CHAPTER 39 Surgical Management of Axial Pain
Epidemiology and Natural History
Having an appreciation of the factors that affect the health of the population is important in understanding the individual who seeks treatment. A study of adolescents concerning the prevalence of musculoskeletal pain in Finland revealed only approximately 25% of 18-year-old girls and about 50% of boys with no report of neck or arm pain in the last 6 months.1 Of these self-reports to questions about musculoskeletal pain, only a small single-digit percentage sought medical consultation. The author’s of the Finnish study note that this prevalence is high, but that the relevance of such reported pain is questionable without knowing the magnitude of the pain-related disability.
It is known from population-based sectional survey studies that numerous individuals complain of acute or chronic neck pain.2–4 The overall prevalence of “troubles or neck pain” was 34.4% in a Norwegian registry, with 13.8% of that group reporting chronic neck pain of greater than 6 months’ duration.2 Similar numbers were reported by Makela and colleagues4 in a study of chronic neck pain in Finland. In an article on the Saskatchewan population published in 2000, Cotes and colleagues3 found that 54% of 1131 respondents had experienced neck pain in the previous 6 months. Of that group, 5% reported that they were “highly disabled” because of neck pain. A comprehensive review by Manchikanti and colleagues5 suggested that the prevalence of people with high pain intensity with disability owing to neck pain is 15%, with 25% to 60% having chronic symptoms 1 year or longer after the initial episode. Complaints of neck pain in the population are common, if the question is asked, but only a small percentage are plagued enough to seek care; if they do seek care, a fair number of people have persistent pain that may lead to surgical consultation.
Why Understanding the Natural History of a Condition Is Crucial
In patients with apparent mechanical axial pain resulting from a degenerative condition, observation with nonoperative recommendations would be appropriate for most patients. When reviewing natural history studies, there is the inherent selection bias of individuals who sought care because of the severity of their symptoms. Many individuals who report pain on population surveys of prevalence of symptoms would not seek out care. In a population questionnaire study, Badcock and colleagues6 found that 11.7% of questionnaire responders had neck pain and that 21% sought general practice consultation; 77% of responders seeking consultation had persistent symptoms, which was a greater percentage of persistent disability than among responders who did not seek out consultation.
Gore and colleagues7 published a classic series on the long-term follow-up of patients who present with neck pain. With a minimum 10-year follow-up, clinical and radiographic data were reported on 205 patients with a chief complaint of neck pain. Of that group, “79% had a decrease in pain, and 43% were pain free; however, 32% had moderate to severe pain.”7 The investigators noted that a specific injury and severity of the initial pain were suggestive of having an unsatisfactory long-term outcome.
In an earlier edition of this text, Rothman8 stated that “it does not appear that cervical disc degeneration is a brief, self limiting disorder, but rather a chronic disease, productive of significant pain and incapacity over an extended period of time.” DePalma and Subin9 reported in 1965 that among patients treated nonoperatively for “cervical syndrome,” only 45% of those presenting for treatment with a chief complaint of neck pain or neck with arm pain had a long-term satisfactory outcome. In a series of the results of anterior cervical discectomy and fusion (ACDF) for cervical spondylosis, DePalma and colleagues10 reported that 21% had complete relief at 3 months with nonoperative care, whereas 22% had no relief. In a 5-year follow-up study of patients presenting with significant complaints of pain secondary to cervical disc degeneration, Rothman and Rashbaum11 noted that 23% remained partially or totally disabled.
When one looks at more recent publications, these classic studies are mirrored. Walker and colleagues12 performed a randomized clinical trial of manual physical therapy and exercise compared with minimal intervention in 94 patients presenting with neck pain, with or without arm pain. At 1-year follow-up, 62% of patients perceived success with treatment, which means that 38% had persistent symptoms, and only 32% in the minimum intervention group perceived treatment success, which means that 68% had persistent complaints. A classic study of the natural history of cervical spondylosis by Lees and Turner13 and a review in the 1980s showed that patients presenting with cervical radiculopathy do not typically progress to myelopathy. Two thirds of patients treated with nonoperative care had consistent complaints of pain, although not severe in all.
Etiology
In relation to trauma, numerous patients are seen who have a rear-end mechanism motor vehicle accident as the etiology for their complaint of neck pain—that is, a “whiplash” injury. The Quebec Task Force on Whiplash-Associated Disorders produced a monograph concluding that patients should be reassured that whiplash-associated disorder is “almost always” self-limited and that it “rarely results in permanent harm.”14 In rebuttal, Freeman and colleagues15 performed a methodologic critique of the literature and stated, “there is no epidemiologic or scientific basis in the literature for the following statement: whiplash injuries do not lead to chronic pain, rear end impact collisions that do not result in vehicle damage are unlikely to cause injury, and whiplash trauma is biomechanically comparable with common movements of daily living.”
Although currently there is an emphasis on performing better designed studies of early nonoperative management of whiplash-associated injuries, a rich history of observational studies does not exist.16 McNab17 reported on 266 patients, out of an original group of 575 patients with soft tissue neck injuries, who were 2 years after settlement of court issues, so as to minimize the bias of legal secondary gain. Of these 266 patients, 145 were available for review, with 121 reporting persistent pain; at minimum, 45% (121 of 266) had symptoms 2 years after court settlement per their injury.17,18 In a similar type of study, Hohl19 noted that of 146 patients who had no pr-existing degenerative condition, 45% had persistent pain 5 years after injury, and in a continuing series from the United Kingdom following patients with whiplash injuries, 66% were noted to have complaints of pain at 2 years after injury, with 10-year follow-up revealing reports of “intrusive pain” and 28% “severe” pain in 12%.20–22 In a prospective Scandinavian series of 93 patients, Hildingsson and Toolanen23 noted complete recovery in 42%, mild discomfort in 14%, and significant residual complaints in 44%. Likewise, Jonsson and colleagues24 reported that 28% (14 of 50) of patients with whiplash distortions had persistent symptoms. Although changing from a tort to no-fault system, to eliminate compensation for pain and suffering, decreases the percentages with whiplash injury from a motor vehicle accident, Cassidy and colleagues25 wrote that the prognosis for individuals with whiplash injury is affected by “… Intrinsic factors such as age, sex, and initial intensity of the pain.” In a series on early aggressive care for patients with whiplash injury, Cote and colleagues26 noted that their “results add to the body of evidence suggesting that early aggressive treatment of whiplash injuries does not promote faster recovery.”
When seeing a patient with whiplash-associated injuries, it would seem that clinicians may counsel them that “usually” or “more often” their pain will subside as they heal themselves and that only a “low percentage” will have long-term permanent damage. This counseling is in contrast, however, to the wording that the patient “almost always” gets better and “rarely has permanent harm” as suggested by the Quebec Task Force.14 In perhaps 10% to 20% of an original whiplash injury population, a surgeon would benefit a patient by proceeding with a diagnostic evaluation to objectify specific anatomic pathologies that may be remedied with open or minimally invasive surgical intervention.
Patient Evaluation
History
One needs to assess the onset (traumatic vs. nontraumatic, acute vs. insidious) and the location of the pain and whether it is local, referred (basioccipital, upper trapezial, or periscapular), or radicular into the arm. A specific assessment of the component that is related to neck pain versus arm pain is crucial (e.g., 80% neck pain and headaches vs. 20% arm pain). Neurologic symptoms of numbness, tingling, weakness, sphincter dysfunction, or ataxia are sought. The pattern of pain is important. Is the pain worse with flexion activities? Does it increase as the day goes on and respond to rest? This finding would suggest a discogenic source, which is a common presenting condition. Unilateral radiation to the upper trapezial and interscapular region that restricts turning the head to that side suggests a radicular component. A history of a known diagnosis of cancer or infection is noted, and constitutional symptoms of night pain, rest pain, fever, and weight loss are reviewed. The social history documents the presence or absence of litigation, workers’ compensation activity, and use of tobacco. The family history may suggest a genetic predisposition. The patient’s self-reported documentation should be reviewed (e.g., pain diagrams, visual analog scale [VAS], self-reported functional scale, SF-36, patient expectations). The pain diagram can be very useful in the assessment of axial mechanical pain with the continuum of those suggesting an anatomic source that makes one think more of a surgical option versus those suggesting a nonorganic source where one thinks less of invasive testing to determine a surgical option (Fig. 39–1A).
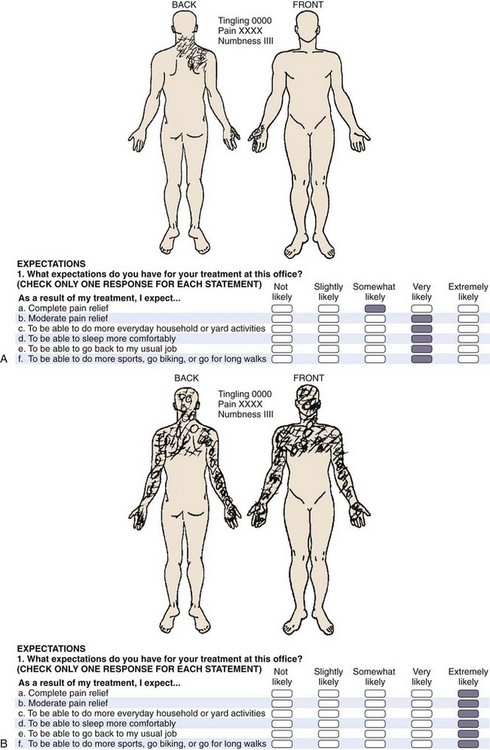
The psychosocial evaluation is critical. True malingerers are rare but do exist.27 Symptom amplification, drug-seeking behavior, work-related litigation, motor vehicle accident litigation, clinical depression, and frank psychiatric dysfunction all can have an impact on the patient’s self-perceived outcome as it relates to the success of elective surgical intervention for axial neck pain. A patient with a nonorganic diagram (Fig. 39–1B) who presents with a history of daily intake of high doses of narcotics, with active litigation, and who smokes two packs of cigarettes per day would suggest delay in surgical management. In a published series in 2002 on axial neck pain, the author and colleagues were unable to correlate a negative outcome with the presence or absence of litigation or cigarette smoking.28 A series from Cleveland documented that of patients who took daily narcotics for greater than 6 months, 51% (24 of 47) reported good to excellent outcome, and 32% (15 of 47) had a poor result.29 These findings contrast with patients without chronic narcotic use having 86% (38 of 44) good to excellent outcomes and no patients with a poor outcome.29
Radiographic Evaluation
The outpatient evaluation should be sequential. A history and physical examination are followed by plain radiographs before magnetic resonance imaging (MRI) or computed tomography (CT). The author routinely obtains an anteroposterior, lateral, and flexion-extension lateral radiographic series. Open-mouth or oblique views do not need to be routinely obtained. These radiographs are ordered for destructive processes that indicate tumor or infection (and the history of axial neck pain did not suggest such) or for the presence of foraminal stenosis, for which one would typically obtain advanced imaging. The presence of spondylosis, as evidenced by loss of disc height, subchondral sclerosis, cyst formation, or osteophyte formation, and the presence of listhesis with any dynamic component to suggest mechanical instability are documented. Using these factors, the author and colleagues have reported on a quantitive radiographic scoring system, which yields a cervical degenerative index.30,31 This objective assessment may be useful to follow patients regarding the progression of disease or patients who have had surgery regarding the development of adjacent segment degeneration. The index is an expansion of Gore’s assessment, and a higher score indicates more radiographic pathology at more levels. In a young patient with multilevel spondylosis, one would tend to encourage nonoperative treatment. The presence of spondylosis on radiographs is nonspecific and does exist in asymptomatic individuals, but the review of plain radiographs is still quite useful.32,33
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


