Total Knee Replacement: Medial Release via Osteotomy
The traditional method of managing severe varus deformity involves extensive stripping of soft tissue from the tibia. Medial ligament release via an osteotomy of the medial epicondyle1 is an alternative method for correcting soft tissue contractures. The flexion contracture that commonly coexists with varus deformity from arthritis, and is secondary to contractures of the posteromedial capsule, is easily and safely corrected with the exposure provided by the osteotomy.
Indications
- Knees with fixed varus deformity, particularly when a flexion contracture of 15 degrees or greater is present. The osteotomy can be used in both primary and revision total knee arthroplasty.
- Ankylosed knees (including conversion of a knee fusion to a total knee arthroplasty)
- Revision arthroplasty that requires an allograft-revision implant composite to reconstruct the distal femur
Contraindications
- Knee instability
- Deficient medial collateral ligament
Physical Examination
- Varus deformity that will not correct with valgus stress
- Flexion contracture that will not correct to less than 15 degrees
Diagnostic Tests
- Preoperative radiographs demonstrating medial tibial plateau bone loss
- Examination under anesthesia to confirm flexion contracture
Special Considerations
The epicondylar osteotomy is similar to a trochanteric slide performed with total hip arthroplasty. The osteotomized bone wafer must include the insertion of the adductor magnus tendon to the adductor tubercle. Continuity is maintained from the adductor tendon through the epicondyle and medial collateral ligaments to the tibia. Stability in extension is maintained by preserving ligamentous integrity to the osteotomized fragment of bone.
Preoperative Planning
None
Special Instruments
- 1 1/4-inch osteotome
- No. 2 (or heavier) Vicryl suture on a TP-1 needle, or
- No. 5 Ethibond suture on a V-40 taper cut needle
Anesthesia
Options are general anesthesia, spinal anesthesia, or epidural anesthesia.
Patient and Equipment Positions
- Supine
- Sandbag or foot rest at the level of the popliteal space
Surgical Procedure
- A standard medial parapatellar, midline, midvastus, or trivector approach may be used.
- The capsule is opened and reflected from the medial tibial flare to the midcoronal line.
- Osteophytes are completely removed from the rim of the medial femoral condyle.
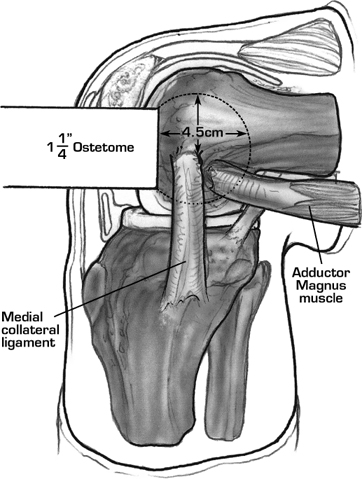
- The knee is positioned at 90-degree flexion. A cautery is used to incise synovium around the margins of the medial femoral condyle and outline the osteotomy site (4 to 5 cm in diameter).
- A 1 1/4-inch osteotome is directed distally to proximally in line with the femur to release a wafer of bone (1 cm thick and 4 to 5 cm in diameter). The osteotome must exit the epicondyle proximal to the adductor tubercle 4 to 5 cm from its entry point. A cortical bridge of bone (1 cm in width) is preserved anteriorly between the anticipated anterior femoral resection and the base of the epicondylar osteotomy for ligament reattachment (Fig. 35–1).
- The osteotomized epicondyle is displaced posterior to the medial femoral condyle, exposing the posteromedial joint capsule.
- The posteromedial joint capsule is released from its attachment to the posterior femur.
- Upon completion of the arthroplasty the knee is repo-sitioned at 90-degree knee flexion.
- The epicondyle is held anteriorly on the medial femoral condyle and Vicryl (No. 2 or heavier) or No. 5 Ethibond sutures are passed in a figure-eight fash ion through the epicondyle and medial femoral condyle. The needle is passed deep under the corti cal bridge to achieve a rigid suture repair. At least two, preferably three, sutures are needed to reattach the osteotomized bone wafer (Fig. 35–2).
- Knee stability is tested prior to wound closure. If the fragment moves with knee flexion, this is noted in the operative record, as is the position of flexion when the movement occurs.
- The osteotomized epicondyle is displaced posterior to the medial femoral condyle, exposing the posteromedial joint capsule.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


