82
Polydactyly and Bifid Thumb
Kevin D. Plancher
History and Clinical Presentation
A 2-year-old girl presents for evaluation of her duplicate thumb. The family recently moved from the Dominican Republic. The mother reports that her uncle had the same condition.
Physical Examination
The patient has an obvious deformity of the thumb (Fig. 82–1). The forearm and hand are one half the width of the other arm. There is no other malformation on the child’s hands or feet. The patient was referred for a complete genetic workup. The hand itself is fully functional.
Diagnostic Studies
Radiographs show a single but widened metacarpal with a bifid proximal phalanx (Fig. 82–2). Hematologic indices, including complete blood count with differential, platelet count along with prothrombin time (PT), and partial thromboplastin time (PTT), were checked preoperatively to rule out thrombocytopenia or any coagulopathy.

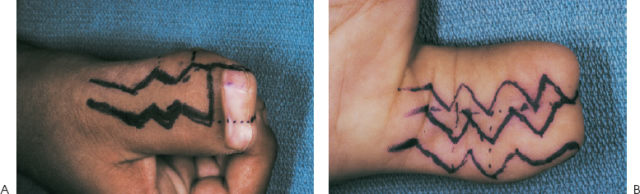
Figure 82–1 The patient’s widened thumb.

Figure 82–2 Radiographs show a single but widened metacarpal with a bifid proximal phalanx.
PEARLS
- For symmetrical thumb duplication, a Bilhaut-Cloquet (Fig. 82–3) technique is preferred; however, technical expertise is needed.
- Initial dissection should expose and retain all tissues until the anatomic orientation is exposed.
- After final determination is made to remove the more hypoplastic thumb, then safely ligate the neurovascular structures.
PITFALLS
- Ignoring a zigzag deformity can lead to additional complications.
- Recurrence of the deformity can be seen in reconstructions done prior to 18 months of age.
- Incomplete correction and instability at the reconstructed metacarpophalangeal joint
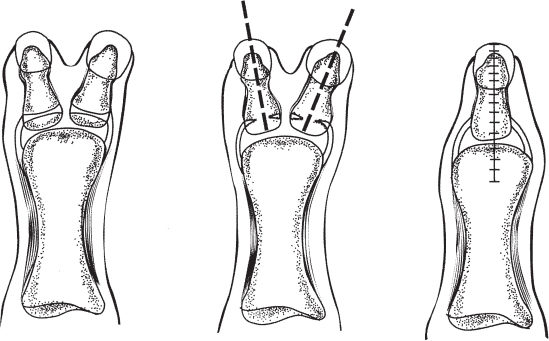
Figure 82–3 Distal phalanx with artwork showing the technique for a Bilhaut-Cloquet.
Differential Diagnosis
Duplicated thumb (classification system Table 82–1)
Diagnosis
Bifid Proximal Phalanx of the Thumb
Polydactyly is defined as duplication of a finger or part of it. It occurs as an isolated malformation, in association with other malformations of the hands and/or feet, or as a part of a syndrome. It is one of the most frequent congenital anomalies and is seen frequently in the hands. The prevalence of polydactyly with or without an associated malformation varies between 5 and 17 per 10,000 live births. The bifid thumb represents a complete or partial duplication of the thumb. It occurs in 1 per 3000 births.
| Type | Description | Frequency |
| I | Bifid distal phalanx | 2% |
| II | Duplicated distal phalanx | 15% |
| III | Bifid distal phalanx | 6% |
| IV | Duplicated distal phalanx | 43% |
| V | Bifid metacarpal | 10% |
| VI | Duplicated metacarpal | 4% |
| VII | Triphalangia | 20% |
Thumb polydactyly is classified by the Wassel classification (Table 82–1). The Wassel type IV is the most common followed by type VII and type II. Clinical appearance varies from a mild widening thumb to a complete duplication of the entire thumb. The radial half of the thumb is often more hypoplastic. There may be fibrous connections between the two thumbs. The nail may be one large nail, a conjoined nail, or a completely duplicated nail. The adductor pollicis and deep head of the flexor pollicis brevis typically insert on the ulnarmost thumb, and the abductor pollicis, the superficial head of the flexor pollicis brevis, and the opponens pollicis insert on the radial most thumb. The joints are stiff and the collateral ligaments are shared.
If surgical reconstruction is to be performed, the optimal age is between 1 and 2 years. At 6 months, gross grasp and grip are seen. At 1 year of age thumb and index function is seen, with voluntary release seen at 18 months. If surgical intervention is put on hold until 2 years, the neurovascular and tendinous structures are larger and complications may be fewer.
Nonoperative Treatment
Certain systemic abnormalities make surgical reconstruction contraindicated. These include Holt-Oram and Diamond-Blackfan syndromes and Fanconi’s anemia, which can be associated with duplicate thumb. In certain cultures, surgical reconstruction is also contraindicated. In the Asian culture, it is unethical to remove a body part. In these cases, adequate therapy must be provided to the child to allow for adequate hand function.
Surgical Treatment
An initial skin incision is made in a zigzag fashion beginning just distal to the carpometacarpal joint, based on the radial aspect of the hand (Fig. 82–4). The radial hypoplastic thumb is encircled and the incision is continued distally to joint the ulnar thumb. Anomalous tendons and neurovascular structures innervating the duplicate thumb should be identified. The neurovascular structures are ligated if the determination is made to ligate the hypoplastic thumb. The tendons are dissected back to their bifurcation.