Chapter 8 The needle contact test
INTRODUCTION
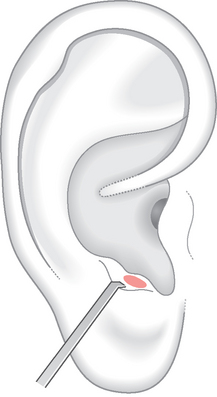
In 1995 the physician Stefano Marcelli proposed the ‘active point test’ (‘Il test dei punti attivi’).1 His intention was to introduce a diagnostic method which could quickly and accurately identify the most effective points for therapy. The test was used by Marcelli in the case of painful syndromes and required the collaboration of the patient, who was asked to keep his attention fully focused on his perception of pain throughout the test. Among the meridian acupuncture points suitable in the treatment of a given painful condition Marcelli was able, through his test, to identify the point/s which succeeded in reducing the intensity of symptoms. The test was proposed to doctors and physiotherapists and the author recommended several kinds of stimulation, among them acupressure. A needle was to be applied to the acupuncture point for a few seconds, touching the skin without penetration. The sensation that should be felt by the patient was that of a superficial puncture of such light intensity that it should not cause any bother at all. The best diameter for the testing needle was between 0.25 and 0.35 mm. Especially in the case of more widespread pain syndromes, different points were tested following the concepts of harmonization and redistribution of energy in the meridians which typify traditional Chinese medicine (TCM). Once the meridian point effective in reducing pain was identified, the same needle was inserted into the skin for starting treatment. According to Marcelli, the result of the test could be rated as indifferent, negative, moderately and strongly positive. An indifferent answer corresponded to no variations, negative to a worsening of pain and positive to more or less rapid and widespread reduction of pain.
APPLICATIONS OF THE NEEDLE CONTACT TEST
The different applications examined to date are:
FOR CURRENT PAIN
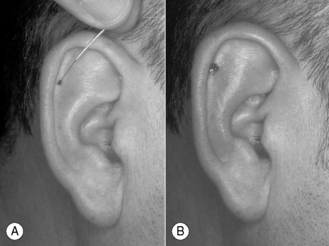
The best results of NCT are in acute pain due to trauma (for example bruising, sprains, fractures, etc., visceral disorders or postoperative pain). After the needle has been applied for 5–10 seconds one must wait for the effect, which usually manifests in the following minute. If the reduction of pain is rated by the patient to be at least 25–30%, one can wait for a further 2–3 minutes to verify if the effect is going to pass rapidly or remain stable in time. There is of course great anticipation on the part of the patient and this initial variation of pain can be considered a placebo effect. Other neighboring points can therefore be tested, with the aim of obtaining an analgesic effect beyond the threshold of the placebo effect (commonly rated as being about 35–40% of the total). For example, the lady in Figure 8.1 suffered with acute pain of her sixth upper right tooth which was rated about 7 on a verbal numeric scale (VNS). She had undergone devitalization of the tooth the day before and at the time of auricular diagnosis had not taken any painkillers. Two different points were located with PPT on the central area of the lobe, which does not correspond either to the French or to the Chinese representation of the jaw (LO3 He) (see the representation of the teeth described in Ch. 5). The points were very close to each other, the distance between them no greater than 1 mm (Fig. 8.1). They were consecutively tested; the pain was rated as 5 in severity 1 minute after needle contact of the lower point, but 3 minutes later had again reached 6–7; however, NCT on the upper point lowered the pain steadily to 3 and this level remained stable for the next 5 minutes. A temporary sterile disposable steel implant was placed in this point and the patient had no relapse of pain.

FOR MIGRAINE
My reasons for distinguishing this pain from musculoskeletal pain is that migraine is a neurovascular pain which manifests itself on the trigeminal territory and tends to relapse over time. Migraine is a disabling disorder with a high social and economical impact which requires a careful strategy of prophylaxis for reducing the number of attacks and preventing the chronic abuse of painkillers. Here acupuncture can gain ground with honor as an alternative treatment or for use in combination with pharmacological therapy.2–8
In 15 patients with migraine attacks (13 female, 2 male) pain scoring with a VNS was repeated 1, 5, 15 and 30 minutes after NCT. Pain decreased about 26.4% after 1 minute and 47.4% after 5 minutes; in the succeeding time intervals the pain level remained unchanged (Fig. 8.2). The points identified with NCT were mainly distributed in the area of the forehead (AT1 e) and the temple (AT2 nie) on the Chinese map and frequently also on the supero-internal surface of the antitragus overlapping partially with the Chinese subcortex area (AT4 pizhixia) (Fig. 8.3).
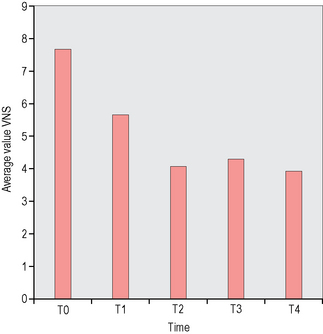
It has to be stressed that AT4 extends itself to the bottom of the medial wall of the antitragus and carries the generic indication ‘painful symptoms’. The first documented application of NCT in a case of migraine attack was performed on one of these patients and a steady level of analgesia was maintained up to the 60th minute.9
FOR PAIN PROVOKED BY PALPATION
Any part of the body, if painful at palpation, can be challenged with NCT.
The locomotor apparatus is the favorite for this kind of test, and inflammation of the joints, bursitis and tenosynovitis are often successfully treated. For example, in Figure 8.4 the 45-year-old male patient had been suffering with tennis elbow for 3 months. In the previous 2 weeks the pain had increased and he was limited in his daily activities. He felt acute pain on palpation and pressure on his right lateral epicondyle. Also movements of pronation of the arm and dorsiflexion of the wrist were very painful.
The patient asked for treatment with steroids but I convinced him to try ear acupuncture first. Performing PPT, I found a sensitive point on the scapha corresponding to the representation of the elbow. NCT on this point lowered pain at palpation of the lateral epicondyle (Fig. 8.4A) and a temporary sterile single-use steel implant (ASP) was placed there. Two more ASPs immediately beneath improved pain at pronation of the arm and dorsiflexion of the wrist (Fig. 8.4B). This treatment with three grouped implants in all was efficacious enough to make steroid treatment unnecessary. The patient received similar therapy 15 days later with lasting results.
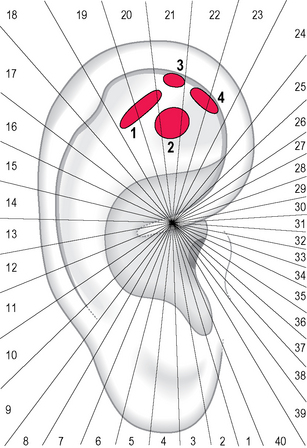
As regards the issue of the different representation of the lower limb in the French and Chinese maps, see the section on the musculoskeletal system in Chapter 5 (p. 115). The hypothesis that different parts of the knee and the ankle may have a different representation on the ear was forwarded by Dr Caterina Fresi. She examined 34 patients with knee pain caused by current injury of the lateral capsule–ligament complex (14 patients) or of the medial complex (20 patients). In the first group the pain syndrome evoked a sensitization of an extended oval area covering the Chinese hip and knee area (area 1 in Fig. 8.5), whereas in the second group the sensitized area was rather rounded and corresponded to the French thigh and knee area (area 2 in Fig. 8.5). Dr Fresi also examined 15 patients with ankle pain caused by current injury of the capsule–ligament complex of the malleolus lateralis (8 patients) or of the complex of the malleolus medialis (7 patients). In the first group the sensitized area corresponded to the Chinese ankle and toe/heel area (area 3 in Fig. 8.5) whereas in the second group the sensitized area corresponded to the French foot area (area 4 in Fig. 8.5).
< div class='tao-gold-member'>

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


