CHAPTER 19 Anterior Exposure to Lumbosacral Spine
Anatomy and Techniques
Anatomy
Vascular Anatomy: Variability, Bifurcations, Iliolumbar Vein, Segmental Vessels, and Middle Sacral Vessels
Surgical Approach
Preoperative Considerations
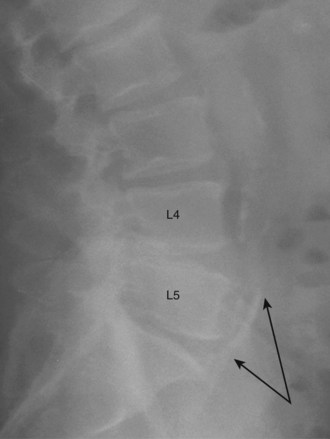
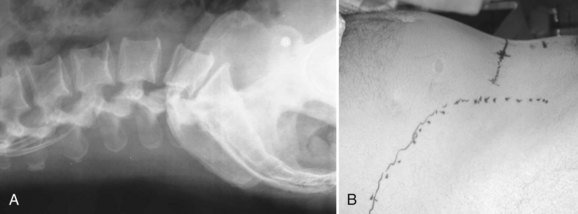
Communication is the mainstay to a successful partnership between the spine surgeon and access surgeon and the supporting surgical team. Before the day of surgery, relevant radiologic imaging will have been obtained and reviewed to determine the surgical plan. Any additional imaging should be pursued at that time to take into account disease processes that the patient may have. Examining plain films for signs of arterial calcifications, which may provide indirect evidence of vascular disease (Fig. 19–1), is particularly useful for the access surgeon. Additionally, the plain film should be evaluated for osteophytes and spondylolisthesis, which can exaggerate misleading anatomic bony features or be an indicator of potential inflammatory changes. A thorough vascular examination should be repeated at the time of surgery. Pulse oximetry on the patient’s left lower extremity is a useful adjunct for monitoring arterial flow distal to the area of dissection. Positioning of the patient is important to facilitate intraoperative placement of personnel, fixed retraction, and fluoroscopy machines.
Open Approaches
Retroperitoneal
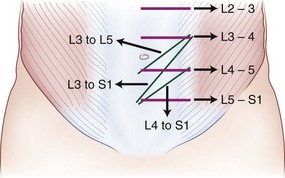
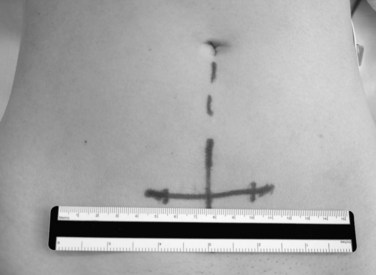
The retroperitoneal approach can proceed from various incisions, including vertical midline, paramedian, oblique, and transverse. Extensive lateral incisions should be avoided because this may denervate medially situated rectus muscle. The incision needs to take into account the spinal level and the number of lumbar levels to be exposed. An infraumbilical transverse incision can accommodate most approaches to the L4-5 and L5-S1 disc levels, whereas a more obliquely oriented incision is favored for access to disc levels above L4 (Figs. 19-2 and 19-3). This incision allows for access to the L2-3 disc level and possibly L1-2 disc level in patients with a favorable body habitus.
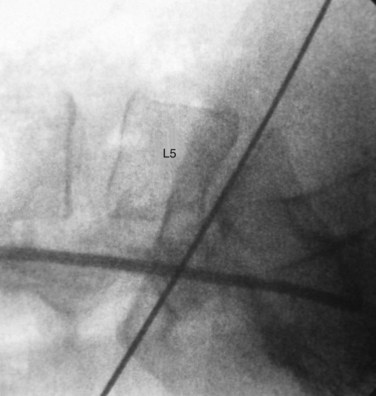
Lateral fluoroscopy can be used to assess the level of the incision (Fig. 19–4). This imaging is done in conjunction with a radiopaque probe or rod to determine the angle of the approach and level, which can be marked on the patient’s abdomen. Fluoroscopy can be especially important in obese patients because there may be no other anatomic landmarks palpable to guide the placement of the abdominal incision (Fig. 19–5). In most nonobese patients, palpation by an experienced access surgeon can be used to locate the sacral prominence to identify the L5-S1 disc space. A transverse approach to the L4-5 level should be directed at approximately the level of the superior anterior iliac spine, although fluoroscopic confirmation should be used if there is any question. All of the landmarks can be confirmed by fluoroscopic guidance, and fluoroscopy is especially important in patients who have distorted spine anatomy, had prior spine surgery, or are obese.
< div class='tao-gold-member'>

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


