CHAPTER 11 The Patient History and Physical Examination
Cervical, Thoracic, and Lumbar
Differential Diagnosis
The differential diagnosis of spinal pain or related symptoms is enormous when considered in a general sense. Numerous anatomic structures may be associated with pain, multiple local or systemic disease processes can affect the spine, and numerous non–spine-related structures or conditions can result in back or neck pain or mimic syndromes related to spine disorders.1–5 In addition, numerous psychosocial factors can produce ongoing pain and disability. The ability to process all of the available possibilities and to develop a relatively short list of diagnostic options depends heavily on the ability to obtain a thorough history and physical examination. It is helpful to begin with an understanding of structures in the spine that can be associated with pain and their patterns of pain referral.
From an anatomic perspective, a structure must be innervated to cause pain. In the spine, the list of discrete anatomic structures with sensory innervation (i.e., potential pain generators) includes muscles, tendons, ligaments, fascia, anulus of the intervertebral discs, bone, zygapophyseal joints, dura mater, nerve roots and dorsal root ganglia, and vascular elements.1,2 All structures of common embryologic segmental origin tend to refer pain in very similar patterns, and the pattern of pain is determined by the nerve supply to the structure.1 The end result is that there is substantial overlap between the referral patterns for anatomic structures of the same spinal level, such as intervertebral discs and zygapophyseal joints, and dermatomal, myotomal, and sclerotomal referral patterns at many spinal levels (Fig. 11–1). The location of pain or radiating symptoms can often be a useful feature in the identification of an affected spinal level, although the location of pain alone does not indicate which particular anatomic structure is the source of the specific symptom.
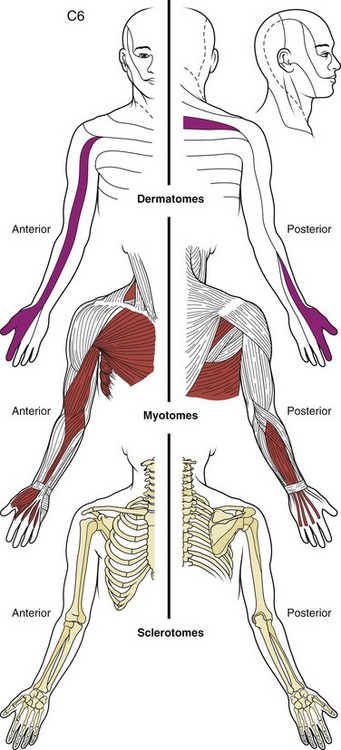
FIGURE 11–1 Drawing of dermatome, myotome, and sclerotome of C6 level showing substantial overlap in distribution.
(From Bland JH: Disorders of the Cervical Spine: Diagnosis and Medical Management, 2nd ed. Philadelphia, WB Saunders, 1994.)
The zygapophyseal joints are one of the best-studied structures in terms of pain referral patterns and relative prevalence in patients with spinal pain. In the cervical spine, the pattern of pain distribution from the stimulation of specific zygapophyseal joints has been described (Fig. 11–2).6 Those results were subsequently validated in a study of patients with cervical complaints based on pain distribution and response to diagnostic blocks.7 Another study using a double-block protocol on patients with persisting symptoms after whiplash injury found that the prevalence of C2-3 zygapophyseal joint pain in patients with headache was 50%; in patients without C2-3 zygapophyseal joint pain, the prevalence of symptoms related to the lower cervical zygapophyseal joints was 49%.8 Although there is far less clinical information on pain associated with thoracic zygapophyseal joints, a similar map of referral patterns has been identified (Fig. 11–3).9
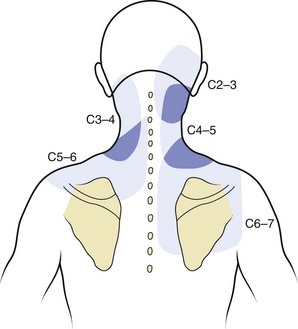
FIGURE 11–2 Map of characteristic areas of pain referred from cervical zygapophyseal joints (C2-3 to C6-7).
(From Dwyer A, Aprill C, Bogduk N: Cervical zygapophyseal joint pain patterns I: A study in normal volunteers. Spine 15:453-457, 1990.)
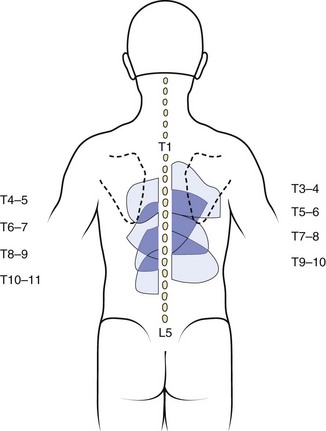
FIGURE 11–3 Map of characteristic areas of pain referred from thoracic zygapophyseal joints (T3-4 to T10-11).
(From Dreyfuss P, Tibiletti C, Dreyer S: Thoracic zygapophyseal joint pain patterns: A study in normal volunteers. Spine 19:807-811, 1994.)
In the lumbar spine, there has also been a great deal of attention directed to the zygapophyseal joints as potential sources of pain, although the relative frequency with which they seem to be primary pain generators is less than for cervical zygapophyseal joints causing pain in patients with chronic whiplash. A more recent study noted a 15% overall prevalence of zygapophyseal pain in a group of 176 patients with chronic low back pain using a diagnostic double-block protocol.10 Although pain associated with lumbar zygapophyseal joints is generally described as occurring with lumbar extension and rotation, the authors of that study did not find any consistent clinical features that were associated with the presence of a positive diagnostic response to injections.10 Stimulation of lumbar zygapophyseal joints can result in either local axial or, far less frequently, radiating pain, and pain referral patterns have been documented.11
Multiple authors have addressed the distribution of pain associated with intervertebral discs. Cloward12 first described cervical discography and noted that pain that seemed to be emanating from irritation of the anulus resulted in radiating pain into the thoracic or scapular regions in distinct patterns (Fig. 11–4). Similar findings were more recently described by others.13 As mentioned previously, pain referral patterns are similar to patterns noted for cervical zygapophyseal joints, with the level of spine pathology, rather than the actual structure involved, affecting the pain referral pattern.
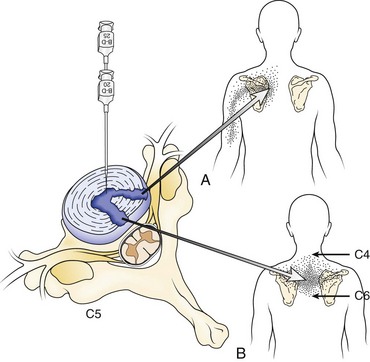
FIGURE 11–4 A and B, Pain referral pattern from posterolateral (A) and central (B) discs.
(From Cloward RB: Cervical discography: A contribution to the etiology and mechanism of neck, shoulder and arm pain. Ann Surg 150:1052-1064, 1959.)
Other pain referral patterns that should be recognized by all physicians treating patients with spine disorders include patterns related to neurologic injury. These patterns are discussed further later in the section on the neurologic examination, but identifying the dermatomal pattern of pain is central to the assessment of individuals with potential nerve root pathology (Fig. 11–5). Nerve root symptoms include paresthesias, burning, hyperalgesia, aching, analgesia, or pain. The ability to identify a dermatomal pattern to the symptoms can help localize the area of spine involvement.
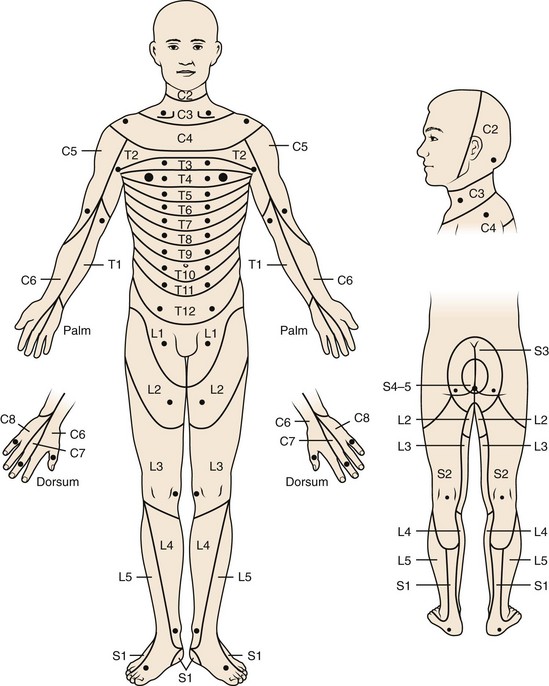
FIGURE 11–5 Dermatomal distribution and key sensory points.
(From American Spinal Injury Association: International Standards for Neurological Classification of Spinal Cord Injury [reprint]. Chicago, American Spinal Injury Association, 2008.)
The clinical utility of pain provocation is uncertain because there are inherent problems with this approach owing to the complex nature of pain perception.1,14–18 The identification of a “pain generator” in individuals with chronic spinal pain can be difficult. In contrast to cutaneous sensation, nociceptive signals from deep somatic structures such as joint capsules, fascia, and periosteum are carried by relatively few primary afferent fibers, resulting in only vague localization of pain.16 Additionally, there is the issue of convergence, in which a single dorsal horn cell may receive synaptic input from afferent fibers that innervate many structures and can result in multiple structures producing similar patterns of pain perception. This convergence makes it extremely difficult to validate a single entity as “the cause” of an individual’s pain because the stimulation of any one of numerous structures may result in identical perceptions of pain.16 These issues become even more complex when additional potential neurologic and psychological changes that can occur with chronic pain are involved.
Biomedical Factors and the Medical History
“Red Flags”—What Not to Miss
It is essential to identify all conditions that pose a substantial, imminent risk for further harm to the patient. Many authors have identified specific “red flags” in the history of patients with low back complaints that indicate the presence of such a condition; these include infection, tumor, fracture, cauda equina injury, and progressive neurologic injury such as motor loss or myelopathy (Table 11–1).19–22 “Red flags” for the possibility of cancer include age older than 50 years, previous cancer history, unexplained weight loss, pain not relieved by bed rest, duration of pain for more than 1 month, and failure of conservative therapy after 1 month.22 The combined sensitivity of age older than 50 years, history of cancer, unexplained weight loss, and failure of conservative therapy is nearly 100%.22 A history of smoking also increases a patient’s risk for cancer.21 Although similar data are unavailable for cervical and thoracic pain, the same factors seem relevant.
TABLE 11–1 “Red Flags”: Emergent or Urgent Medical Conditions That Need to Be Identified Promptly in All Patients Presenting with Possible Issues Related to the Spine
| Symptom or Finding | Possible Significance |
|---|---|
| History of cancer | Cancer |
| Unexplained weight loss | |
| Age >50 yr | |
| Failure to respond to >1 mo of conservative care | |
| Duration of pain >1 mo | |
| No pain relief with bed rest | |
| Night pain | |
| History of smoking | |
| Known osteopenia or osteoporosis | Fracture |
| History of corticosteroid use | |
| Age >50 yr | |
| DISH or ankylosing spondylitis | |
| Trauma (major in younger individual, minor in older individual) | |
| Fever | Infection |
| Illicit use of intravenous or percutaneously injected drugs | |
| Recent or known infection | |
| Immunosuppressive illness | |
| Use of immunosuppressive medications | |
| Tuberculosis exposure | |
| Progressive weakness in limbs | Cauda equina or spinal cord injury |
| Progressive balance deficit or loss of coordination | |
| Bowel or bladder dysfunction or urinary retention | |
| Sexual dysfunction | |
| Numbness or paresthesias in perineum or saddle anesthesia | |
| Significant weakness of major muscle group or progressive motor loss in limb | Severe or progressive radiculopathy |
DISH, diffuse idiopathic skeletal hyperostosis.
Spine infections, including discitis, osteomyelitis, and epidural abscess, are usually blood-borne from other regions.22 Important risk factors for infection include the use of illicit intravenous drugs, active or recent infection elsewhere (e.g., urinary tract, pulmonary, skin, dental), and immunosuppression (owing to either medications or illness affecting the immune system).19,22 Additional risk factors for infection include diabetes and history of tuberculosis or exposure to a region endemic for tuberculosis.
The risk of fracture is elevated in patients older than 50 years, particularly patients older than 70 years.22 Patients with a history of corticosteroid use or known osteopenia or osteoporosis are also at increased risk for fracture. A history of fracture in a younger individual after major trauma, in an older individual after minor trauma, or in anyone with the potential for reduced bone density should also be considered a risk factor. Trauma and fracture risk are discussed further elsewhere in this book.
Significant neurologic injuries include cauda equina syndrome, progressive radiculopathy, or myelopathy. Cauda equina syndrome should be considered in a patient with saddle anesthesia; bowel, bladder, or sexual dysfunction; or significant lower extremity pain and weakness, particularly if bilateral.19,22 Progressive neurologic loss from nerve root compression is an indication for urgent surgical intervention and needs to be identified promptly. Myelopathy can present in various ways, including hand paresthesias or decreased fine motor control; lower extremity weakness or gait instability; sensory alterations in the trunk or extremities; or changes in bowel, bladder, or sexual function.23
Axial Versus Radicular Pain
The distinction between axial and radicular pain is fundamental in assessing a patient with a potentially neurogenic problem. Axial pain in the cervical, thoracic, or lumbar region suggests a different etiology, evaluation, diagnosis, and potentially treatment than radicular pain. For all levels of the spine, pathology involving the musculotendinous and ligamentous structures, zygapophyseal joints, vertebrae, and anulus of the intervertebral discs tends to cause axial pain. Other structures in the cervical and thoracic regions that can result in axial pain include soft tissue structures in the neck; vascular structures (e.g., aorta or carotid arteries); portions of the brachial plexus such as the long thoracic or suprascapular nerves; the proximal portion of ribs; costovertebral or costotransverse articulations; various structures within the shoulder; and various visceral structures, including the pancreas, gallbladder, lung and pleura, and stomach or duodenum (Fig. 11–6).
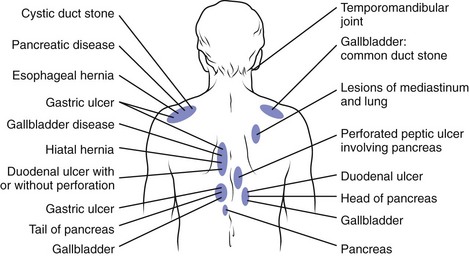
FIGURE 11–6 Posterior referral sites from distant visceral or somatic structures.
(From Nakano KK: Neck pain. In Kelley WN, Harris ED Jr, Ruddy S, et al [eds]: Textbook of Rheumatology, 4th ed. Philadelphia, WB Saunders, 1993.)
For the lumbar spine, the hip and pelvic structures must be considered as potential sources of low back, buttocks, or posterolateral hip pain. Particular sources of low back or buttock pain related to the bony pelvis include the sacroiliac joints, the sacrum (e.g., stress fractures), the ilia, and the hip joints. Other structures and processes that can result in low back pain include the kidneys and ureters; the pancreas; gastric ulcers; vascular abnormalities (e.g., aortic aneurysm); and retroperitoneal processes such as hematoma, endometriosis, or lymphadenopathy associated with malignancy.24
As with upper extremity pain, lower extremity radicular pain often has different etiologies and generally implies involvement of the lumbosacral nerve roots, the conus medullaris, or the spine. The lumbar zygapophyseal joints and the sacroiliac joints also may occasionally be associated with radicular leg pain.11,25 Distal lower extremity symptoms also may arise from intra-articular hip pathology; greater trochanteric bursitis; vascular pathology (e.g., vascular claudication); peripheral nerve injuries; compartment syndrome; local musculotendinous, ligamentous, or bony structures; and pelvic causes such as endometriosis.
Patient Demographics
Growth and development have a profound impact on the development and approach to various processes, such as spondylolisthesis, scoliosis, and Scheuermann kyphosis. In contrast to the adult spine, the developing bony spine is relatively more prone to injury than some soft tissue structures. In a study by Micheli and Wood,26 47% of adolescents presenting to a pediatric sports medicine clinic were diagnosed with spondylolysis and only 11% had disc abnormalities compared with 48% of adults presenting to a low back pain clinic who were thought to have disc pathology. Generally, symptomatic isthmic spondylolysis is almost entirely seen in older children, adolescents, or young adults, although the rate of pars defects identified in the general population does not change substantially between the ages of 20 and 80.27,28 Although 50% or more of children may be affected by low back pain by age 15,29,30 significant spinal pain in children is uncommon and should raise concern for the presence of serious medical pathology.31,32 Infection, neoplasm, rheumatologic conditions such as ankylosing spondylitis and juvenile rheumatoid arthritis, and other nonspine sources of pain may be more common in children and adolescents than in adults.31,32
In adults, the frequency of certain spine conditions varies by age group. Disc herniations are most frequent during the 4th and 5th decades, although they can affect individuals in their 50s and 60s or children and young adults.33 Degenerative spinal stenosis and degenerative spondylolisthesis tend to present later in life. As mentioned previously, some medical conditions, including ankylosing spondylitis, spondylitis associated with inflammatory bowel disease, and tumors such as osteoid osteoma and osteoblastoma, tend to manifest in younger adults (20s and 30s). Other conditions, such as osteoporosis, polymyalgia rheumatica, metastatic cancer, or multiple myeloma, tend to occur in older adults (40s and 50s or older) (Fig. 11–7).3,34
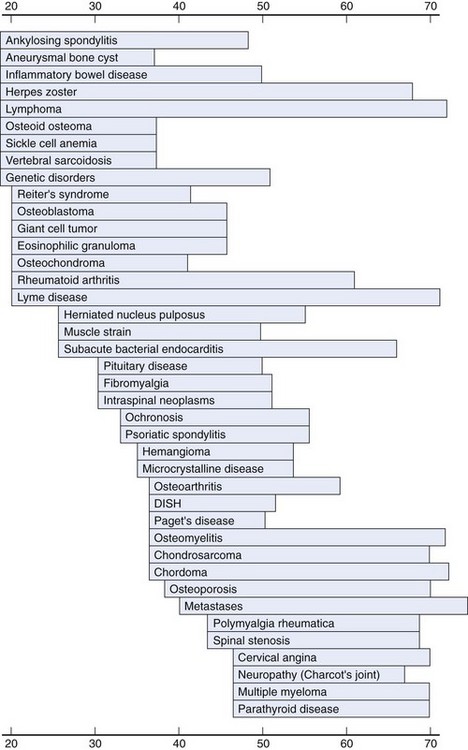
FIGURE 11–7 Age at peak incidence of neck pain associated with various disorders.
(From Borenstein DG, Wiesel SW, Boden SD: Neck Pain: Medical Diagnosis and Comprehensive Management. Philadelphia, WB Saunders, 1996.)
Gender is a factor in many spine pathologies. Osteoporosis is more common in women than in men, and osteoporotic fractures are more common in women. Neck pain also has been noted to be more prevalent in women than in men.35,36 Rheumatoid arthritis, polymyalgia rheumatica, and endocrine disorders also tend to occur more frequently in women.34 Spondyloarthropathies; infections; and various spine tumors, such as multiple myeloma, lymphoma, osteoblastoma, and eosinophilic granuloma, occur more frequently in men.
Demographic factors such as race, ethnicity, and cultural milieu may also play a role in the prevalence of some spine disorders but are less well studied. Whites tend to have higher rates of osteoporosis than some other races, and metabolic conditions such as Gaucher disease can be associated with certain ethnic groups.3 Whites have a higher rate of spondylolysis than African Americans.27 The prevalence of low back pain also varies in different parts of the world, with industrialized regions reporting a higher prevalence of low back complaints than rural, low-income areas.37 Pain perception, disability, and other effects of pain on individuals vary widely and depend on many cultural and social factors.
Past Medical History
In addition to identifying prior surgical procedures, it is important to identify all past and current medical conditions because many medical problems can be associated with spine issues and can affect care of a patient with a spine disorder. As noted previously, a history of cancer, recent infection, or disease processes that affect the immune system or may require immunosuppressive medications can be associated with significant spine problems. Other medical conditions, such as osteoporosis, ankylosing spondylitis, and diffuse idiopathic skeletal hyperostosis, may place patients at increased risk for spine fracture.38 Some congenital or genetic syndromes, such as Marfan syndrome and Down syndrome, can be associated with spine anomalies that must be identified. Vascular disease, such as vascular claudication or aortic aneurysm, can produce symptoms that mimic spine pathology. Other disorders, including cardiac or pulmonary disease, renal disorders, skin conditions, gastric ulcers, diabetes, and hepatic disorders, may have an impact on potential treatment options and may preclude certain therapies. Clinicians need to be aware of all facets of a patient’s medical history and the potential influence that medical issues may have on the care of the patient.
Family History
The family history is a necessary component of a complete medical history. Although back pain and many other spinal conditions are common in the general population, data suggest possible genetic risk factors for lumbar degenerative disc disease.39 A family history of rheumatologic diseases, particularly conditions associated with HLA B-27 such as ankylosing spondylitis, Reiter syndrome, and inflammatory bowel disease, can suggest a tendency for, or risk of, developing a similar process.3,40 Other inheritable diseases, including certain neuromuscular diseases, may be associated with progressive spinal deformity, and patients with a genetic predisposition for certain medical conditions (e.g., vascular disease, specific cancers) may also present additional diagnostic considerations.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


