Open Reduction of the Unstable Slipped Capital Femoral Epiphysis
Matthew P. Fishman
Ira Zaltz
Introduction
The current treatments for slipped capital femoral epiphysis (SCFE) include in situ pinning (1,2,3,4); open physeodesis (5,6); subcapital (7,8,9,10,11,12), basicervical (13,14), intertrochanteric (15), and subtrochanteric osteotomies (16); and open reduction and internal fixation (17,18,19,20,21,22,23). All forms of treatment are designed to stabilize the capital femoral epiphysis and either to maintain or to improve the anatomic relationship of the epiphysis to the proximal femur. Considering the current understanding of the natural history of the deformity, the ideal treatment, therefore, depends on the stability of the epiphysis and the degree of upper femoral deformity.
In situ fixation of both stable and unstable epiphyses using a threaded cannulated screw is the most prevalent current treatment because it is associated with the fewest complications and the lowest frequency of osteonecrosis following treatment (1,4). Recently, the beliefs that the persistent hip deformity following in situ fixation has a favorable long-term natural history and yields good patient function (3,24,25,26) have been questioned (27). Although some degree of upper femoral remodeling potential may gradually diminish the deformity (2,25,26,28,29), this mechanism does not reliably restore normal upper femoral anatomy (Fig. 49.1) (30). Contemporary data suggest the resultant deformity associated with a healed SCFE leads to femoroacetabular impingement, acetabular cartilage and labral damage, and the development of osteoarthritis of the hip (31,32,33,34,35,36,37,38). Accepting our current understanding of femoroacetabular impingement, open reduction and internal fixation of a SCFE is of renewed interest to restore upper femoral anatomy and eliminate femoroacetabular impingement (27). Historically, capital femoral epiphyseal reduction was associated with a higher risk of osteonecrosis compared to in situ fixation (39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54). Recently, a modification of Dunn’s technique of open reduction and internal fixation by means of surgical hip dislocation has produced favorable results with a low reported prevalence of osteonecrosis (17,18,19,20,22,23).
 Figure 49.1. Anteroposterior (A) and frog-leg lateral (B) radiographs of a patient who underwent in situ pinning for right SCFE demonstrate residual deformity in the anterolateral femoral neck which has been shown to be a source of femoroacetabular impingement, labral and cartilage damage, and early advancement of osteoarthritis. |
 Figure 49.2. Anteroposterior radiograph demonstrating avascular necrosis of the left hip following in situ pinning for SCFE. The contralateral hip was prophylactically pinned in situ and showed no signs of avascular necrosis. |
Natural History
The natural history of SCFE is a source of significant controversy. Current clinical data suggest that patients treated for mild to moderate deformities have satisfactory clinical results into middle age (4,26). Patients with severe deformity, complications following treatment, or who present with an unstable slip have a higher rate of associated complications and a less favorable natural history (4,55). The precise incidence of near-term complications is not known; however, osteonecrosis, slip progression, chondrolysis, fracture, and screw impingement are more prevalent following unstable and severe SCFE (Fig. 49.2). Post-SCFE femoroacetabular impingement that is caused by posterior epiphyseal displacement and metaphyseal prominence (Fig. 49.3) has been illustrated by Mamisch who used three-dimensional computer models to evaluate the deformity and showed that during hip flexion the anterior metaphyseal prominence abuts the anterior acetabulum. Mamisch also found two anatomic reasons for femoroacetabular impingement after SCFE: abnormally high epiphyseal slip angles as classified by Southwick (Fig. 49.4) (16) and loss of the normal concavity of the epiphyseal–metaphyseal junction (33). In another study using computer models, Rab (31) showed that moderate and severe posterior epiphyseal slips (greater than 25 degrees) are associated with impingement between the
anterior femoral neck and the acetabulum that is compensated by external femoral rotation of the hip (Fig. 49.5).
anterior femoral neck and the acetabulum that is compensated by external femoral rotation of the hip (Fig. 49.5).
 Figure 49.3. Prominence is evident at the epiphyseal–metaphyseal junction of the femoral neck in stable (A) and unstable (B) SCFEs. The red cancellous bone is exposed at the tip of the forceps. |
 Figure 49.4. The Southwick slip angle is determined by measuring the angle between a line parallel to the femoral shaft and a line perpendicular to a line from the edges of the epiphysis. The slip angle is the angle as determined in the affected hip minus the angle in the unaffected hip. The patient in this frog-leg lateral radiograph has a slip angle of 20 degrees (31 degrees as measured on the right hip, shown; -11 degrees as measured on the left hip, not shown). |
 Figure 49.5. Patient with SCFE exhibiting typical presentation of obligatory external rotation during flexion of the hip secondary to impingement of the anterior metaphysis on the acetabulum. |
Evidence exists that even mild slips may cause femoroacetabular impingement. Fraitzl (34) reviewed cases of mild slips treated with in situ fixation for radiographic evidence of femoroacetabular impingement. He documented average Notzli alpha angles of 86 and 55 degrees on anteroposterior and cross-table lateral radiographs, respectively, and concluded that mild slips are associated with radiographic evidence of femoroacetabular impingement.
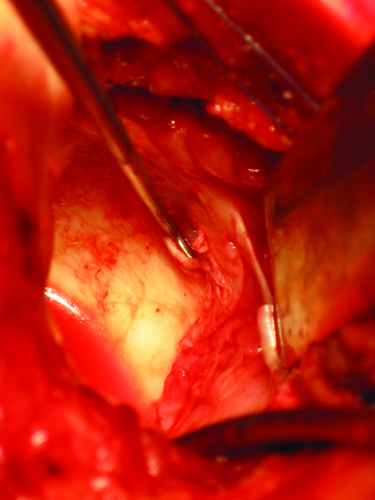 Figure 49.6. Unstable labral damage demonstrated by a probe in the acetabulum during surgical hip dislocation in a patient with residual femoral neck deformity following SCFE previously treated by in situ pinning without reduction. |
Femoroacetabular impingement is associated with damage to the acetabular cartilage and labrum. In a computer model showing anterior femoroacetabular impingement following SCFE, Rab (31) postulated the resulting impingement causes injury to the anterior acetabular labrum. Several reports have validated his conclusions by confirming injury to the acetabular cartilage. Arthroscopic visualization of the hip in patients with SCFE prior to treatment with in situ fixation has shown damage to the anterosuperior acetabular cartilage and posterolateral labrum (32). Under direct observation during surgical hip dislocation to treat previously fixed but persistently symptomatic SCFE, Sink et al. (36) documented labral damage in 87% of cases and damage to the acetabular cartilage in 85% of cases (Fig. 49.6). Leunig documented partial and full thickness articular damage following SCFE caused by the abnormally prominent anterior metaphysis of the femoral neck (Fig. 49.7




Related posts:

Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
