66
Tears of the Triangular Fibrocartilage Complex
Philip E. Blazar and Scott D. Mair
History and Clinical Presentation
A 19-year-old right hand dominant college student presented for evaluation of left wrist pain 5 months after closed treatment for a distal radius fracture. The pain was ulnar sided and associated with activities, particularly those involving maximal extension or pronation/supination against resistance (e.g., turning a doorknob on a heavy door). There was no clicking. The patient’s injury had been treated in a long-arm cast for 8 weeks. Office notes from the referring physician document a diagnosis of distal radius fracture and distal radioulnar joint (DRUJ) dislocation reduced and treated in a closed manner. The patient was referred for persistent ulnar sided wrist pain.
PEARLS
- Patients with injuries to the wrist, particularly displaced distal radius fractures, should be examined after reduction for instability of the DRUJ.
- The majority of patients presenting with ulnar-sided wrist pain can be managed non-operatively and returned to normal activities.
- The central component of the TPCC can be excised to a stable rim without compromising its biomechanical function.
PITFALLS
- The differential diagnosis of ulnar-sided wrist pain is lengthy. A careful examination of the ulnar side of the wrist will frequently rule in other causes of patient’s symptoms.
- The dorsal branch of the ulnar nerve crosses from volar to dorsal in the region of ulnar (6U) wrist arthroscopy portals. Careful dissection and protection of this nerve is mandatory to prevent complications.
Physical Examination
The hand, wrist, elbow, and shoulder were normal to inspection. There was minimal atrophy of the forearm musculature. Active range of motion of all joints was symmetric bilaterally. There was tenderness to palpation radial to the ulnar styloid with the arm in neutral rotation and mild discomfort, but no increased translation with stressing the DRUJ. TFCC grind maneuver produced no pain or clicking. The extensor carpi ulnaris (ECU) tendon did not subluxate out of its groove, and wrist instability maneuvers caused minimal discomfort and no clunking. Neurologic and vascular examinations were normal.
Diagnostic Studies
Anteroposterior, lateral, and oblique radiographs of the wrist were obtained (Fig. 66-1).
Differential Diagnosis
Ulnar styloid nonunion
TFCC tear
Ulnocarpal abutment
DRUJ incongruity
Distal radius malunion
ECU tendinitis
Diagnosis
Triangular Fibrocartilage Complex (TFCC) Tear
Ulnar-sided wrist pain is a common complaint. The patient’s age, hand dominance, avocations, and occupation are important historical factors, and the nature and date of injury should be sought. Patterns of injury have been associated with particular recreational activities (e.g., hook of the hamate fractures with sports involving a bat or club). Neurologic complaints are common and should be sought. The differential diagnosis above is limited to the diagnoses likely after a distal radius fracture.
Examination of the TFCC is performed in conjunction with a thorough exam of the wrist, elbow, and hand, including neurovascular structures. Direct palpation of the bony and soft tissue structures of the ulnar side to localize point tenderness is the most helpful examination maneuver. Tenderness radial or ulnar to the ECU tendon with the wrist in neutral rotation may be consistent with a TFCC lesion. The DRUJ is examined with the patient’s elbow on a table in front of the examiner. The DRUJ is stressed with one of the examiner’s hands grasping the distal ulna and the other grasping the radius. Volar and dorsal translation is assessed in neutral, pronation, and supination. A TFCC grind test is performed with the wrist in ulnar deviation and dorsiflexion with an axial load applied to the hand by the examiner as the carpus is rotated on the fixed forearm. Radiographs aid in establishing the diagnosis of a malunion of the distal radius or a nonunion of the ulnar styloid. Fractures at the base of the ulnar styloid are more likely to be associated with a TFCC injury that will produce persistent symptoms if untreated. Ulnocarpal abutment is more likely in patients with ulnar positive or ulnar neutral variance.
The term triangular fibrocartilage complex was originally used by Palmer and Werner for the group of structures that stabilize the carpus and distal radius to the fixed distal ulna. This complex includes the volar and dorsal radioulnar ligaments, the ulnar collateral and ulnocarpal ligaments, and the articular disk. The articular disk separates the carpal bones from the distal radioulnar articulation. The complex is central to three biomechanical functions of the wrist: (1) stability of the DRUJ, (2) axial load transmission from the carpus to the ulna, and (3) ulnar-sided carpal stability.
| Main Category | Subcategories |
| Type 1: Traumatic | A: Horizontal tear adjacent to the radius B: Peripheral detachment from the ulna C: Tear of the ulnocarpal ligaments D: Avulsion from sigmoid notch |
| Type 2: Degenerative | A: Partial-thickness thinning of the articular disk B: A + chondromalacia of lunate and/or ulnar head C: B + full-thickness tear of the articular disk D: C + partial tear of the lunotriquetral ligament E: D + pull tear of the lunotriquetral ligament and arthrosis |
TFCC lesions were classified by Palmer in the Journal of Hand Surgery in 1989. There are two main categories: traumatic and degenerative (Table 66–1).
Nonsurgical Management
Recommended initial management of traumatic TFCC injuries based on history and physical examination is 4 weeks of immobilization. The intimate relationship of the articular disk and the DRUJ typically requires the use of an above-elbow cast. At 4 weeks, patients are begun on range-of-motion and strengthening exercises and progress as tolerated. Surgical management is indicated for failure of conservative treatment.
Degenerative lesions are more common in patients with ulnar positive variance. Recommended initial treatment includes activity modification, splinting, and nonsteroidal medications. The author’s experience has been that patients with negative or neutral ulnar variance are more likely to respond to conservative treatment. Surgical intervention is indicated for failure of conservative treatment.
Surgical Management
Surgical treatment of lesions of the TFCC continues to evolve. Traumatic lesions are typically classified at the time of diagnostic arthroscopy. Wrist arthroscopy is performed with the wrist in 10 pounds of traction to facilitate visualization of the TFCC. The portals for visualization and manipulation of the TFCC include 3–4, 4–5, and 6R. Type 1A or central lesions are the most common traumatic injury seen. Arthroscopic debridement of the unstable edges of the tear is typically recommended. Cadaveric studies have demonstrated that excising the central two thirds of the articular disk does not alter the biomechanical functions of the TFCC. Post-operatively, patients are encouraged in immediate mobilization. Return to work or athletics usually is within 6 to 12 weeks. Diagnostic arthroscopy of this case demonstrated a type 1B lesion.
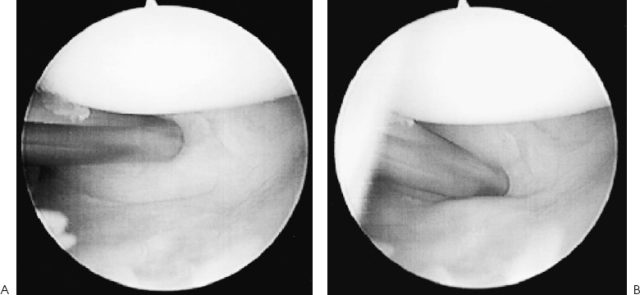
The finding of a peripheral detachment of the TFCC is not always as obvious at arthroscopy as one might anticipate. A helpful diagnostic maneuver is the trampoline sign that is elicited with a probe in the 4–5 portal and the arthroscope in the 3–4 portal. The elasticity of the articular disk is tested with the probe, and a positive test is loss of the normal tissue tautness (Fig. 66-1).
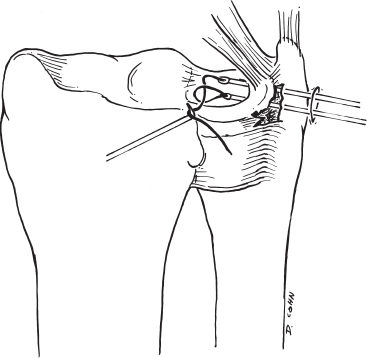
Two or three sutures are placed and tied over the capsule (Fig. 66-2). Postoperatively the patient is immobilized for 4 to 6 weeks in a Munster cast to eliminate rotation of the forearm, and an additional 2 to 4 weeks in a wrist splint. Return to full activity is allowed at 3 months.
Controversial point: Treatment of type 1C and 1D TFCC injuries has not received as much attention as the more common injury patterns. Classically it was believed that radial detachments would not heal and were debrided to stable edges, if there was not a bony fragment attached to the articular disk. Recently, open and arthroscopically assisted repair of avulsion of the TFCC from the sigmoid notch (1D lesions) has been described but outcome data are limited. Distal avulsions (1C) are the least common injury pattern described in most series. Whether debridement or repair of 1C or 1D lesions is superior is unclear at present.
Treatment of degenerative lesions of the TFCC depends on the Palmer classification stage. Lesions classified as 2A or 2B are typically treated nonoperatively with antiinflammatories, splinting, and activity modification. An extraarticular ulnar shortening or an intraarticular “wafer” procedure (with removal of 2 to 4 mm of distal ulna) can be considered in the unusual case of symptoms refractory to these measures. If the lesion has progressed to stage 2C, a TFCC debridement is performed. If the patient is ulnar positive, this may be combined with a “wafer” procedure. Treatment of stage 2D lesions includes an ulnar shortening and treatment of the wrist instability if it is substantial. Stage 2E lesions may present with substantial degeneration of the ulnar carpus and typically require a salvage procedure.