CHAPTER 83 Spinal Orthoses for Traumatic and Degenerative Disease
Orthoses are externally applied devices that serve to restrict motion, correct deformity, or improve function in a particular body segment.1 Spinal orthoses for treatment of traumatic or degenerative disease primarily function to restrict motion through externally applied force. They have played an integral role in the management of spinal pathologic processes for thousands of years. Smith, in his 1908 article “The Most Ancient Splints,” described brace use in ancient Egypt more than 2500 years ago.2 Much of the early literature focused on treatment of spinal deformities including Galen’s chest-strapping method and Paré’s leather-lined metal jacket, popular in the late 16th century.3 Nicholas Andry developed the “iron cross,” consisting of a straight metal upright with a cross and metal ring attached to the top for support of the head, in the early 18th century for cervical immobilization.4 Today, spinal bracing continues to be a mainstay of treating deformity (covered elsewhere in this text) and the management of traumatic and degenerative spinal disorders.
Spinal orthoses can be broadly categorized on the basis of the body segment they are employed to immobilize: cervical (CO), cervicothoracic (CTO), thoracolumbosacral (TLSO), lumbosacral (LSO), and sacroiliac (SIO). This chapter focuses on the biomechanics, laboratory studies, and the classic and recent clinical results of commonly used, commercially available spinal orthoses. The U.S. Food and Drug Administration has classified spinal orthoses as class I devices. As a result, they have not been subject to the strict regulations and scrutiny applied to implantable devices. The currently available knowledge on these devices is the product of observations of varying degrees of scientific merit. Additionally, many commercially available products do not have peer-reviewed data to support their purported effectiveness. The prosthetics and orthotics community has produced numerous publications in print and online trade journals regarding their products and design developments, but comparatively little is published in medical journals familiar to practicing spine specialists. We recently conducted a Medline search covering the past 10 years using the key words “spinal orthoses.” This search yielded 579 unique results. A similar search restricted to new listings over the past year using the online search engine “Google” yielded 607,000 “hits.” The paucity of readily available peer-reviewed literature has presumably contributed to the variability of prescribing patterns among spine specialists. Bible and colleagues5 recently illustrated this point using a questionnaire study of the postoperative bracing preferences among spine surgeons. Most of the respondents braced their patients postoperatively, but there was no consensus on the type, duration, or indications for bracing. In this chapter, therefore, we have attempted to discuss the available data and review design features of various orthoses rather than make specific recommendations on the superiority of one commercial product versus another.
Biomechanics and Biomaterials
An improved understanding of spinal biomechanics has led to advances in spinal bracing. Conceptually, the spine can be thought of as a series of semirigid bodies interconnected by viscoelastic linkages. Spinal kinematics involves motion in six degrees of freedom, with rotation about three axes and translation along the three coordinates.6 For clinical considerations, testing (particularly involving human subjects) has generally been confined to three planes of motion: flexion-extension, axial rotation, and lateral bending.
The efficacy of a particular orthosis to limit spinal motion has been tested using various methods including radiography and goniometry. Standard radiography, typically using flexion-extension views, has been commonly employed. Cineradiography evaluates motion through the use of fluoroscopy. Goniometry uses external devices attached to the subject to measure spinal motion. It has been demonstrated to correlate fairly well with radiographic techniques7 and avoids exposing subjects to radiation. However, there is some decreased accuracy and lack of information on motion at any particular segment.
Because bracing attempts to control the position of the spine through the application of external forces, orthotic design must account for regional variations of the surrounding anatomy and accommodate vulnerable structures. This includes the vital soft tissue about the anterior neck, the rigid thoracic rib cage, the compressible abdomen, and the bony pelvis at the base of the lumbar spine. The surrounding soft tissue envelope has a substantial effect on the ability of an externally applied force to control spinal movement. Pressure measurements on the soft tissues may be an objective way to assess the fit of a spinal orthosis. The role of soft tissue pressure measurement as an index of applied corrective or stabilizing force, however, remains unclear.8,9 The intervening soft tissue envelope is also an area of potential complications with problems including breakdown, local pain, decreased vital capacity, and increased lower extremity venous pressure.10
Along with our improved understanding of the biomechanics of spinal bracing, improvements in the materials available for brace manufacture have led to dramatic advancements in their design. During the 18th century, braces were generally constructed of leather, iron, and wood. German developments in the 19th and early 20th centuries led to many new brace designs with paper cellulose and glue being added to wooden or iron frames.4 Newer composite materials, polymer resins, and thermoplastics have led to a proliferation of commercially available orthoses that are lightweight and comfortable without sacrificing the stability afforded by the heavier, more cumbersome designs of the past. Commonly used materials in the fabrication of orthoses are listed in Box 83–1.
Beyond the advancements in our understanding of biomechanics and biomaterials, advances in computer engineering have led to innovative methods for customized production of orthoses with decreased time requirements. At the primary authors’ institutions, efforts to limit the length of inpatient admissions have necessitated a close working relationship between the treating physicians and the orthotists. A computerized database of key measurements that have been recorded over the years has allowed our orthotists to develop digitized models of various sizes and body types using computer-aided design/computer-aided manufacturing technology (CAD/CAM). Using this approach, simple measurement at the sternal notch, xyphoid, and waist along with linear measurements can be performed and integrated with CAD-CAM technology to rapidly design a precision fit orthosis in a fraction of the time needed for standard mold-based orthoses. Recent studies have evaluated this approach for bracing patients with idiopathic scoliosis. Braces comparable with those made using traditional mold techniques (in comfort and curve correction) could be produced in roughly one third of the time previously required.11 Continuing advancements in this area have included the development of handheld three-dimensional laser imagers that use reflectors placed on the patient to capture shape information. This technology is already used in limb applications with efforts under way to apply this technology for spinal applications.
Cervical Orthoses
The cervical region provides a challenge for externally applied spine immobilization due to the soft tissue structures about the neck and high level of mobility of the spine segments. Cervical orthoses can be divided into two broad categories: soft and rigid. Soft collars provide comfort and proprioception, but little immobilization, decreasing flexion and extension by 5% to 15%, lateral bending by 5% to 10%, and axial rotation by 10% and 17%.12 They are often used in the treatment of whiplash-type injuries or muscular strains about the neck, where proprioceptive feedback helps “remind” a patient to voluntarily restrict motion. The use of soft cervical collars in the management of cervical myelopathy is controversial.
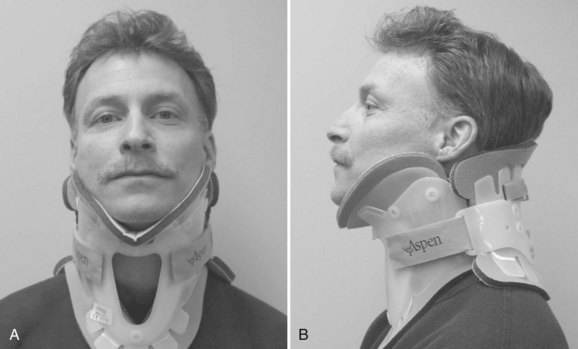
Rigid cervical orthoses are available in several forms, but all forms must be able to accommodate the vital soft tissue structures in the neck while simultaneously providing rigid immobilization of the mobile cervical spine. This is generally accomplished by firm seatings about the base of the skull and upper thorax connected by a rigid column. Most include an anterior opening to accommodate a tracheostomy tube. Rigid cervical orthoses are generally used to provide stabilization to the midcervical spine. Examples of cervical orthoses include the Philadelphia collar (Fig. 83–1), the Miami J collar (Fig. 83–2), the Aspen cervical orthosis (Fig. 83–3), and the Malibu collar (Fig. 83–4).



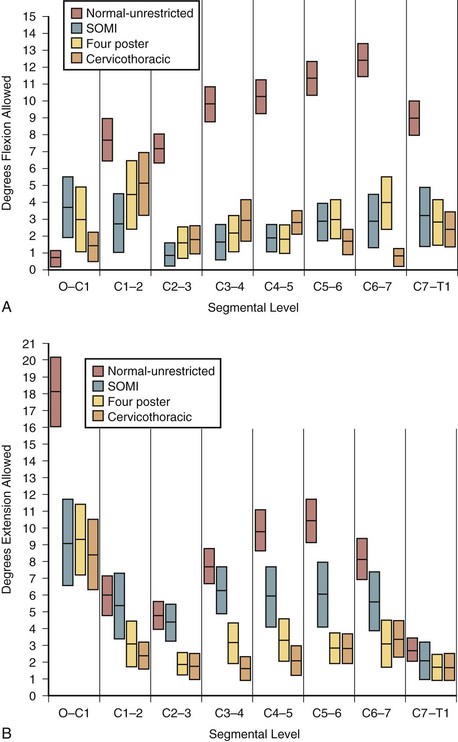
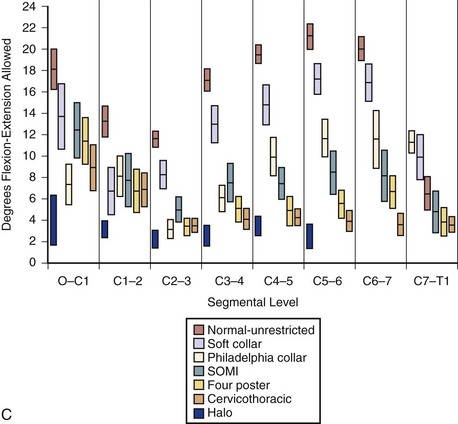
The classic study evaluating the effectiveness of various orthoses in immobilizing the cervical spine was performed by Johnson and colleagues.13 The methods of this study have often been emulated and its results frequently quoted since its publication in 1977. The authors evaluated the soft collar, Philadelphia collar, four-poster orthosis, sterno-occipito-mandibular immobilizer (SOMI), and a cervicothoracic orthosis. They used radiographs and overhead photographs taken at the extremes of motion in flexion-extension, rotation, and lateral bending. They quantified sagittal plane motion for each brace at every level of the cervical spine (Fig. 83–5). As others had demonstrated, they found that a soft collar offered no restriction of motion in any plane. They found that increasing the length of the orthosis (extending it onto the thorax) and increasing the rigidity of the connection improved the flexion control, but lateral bending and total flexion and extension were less controlled. They also demonstrated increased motion between the occiput and C1 in all the braces compared with the unbraced state. This “snaking,” or paradoxical motion, has subsequently been described throughout the cervical and thoracolumbar spine.14–16
Another study by Askins and colleagues17 compared five commonly used cervical orthoses in terms of their efficacy in restricting cervical motion. Radiographic and goniometric measurements found the NecLoc orthosis to be superior to the Miami J, Philadelphia, Aspen, and Stifneck orthoses in terms of flexion-extension, rotation, and lateral bending. The Miami J collar was also found to be significantly superior to the Philadelphia and Aspen orthoses in extension and combined flexion-extension.
A recent article by Bell and colleagues18 using electromagnetic sensors investigated the adverse effects of an ill-fitting Miami J cervical orthosis. The authors compared motion in healthy subjects using a Miami J of correct size to one too small and one too big, among other orthoses. They found that the ill-fitting cervical orthoses allowed significant increase in motion in multiple planes when compared with the correctly sized Miami J. The authors reiterated the importance of correct fitting of a cervical orthosis to avoid the potentially detrimental effects of excessive motion.
Known complications of cervical orthoses include skin breakdown over bony prominences such as the occiput, mandible, and sternum. Skin breakdown is especially prevalent in multitrauma patients with prolonged recumbency and in patients with altered sensorium. One study reported orthosis-related decubiti in 38% of patients with associated severe closed-head injuries.19 Molano-Alvarez and colleagues20 reported a 23.9% incidence of pressure sores in their series of patients with acute cervical spine injury placed in a cervical collar. The pressure sores were found on average at day 7 and were most frequently noted over the chin, occipital, and suprascapular areas. The authors found that pressure sores were associated with a higher injury severity score, longer time on mechanical ventilation, longer stays, and a greater percentage of patients with catheters for intracranial pressure monitoring. In addition, days spent in a cervical collar and presence of edema are thought to be significant predictors of skin breakdown.21 Plaisier and colleagues22 compared the skin pressure associated with the use of the Stifneck, Philadelphia, Miami J, and Aspen/Newport collars in supine patients. They found that the Miami J and Aspen collar produced the lowest chin and occiput pressures, both being below the mean capillary closing pressure.22 Tescher and colleagues23 assessed the effects of four commercially available cervical collars on mandibular and occipital tissue-interface pressure using custom-sized pads from a proprietary capacitive pressure-sensing transducer system. These authors found that the Miami J with and without Occian back had the lowest levels of mandibular and occipital pressure when compared with the Aspen and Philadelphia.23 Recently, increased intracranial pressure as a consequence of rigid cervical orthotic immobilization has been described. Hunt and colleagues24 studied the effects of rigid collar placement on intracranial pressure in head-injured patients. They found that rigid collars cause a small but significant increase in intracranial pressure, which may have deleterious effects in patients with severe head injuries and preexisting intracranial hypertension. They recommend early removal of rigid collars from head-injured patients once cervical spine injury has been excluded. Aspiration and dysphagia are at times anecdotally attributed to cervical collar use, but studies have been inconclusive. When using healthy volunteers performing swallowing studies, some mechanical changes in swallowing physiology were noted but no aspirations occurred.25 A causal link between cervical collar use and aspiration in injured or elderly patients has been suggested but not proven.
Methods for immobilizing the cervical spine of patients in the field have also been extensively studied. These include use of a cervical collar, a short board or sand-bag technique, or a combination of a collar and short board. Cline and colleagues26 compared the Hare extrication collar, the Philadelphia collar, and their immobilization protocol, which consists of a short board with forehead and chin straps. They concluded that the short board with straps provided the best immobilization and that the addition of a Philadelphia collar did not provide additional benefit. Podolsky and colleagues27 used goniometry to evaluate the immobilization provided by soft collar, hard collar, Philadelphia collar, Hare extrication device, and their sand-bag technique (which uses a board plus forehead tape). They found the sand-bag technique provided the most effective immobilization but that the addition of a Philadelphia collar provided additional benefit.27
The role of cervical collars following surgery for degenerative disease is an area of ongoing investigation and controversy. Bible and colleagues5 in their questionnaire of orthosis usage among spine surgeons found that orthoses were more often used after anterior cervical spine procedures as the complexity of the procedure increased. Campbell and colleagues28 evaluated the effect of a cervical collar after single-level anterior cervical fusion with plating on fusion rates and clinical outcomes in a U.S. Food and Drug Administration–regulated, multicenter controlled trial. They found similar clinical outcome parameters and a trend toward higher rates of fusion in the nonbraced group compared with those treated with a cervical collar. In addition, there was no difference between the proportion of patients returning to work.
Cervicothoracic Orthoses
Cervicothoracic orthoses (CTOs) generally consist of occiput and chin supports attached to anterior and/or posterior thoracic plates. Examples include the sterno-occipito-mandibular immobilizer, or SOMI (Fig. 83–6), the Minerva brace (Fig. 83–7), and the Yale brace (Fig. 83–8). Compared with cervical orthoses, these devices improve control in all planes of motion and are particularly suited for immobilization of the middle to lower cervical spine and upper thoracic spine. This improved rigidity, however, comes at the expense of patient comfort. Some of the earlier authors distinguished between the two/four-poster designs and those with more extensive connections between the head and thoracic components.13 The more recent, standardized classification system, however, categorizes the poster braces as CTOs along with the other designs. The traditional four-poster brace was shown to limit 79% of overall cervical flexion-extension and limit midcervical flexion to a comparable degree as the more rigid CTOs.1,29 Because of their heavy design and high resting pressures on the chin and occiput,7 this brace is less commonly used today.



The SOMI (see Fig. 83–6) uses metal uprights to connect occipital and mandibular rests to a sternal plate that is secured to the thorax by padded metal “over-the-shoulder” straps and additional circumferential straps that cross in the back. Because there is no posterior thoracic plate, the occipital rests are supported by uprights from the sternal piece. This results in adequate control of flexion but deficient control of extension throughout the cervical spine.13,29 These braces are fairly comfortable to patients but are associated with high resting pressures at the chin and occiput.7
The original Minerva brace consisted of a heavy, custom, plaster jacket that created difficulties in maintaining patient hygiene and obtaining radiographs.30 As a result of the difficulties encountered in managing patients with this device, the halo came into popular use. Later, the thermoplastic Minerva body jacket (TMBJ) was developed. It preserved the noninvasive nature of the original concept, and its lightweight, bivalved, Polyform shell allowed improved patient comfort and hygiene and interfered less with follow-up radiographs.31 Donning this brace is somewhat complex, often requiring an orthotist for proper application. More recently a prefabricated version of the Minerva body jacket, the Minerva CTO (see Fig. 83–7), has been developed. Its design features a forehead band attached to a large occipital flare. Sharpe and colleagues32 reported that this orthosis limits overall sagittal plane motion by 79%, axial rotation by 88%, and lateral bending by 51%.
The Yale brace (see Fig. 83–8) was originally designed as a modified Philadelphia collar with custom-molded anterior and posterior polypropylene thoracic extensions.33 The modern version is prefabricated and usually made of Kydex. Although lighter and less cumbersome than most of the other CTOs, the Yale brace has similar efficacy in controlling motion. In Johnson’s study, the Yale brace restricted 87% of overall flexion-extension, 75% of axial rotation, and 61% of lateral bending.34 Whereas the CTOs have been shown to be fairly effective at limiting motion of the cervical spine, they should not be expected to rigidly immobilize below the C7-T1 level despite their thoracic components.
Halo Vest
It is generally agreed that the halo vest provides the most rigid immobilization of the cervical spine of all the currently used orthoses and is particularly effective in the upper cervical spine. Originally inspired by a device used by Bloom to treat facial fractures in pilots with overlying burns during World War II, modified versions were used by Perry and Nickel to immobilize patients with polio who had undergone posterior cervical fusion.35,36 The early halo devices consisted of a circumferential stainless steel ring with four pins for skull fixation. The ring was attached to a plaster jacket by upright posts.37 Numerous improvements have been made to the various components of the halo vest, but the overall design principles remain the same. A ring is fixed to the skull with multiple pins. The ring is then attached to a vest by four connecting rods. Newer rings are made of composite materials, which have the beneficial properties of light weight, radiolucency, and compatibility with magnetic resonance imaging. There does not appear to be a difference in fixation strength between newer radiolucent graphite rings and the earlier titanium ones.38 Rings that are open posteriorly, or have crown-type designs, have been developed and are frequently used. These designs allow for ease in placement because the head of the patient does not need to be passed through the ring. Additionally, because the patient is not lying on the back of the ring, there is less risk of cervical spine fracture displacement through ring manipulation.
The initial halo vest was fashioned from heavy plaster of Paris. With the development of plastic technology, lightweight, easily applied vests of various sizes based on chest circumference have been fabricated (Fig. 83–9). Adjustable straps and supports help customize the fit. The connecting rods have been anodized to prevent seizing of the metal during tightening. The connecting rods in many designs are made of carbon fiber for their radiographic lucency, as well as for compatibility with magnetic resonance imaging. Torque wrenches are included in the application sets to prevent overtightening of the bolts that connect the rods to the vest and the ring. Mirza and colleagues39 found that most commercially available vests provide comparable immobilization. Factors that they associated with decreased motion include increasing vest snugness, decreasing the deformability of the vest, and appropriate fit and application.39

FIGURE 83–9 The halo vest (Bremer). This crown type design allows easier placement in the supine position.
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


