Opening Wedge Osteotomy: Femoral
Valgus painful knee is a disabling condition affecting patients in every decade of life. The femoral osteotomy can represent the treatment of choice to correct the valgus deformity in young and middle-aged patients. The technique of opening wedge femoral osteotomy appears to be the most accurate and precise method for obtaining the required correction.
Indications
- Congenital femoral valgus
- Early cartilage deterioration after lateral meniscectomy
- Arthritis of lateral compartment in middle-aged individuals
Contraindications
- Elder patients (over 60 years)
- Osteonecrosis of the lateral condyle
- Arthritis involving femoropatellar joint and medial compartment
Physical Examination
- Valgus knee in standing position
- Pain at the lateral joint line
- Pain and swelling after mild activities or activities requiring standing for long periods
Diagnostic Tests
- Standing 45-degree posteroanterior flexion weight-bearing radiograph of both knees (Rosenberg)
- Standing anteroposterior radiograph of both limbs including hip and ankle joints
- >Magnetic resonance imaging (MRI) for evaluation of medial compartment and patellofemoral joint
- Arthroscopy (better if associated with the osteotomy)
- Adduction stress-radiograph at 30 degrees of flexion to evaluate the medial compartment
Special Considerations
- After the anesthesia has been induced, adduction-stress fluoroscopic view and arthroscopy can investigate the status of the medial compartment and confirm or not the opportunity for using the antivalgus osteotomy.
- Bone grafting from iliac crest is always required.
Preoperative Planning and Timing of Surgery
- Measurement of preoperative anatomic and mechanical axis of the valgus knee.
- Calculation of the required amount of correction (first in degrees and then in millimeters of wedge) to get a neutral femorotibial axis.
Special Instruments
- Power drill and saw
- Special retractor for the vastus lateralis
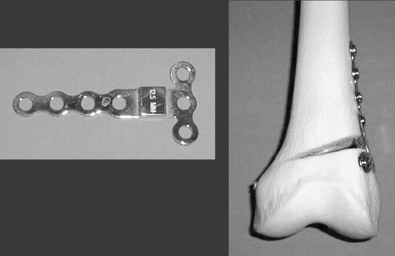
- Femoral plates with a central spacer ranging from 5 to 15 mm in width and seven holes for screws (Fig. 52–1)
- Graded wedge opener (Fig. 52–2) and osteotomy cutting guide, if required by the surgeon
Anesthesia
General anesthesia is preferable because bone grafting from iliac crest is required. Epidural anesthesia is an alternative.
Patient and Equipment Positions
- Patient is in a supine position on a radiotransparent operating table.
- Skin preparation of the free limb and of the iliac region
- Arthroscopic set; particular care in waterproof dressing
- Amplifier should be within easy access of the patient’s knee and hip.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


