its initial development, increasing restrictions to joint mobility in the third trimester cause the biologically plastic femoral head to become more ellipsoidal. After birth, the range of motion increases and the spherical structure is restored (2).
Primary ossification centers for the three hip cartilaginous precursors appear in the ilium at 10 to 11 weeks, in the ischium between 15 to 16 weeks, and in the pubis at 19 to 20 weeks (3). Ossification is preceded by establishment of a fetal vascular supply for the developing hip at 10 to 11 weeks (4,<A onclick="if (window.scroll_to_id) { scroll_to_id(event,'R5-2'); retu variants in hip morphology associated with impingement will be offered.
Prenatal Femoral–Acetabular Development
Prenatal Acetabulum
Formation of the acetabulum occurs at approximately 6 weeks of embryonic development with the condensation of cells in the space between the prospective femoral head and the acetabulum which at this point is a cellular depression (1). Formation of the components of the pelvis occurs by endochondral ossification. Cartilage cells condense first in the centers of the primordial ilium, then the pubis, and finally the ishium. Central condensations containing chondrocytes migrate toward each other until fusion occurs with the ilium and ischium fusing first, followed by the ilium and the pubis. At the seventh week, the pubis and ischium centers join, leaving a small lateral opening which will become the apex of the developing acetabular fossa. It is noteworthy that the developing acetabulum follows the development of the head and shaft of the femur at all stages.
At 7 weeks, the femoral head has a spherical contour and the acetabulum develops rapidly around it (1). At this point the mesenchymal cells that separate femoral and acetabulum undergo cell death, yielding a fluid-filled channel that is the precursor of the hip joint. This is the earliest time in development when hip dislocation can occur. Although the femoral head is spherical during in spite of this, ossification of the acetabulum itself does not occur until adolescence.
In summary, the ischium, ilium, and pubis, from a functional developmental point of view, can be regarded as “squashed” long bones each with its own diaphysis, metaphysis, and epiphysis as illustrated (2).
Primary ossification centers for the three hip cartilaginous precursors appear in the ilium at 10 to 11 weeks, in the ischium between 15 to 16 weeks, and in the pubis at 19 to 20 weeks (3). Ossification is preceded by establishment of a fetal vascular supply for the developing hip at 10 to 11 weeks (4,5).
Prenatal Femur
By the eighth week the primary ossification center appears in the diaphysis of the developing femur. Ossification extends proximally and distally from this center and soft tissue elements of the hip begin to form. At this stage (1), cells near the femoral head form the precursor of the ligamentum teres along with the future traverse acetabular ligament below. The acetabular labrum, first visible at 6 weeks as a clump of cells along the outside of the acetabular rim, continues its development as the ilium, ischium, and pubis enlarge at 8 weeks (1).
By 11 to 14 weeks, blood vessels are observed entering the head and neck of the femur leading to eventual ossification of these regions (1). By 16 weeks, ossification of the femur is complete up to the level of the lesser trochanter, and primary ossification of three hip component bones has begun. It is noteworthy that,oral neck (Fig. 2.2) (2). During the neonatal period, the intracapsular joint is formed by the hip capsule attaching to the bone and cartilG” id=”F1-2″ id_xpath=”/CHAPTER[1]/TBD[1]/TLV1[2]/TLV2[2]/FG[1]”>
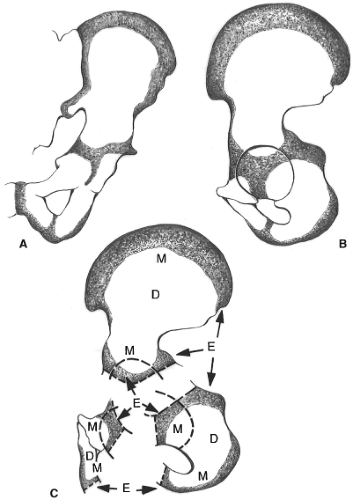 Figure 2.1. This illustration depicts the separate osseous entities from which the hip bone is composed. A: An anterior view does not permit a full appreciation of the acetabulum. B: In a true lateral view, a better grasp of the union of the separate components is apparent. C: An exploded view depicts the morphologic identity that each of the three component bones (ilium, ischium, and pubis) brings to the triradiate cartilage. E, epiphysis; M, metaphysis; D, diaphysis. |
Postnatal Development
Development of the hip in newborns is characterized by three important events from a clinical point of view: (1) development of the acetabular roof, (2) elongation of the femoral neck, and (3) ossification of the head of the femur.
In general, the femoral neck, from birth to age 16, elongates and widens by both appositional and interstitial growth. As growth occurs in longitudinal and lateral directions, remodeling of bone on the medial and lateral sides of the femoral neck maintains its shape (2).
After birth, the shape of the head of the femur is spherical with variable anteversion and the near absence of a femoral neck (Fig. 2.2) (2). During the neonatal period, the intracapsular joint is formed by the hip capsule attaching to the bone and cartilage beyond the acetabular rim. The femoral head is only slightly higher than the greater trochanter, and the proximal femur has already formed three distinct regions: (1) femoral head, (2) greater trochanter, and (3) intervening intraepiphyseal region. From 3 to 6 months, the acetabular labrum grows, stabilizing the hip joint, with the femoral head growing more on the medial side. The secondary ossification center of the femoral head forms at 3 months and continues to enlarge after 6 months. As this ossification center enlarges, the femoral head growth plate appears and separates the head from the greater trochanter.
 Figure 2.2. Neonatal proximal femur shows a hemispheric femoral head that is now slightly “higher” than the greater trochanter, reflecting the beginning of preferential development of the medial portion of the proximal femur. (Reprinted with permission from Katz JF, Siffert RS. Management of hip disorders in children. Philadelphia, PA: Lippincott; 1983.) |
During the second year, the femoral neck continues to elongate and the capitis femoris ligament enters the fovea capitis. Between 3 and 4 years, the greater trochanter forms a secondary ossification center and separates further from the femoral head. The interdigitating mammillary process in the femoral head growth plate also develops at this time. Between 5 and 8 years, the greater trochanter ossification center fuses with the main ossification center of the femur, whereas the ossification center of the femoral head continues to widen, mature, and grow radially. Between 9 and 12 years, the cartilage thins on the acetabular roof, forming a well-defined labrum, and interdigit”1″>Amount of cartilage between the ossified acetabular roof and the articular surface decreases. Labrum is well defined Interdigitation of the mammillary processes into the metaphysis ates of the femur close—the femoral head first, then the greater trochanter. Hyaline cartilage is replaced with bone except for a thin layer of articular cartilage (Table 2.1).
Get Clinical Tree app for offline access

Table 2.1 Summary of Hip Development from Birth to Adulthood | ||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
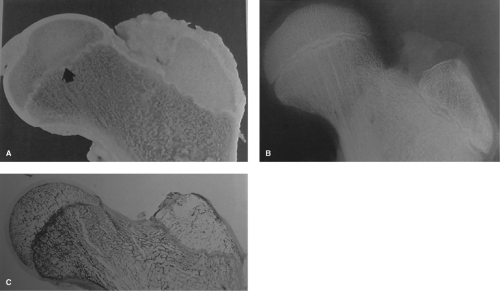 Figure 2.3. (A) Gross, (B) radiographic, and (C) histologic sections from a 15-year-old boy. Thickening of the bone on both sides of the capital femoral physis is evident radiographically and histologically. In the gross section, central bridging is apparent (arrow). The intraepiphyseal cartilage is still present and capable of function. (Reprinted with permission from Katz JF, Siffert RS. Management of hip disorders in children. Philadelphia, PA: Lippincott; 1983.) |
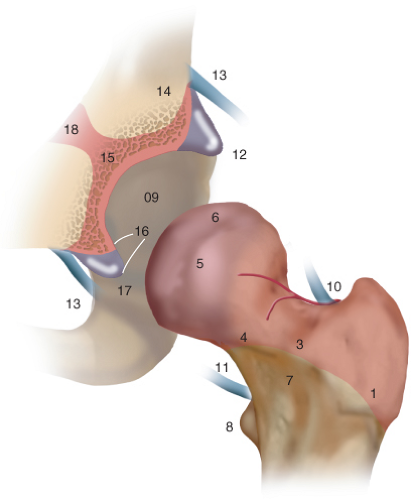 Figure 2.4. Schematic diagram shows areas where growth abnormalities may occur, as described by Katz and Siffert (6). 1, greater trochanter; 2, lateral growth of the physis; 3, growth of the midzone of the physis; 4, growth of the medial zone of the physis; 5, development of the lesser trochanter; 9, development of the articular surfaces of the proximal femur and acetabulum; 10, damage to the posterosuperior vessels; 11, damage to the posteroinferior vessels; 12, development of the acetabular labrum; 13, development of the capsule; 14, remodeling, particularly in the lateral side of the iliac metaphysis; 15, growth within the acetabular cartilage; 16, development of the ligamentum capitis femoris; 17, development of the transverse acetabular ligament; 18, development of the triradiate cartilage. All of these areas represent cellular zones where major growth defects may take place, leading to the various deformities of the hip discussed in subsequent chapters. |
There are many areas in the developing acetabulum and femoral head where growth abnormalities can occur. These are summarized in 8,9). At this point, capillaries have invaded the ligamentum teres and the fibrofatty tissue filling the acetabular fossa, known as the haversian gland or the pulvinar. This formation is believed to supply the femoral head as well, but studies have shown that it does not plar Timing
At 8 weeks of hip development, the early derivatives of the blastema, including the cartilages, perichondral tissues, and joint interzones, are free of blood vessels (7). The primary ossification center of the proximal femoral shaft appears, and blood vessels ramify over the outer surfaces of the perichondral tissues (1). Vessels do not enter the perichondrium until this layer alters in structure in preparation for the formation of periosteal bone (7). Capillaries first break through the periosteum at the level of the nutrient artery in the middle third of the femoral shaft. These vessels carry mesenchymal and hematopoietic cells into the bone marrow (1). Some vessels do appear in the fibrous capsules of the joints and are seen lying in the synovial mesenchyme. At 10 weeks of development, after the shoulder, elbow, and knee have begun to appear as joint cavities, the hip cavity spreads around the head of the femur and the ligamentum teres lies in this synovial mesenchyme accompanied by the conspicuous blood vessels, which will later supply the cartilage canals of part of the head of the femur (7). At 12 to 14 weeks, vessels invade the cartilage model of the femur and femoral head, forming the future medial and lateral circumflex vessels, the obturator, and the superior and inferior gluteal vessels (8,9). At this point, capillaries have invaded the ligamentum teres and the fibrofatty tissue filling the acetabular fossa, known as the haversian gland or the pulvinar. This formation is believed to supply the femoral head as well, but studies have shown that it does not play an important role in development (8). Soon after the 12th week of development, blood vessels enter the acetabulum, completing the special arrangement of blood vessels in the hip joint. It has been shown that the vessel configuration at this point is maintained throughout development and adulthood (1).
Vascularity of the Proximal Femur
The vascular organization of the hip joint can be divided into femoral and acetabular development. The proximal femur is supplied by three main groups of arteries: Arterial supply consists of the extracapsular ring, intracapsular cervical arteries, and intracapsular subsynovial ring (8). The extracapsular arterial ring is formed from the branches of the medial and lateral circumflex arteries at the base of the femoral neck. Thin cervical or retinacular vessels enter the hip capsule and travel along the femoral neck toward the head. These vessels are classified by their location relative to the femoral neck: lateral, posterior, medial, and anterior. The ascending cervical arteries pierce the femoral neck and travel distally to the metaphysis to either turn laterally to supply the greater trochanter, join the ascending nutrient vessels from the femoral shaft, or turn medially to supply the femoral neck. The ascending cervical vessels unite at the junction of the articular cartilage and the femoral neck, forming an intra-articular subsynovial arterial ring anastomosis. From this location, the epiphyseal and metaphyseal blood vessels branch in two directions. The epiphyseal supply crosses the perichondral ring superficially and enters the cartilage of the developing femoral head. The metaphyseal supply enters the femoral neck and travels distally (10,11,12,13).
The main difference between a child’s and an adult’s hip is the presence of a growth plate. This plate obstructs blood flow until it closes and allows the ascending cervical vessels to pass through it (1).
During development, the longitudinal growth plate (epiphysis) is avascular, but has a dual blood supply to aid in growth (7,14). The first source, epiphyseal blood vessels, supplies nutrients to the growth plate from above. The second, the metaphyseal blood vessels, flows up to the epiphysis from the periphery or from within the nutrient artery in the shaft of the femur. An additional source, the perichondral arteries of the perichondral ring of La Croix, supplies
 Diagnostic Categories and Definitions for the Adult Hip
Measurement of Treatment Outcomes in the Young Patient with a Hip Disorder
Hip Arthroscopy Anatomy and Access to the Central Compartment
Chiari and Salvage Osteotomy for the Treatment of Symptomatic Acetabular Dysplasia
FAI: Extra-articular Bony Impingement
Treatment of Slipped Capital Femoral Epiphysis Deformities in Skeletally Mature Patients
Diagnostic Categories and Definitions for the Adult Hip
Measurement of Treatment Outcomes in the Young Patient with a Hip Disorder
Hip Arthroscopy Anatomy and Access to the Central Compartment
Chiari and Salvage Osteotomy for the Treatment of Symptomatic Acetabular Dysplasia
FAI: Extra-articular Bony Impingement
Treatment of Slipped Capital Femoral Epiphysis Deformities in Skeletally Mature Patients




Related posts:
Diagnostic Categories and Definitions for the Adult Hip
Measurement of Treatment Outcomes in the Young Patient with a Hip Disorder
Hip Arthroscopy Anatomy and Access to the Central Compartment
Chiari and Salvage Osteotomy for the Treatment of Symptomatic Acetabular Dysplasia
FAI: Extra-articular Bony Impingement
Treatment of Slipped Capital Femoral Epiphysis Deformities in Skeletally Mature Patients
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree