures, or recurrent bleeding from hemophilia are all causes of a false aneurysm. Other causes of a false aneurysm include arterial punctures from blood gas analysis, cannulation of a vein or axillary arterial injury during a brachial plexus injection, as well as unrecognized arterial bleeders during operations. Diseases associated with peripheral aneurysms include Kawasaki’s syndrome, Buerger’s disease, and hemophilia.
Nonsurgical Management
While the patient is waiting for results of clinical tests, several nonsurgical options are available. The patient may be prescribed a vasodilator for partial obstructions to a blood vessel. Nitropaste placed on the finger or affected site has also been used, as has sublingual nifedipine. Surgery is indicated if symptoms persist and survival of the finger or hand is in question.
Surgical Management
Treatment of upper extremity aneurysms consists of exploration, resection, and vascular reconstruction depending on the location and type of aneurysm. The most common true and false aneurysms reported to date are the ulnar artery aneurysms. The redundant artery allows for an end-to-end repair. Digital artery aneurysms are rare. In the absence of ischemic signs, when an arterial thrombosis is present in a digit, ligation rather than reconstruction is the treatment of choice (Figs. 24–4 and 24–5).
The patient was administered general anesthesia and the arm was exsanguinated, and a tourniquet inflated to 250 mm Hg. The wound was explored under loupe magnification and a 2 by 3 cm pseudoaneurysm was located, emanating from the superficial palmar arch between the common digital arteries to the ring and little fingers (Fig. 24–6A). The mass occupied the entire space between the two arteries and a 1-cm segment of the superficial arch appeared thin-walled and fibrotic at the origin of the pseudoaneurysm (Fig. 24–6B). Proximal and distal control of the vessel was obtained with a vascular loop around the superficial arch at the base of the common digital arteries. Resection of the pseudoaneurysm was done, and then the free ends of the arch were brought together easily (Fig. 24–6C). A primary anastomosis in this position was formed by an intersection with the superficial palmar arch and the third and fourth common digital arteries. If there is concern that the tension produced by such an anastomosis could lead to occlusion, then a timed Allen test should be performed. This test can be performed by closing the cut ends of the superficial palmar arch with microvascular clamps. Vessel loops provided occlusion of the arch on both sides proximal to the common digital arteries. Normal color and turgor was noted with brisk capillary refill in the ring and little fingers within 3 seconds after release of either the ulnar or the radial side of the superficial palmar arch. If the arteriogram shows digital flow and the Allen test has demonstrated sufficient flow at rest, you will not need to perform a vein graft, and the superficial palmar arch can be ligated (Fig. 24–7). A timed Allen test was again performed, with occlusion of the radial and ulnar arteries at the wrist crease. Brisk capillary refill was again noted within 3 seconds after sequential release of the occlusion of the arch.