Fig 1
A 36-year-old female presented with a traumatic right hip fracture-dislocation, with a large, displaced intra-articular femoral head fracture (a). CT scan demonstrated the complex fracture pattern (b). Using a digastric trochanteric flip osteotomy, the articular surface was visualized and the large fragment anatomically repaired using countersunk 2.4 mm cortex screws (c). Postoperative radiographs at 6 months reveal an anatomic fracture reduction with minimal heterotopic ossification and no evidence of radiographic posttraumatic arthritis or avascular necrosis (d)
The medial femoral circumflex artery (MFCA) is the primary blood supply to the femoral head. There are five described branches of the MFCA, including the acetabular branch, which yields the medial epiphyseal and inferior retinacular vessels, and the deep branch of the MFCA, which yields the superior retinacular and lateral epiphyseal vessels (Table 1). All together, the deep branch of the MFCA and its branches have been shown to be the predominant vascular supply to the femoral head. Gautier et al. defined the anatomy of the deep branch of the MFCA [5], and Ganz later described the digastric trochanteric osteotomy highlighted below as a safe way to approach the entirety of the hip joint, without injuring this artery and without increasing the risk of AVN [6]. It is important to recognize that several studies have shown the importance of an anastomosis with the between the inferior gluteal artery and the MFCA, at the level of the piriformis [5, 7, 8]. This anastomosis may be capable of compensating after an injury to the deep MFCA and needs to be preserved during surgical approach.
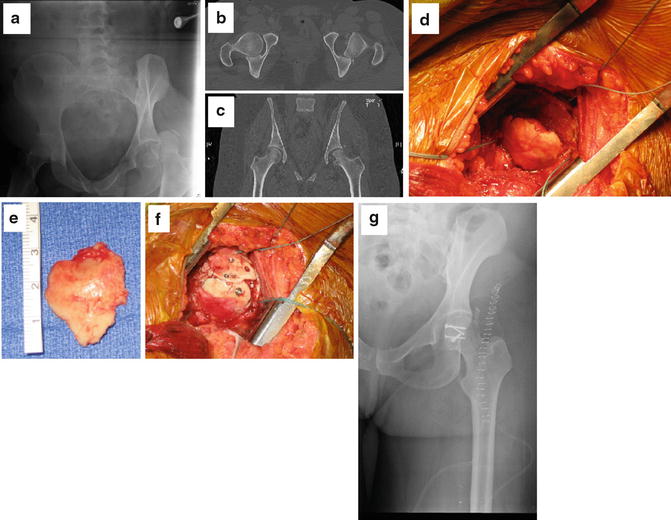
Fig 2
A 45-year-old female presented to the trauma bay with a traumatic left hip fracture-dislocation with a large, displaced femoral head fracture (a). CT scan demonstrated the complex fracture pattern (b, c). Using a Smith-Petersen dislocation approach, the articular surface was visualized and the large fragment anatomically repaired using countersunk flat-headed 2.0 mm and 2.7 mm cortical screws (d–f). Postoperative radiographs reveal an anatomic fracture reduction (g)
Table 1
The five branches of the medial circumflex femoral artery
Branch | Path |
|---|---|
Superficial | Courses between pectineus and adductor longus |
Ascending | To adductor brevis, adductor magnus, and obturator externus |
Acetabular | Gives off foveolar artery (medial epiphyseal artery) |
Descending | Courses between quadratus femoris and adductor magnus |
Deep | To the head of the femur |
Surgical Technique: Digastric (Trochanteric Flip) Osteotomy
The patient is positioned in the lateral decubitus position using a radiolucent beanbag or hip positioners on a standard flat-top radiolucent table [6, 9]. A Kocher-Langenbeck (gluteus maximus split) or modified Gibson exposure (anterior to gluteus maximus) can be utilized to expose and access the proximal femur and femoroacetabular joint. The hip is then internally rotated, and electrocautery is used to identify the posterior margin of the gluteus medius and vastus lateralis insertions on the proximal femur. The planned osteotomy is pre-drilled to accept at least three 3.5 mm screws in an effort to minimize difficulty with reduction and fixation of the osteotomy at the completion of the case. A trochanteric osteotomy is performed using an oscillating saw and broad osteotome, creating a wafer of bone approximately 1.5 cm in thickness. At its proximal limit, the osteotomy should exit just anterior to the most posterior fibers of the gluteus medius; this preserves and protects the deep branch of the MFCA, which becomes intracapsular at the level of the superior gemellus. The remaining gluteus medius fibers are then released, as are the posterior fibers of the vastus lateralis, to the level of the gluteus maximus insertion on the femur. By performing these releases, the trochanteric wafer is then mobilized anteriorly via the interval between the piriformis and the gluteus medius, exposing the anterior capsule. The capsule is then incised in a z-shaped fashion along the anterolateral femoral neck, with the medial limb directed posteriorly, parallel to, and just lateral to the labrum. The lateral limb must remain anterior to the lesser trochanter in order to protect the MFCA, which lies just superior and posterior to it. The hip is then dislocated anteriorly with gentle flexion and external rotation. The ligamentum teres may need to be incised, allowing the femoral head to dislocate, offering a complete view of the femoral head and acetabular socket. Once exposed, any damage to the labrum or acetabulum can be visualized and treated and loose intra-articular bodies may be removed.
Small comminuted fragments of the femoral head may then be excised, particularly fracture s that are caudal to the fovea. Care should be taken excising fragments in patients with ipsilateral posterior wall fractures. For fragments large enough to fix, it is the authors’ opinion and practice to anatomically fix them. Temporary fixation may be obtained with Kirschner wires. Definitive fixation is then performed with interfragmentary positional or lag screws. Numerous implants have been successfully used, including countersunk 2.7 mm or 2.4 mm screws (flat-headed screws), headless compression screws, and bioabsorbable pins [10]. Regardless of device selected, it is paramount to recess the implant to allow a smooth articulation following fixation. Once the fracture is stabilized, the hip is reduced with traction, extension, and internal rotation. The hip is cycled through a full physiologic range of motion to ensure a concentric reduction and smooth articulation. The capsule may be repaired, but not tightened, since this may create tension on the retinacular vessels and a decreased femoral head perfusion [11]. The trochanter is then reattached using three 3.5 mm cortical screws, pre-drilled previously, directed towards the lesser trochanter.
Related posts:
 Neuromuscular Hip Disorders: Focus on Cerebral Palsy
Neuromuscular Hip Disorders: Focus on Cerebral Palsy
 Surgical Technique: Bone Graft for Avascular Necrosis of the Hip
Surgical Technique: Bone Graft for Avascular Necrosis of the Hip
 Rehabilitation of Non-Operative Hip Conditions
Rehabilitation of Non-Operative Hip Conditions
 Surgical Technique: Open Proximal Hamstring Repair
Surgical Technique: Open Proximal Hamstring Repair
 Subspine Impingement and Surgical Technique
Subspine Impingement and Surgical Technique
 Atraumatic Instability and Surgical Technique
Atraumatic Instability and Surgical Technique
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


