14 Subtrochanteric Fractures
Plate Fixation
Epidemiologic, Anatomic, and Biomechanical Overview
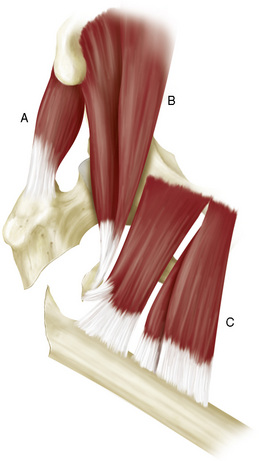
The treatment of subtrochanteric fractures remains a challenge because of the unique anatomic features of this area: the medial wall of the femur carries extremely high-pressure forces, whereas the lateral wall is subjected to strong tension forces. These anatomic and physiologic demands are induced by (1) the distribution of body weight through the femur into the hip and (2) the insertion of three major muscle groups to this region. These muscle groups are depicted in Figure 14-1. The strong abductor group of the gluteus medius and minimus muscles inserts into the major trochanter and comprises the major source of the pulling forces, the iliopsoas and adductor group at the lesser trochanter (piriformis, obturator externus, pectineus, adductor longus, and adductor brevis and magnus muscles).
Classifications and Stability
Lundy2 described subtrochanteric fractures as injuries of the proximal femur from the fossa piriformis to the isthmus. In older publications, the fracture was considered to occur more distally, between the lesser trochanter and 5 cm distal to it.3,4 The AO concentrated on an even smaller area, between the lesser trochanter and 3 cm distal to it.5
Biomechanically, the lateral cortical bone is subjected to high tensile forces, and the medial cortex is subjected to extremely high compressive forces.6 Hence, when developing potential therapeutic strategies, investigators must take into account that internal fixation techniques require substantial mechanical strength to support the significant forces exerted on the femur.
Several classifications for subtrochanteric fractures have been proposed.3,7 Most classifications distinguish between stable and unstable fracture types. Hence, the number of bone fragments and direction of fracture lines is the classifier for grouping injuries.
AO Classification
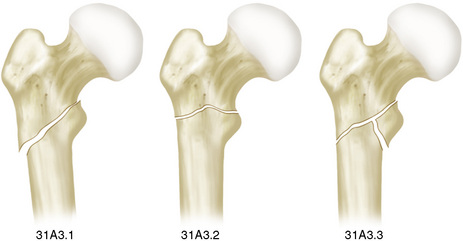
Within the AO classification system, Mueller8 proposed the designation 31 for the proximal femur and A3 for the extra-articular trochanteric region. According to this nomenclature, 31A3.1 represents the reversed fracture, which is considered unstable. The designation 31A3.2 represents a subtrochanteric fracture with a transverse fracture line visible on the anteroposterior radiograph, and 31A3.3 is a multiply fragmented comminuted subtrochanteric fracture with a separate fragment of the lesser trochanter (Fig. 14-2).
Russell-Taylor Classification
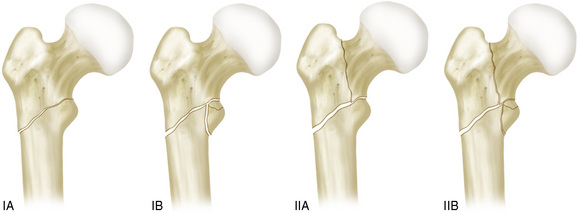
In the international literature, the Russell-Taylor classification is more widely used than the AO classification.9 This classification system is principally based on two issues: stability and fracture extension. Fractures without extension of the anteroposterior fracture line into the piriformis fossa are designated type I; the others are considered type II. In both types, fractures without comminution of the lesser trochanter are designated A, and those with comminution zone are B (Fig. 14-3).
Related posts:
 Investigation and Management of Postoperative Delirium
Investigation and Management of Postoperative Delirium
 Rehabilitation: Improving Outcomes for Patients Following Fractures of the Proximal Femur
Rehabilitation: Improving Outcomes for Patients Following Fractures of the Proximal Femur
 Femoral Neck Fractures: Treatment of Nonunion
Femoral Neck Fractures: Treatment of Nonunion
 Femoral Neck Fractures: Reduction and Fixation
Femoral Neck Fractures: Reduction and Fixation
 Subtrochanteric Fractures: Intramedullary Fixation
Subtrochanteric Fractures: Intramedullary Fixation
 Complications of Trochanteric Fractures
Complications of Trochanteric Fractures
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


