FAI: Extra-articular Bony Impingement
Ernest L. Sink
Lazaros A. Poultsides
Introduction
Femoroacetabular impingement (FAI) has been most commonly described as a pathomechanical process where deformities at the femoral head and neck junction or acetabular rim induce injury to the hip cartilage and labrum with hip motion (1). The osseous abnormalities have been described in the context of a femoral-side cam deformity, and/or acetabular-sided overcoverage or pincer deformity. In the cam mechanism, the deformity creates an outside–inside pattern of inclusion injury at the labral/chondral junction as the head and neck junction enters the hip joint with hip flexion and rotation. In the pincer mechanism, an impaction injury occurs between a prominent acetabular rim and the proximal femur, inducing a crushing injury to the labrum and acetabular rim. The pathoanatomy causing cam and pincer impingement, as well as combinations of both, has been well described (2,3,4,5).
Hip pain associated with FAI is traditionally thought to result from intra-articular pathoanatomy and the resultant chondrolabral injury. Yet, we have also observed extra-articular forms of impingement in clinical practice and during surgical hip dislocation that clearly limits hip motion, compresses adjacent soft tissues, and impacts the acetabular rim. This is commonly observed as a conflict between the different facets of the greater trochanter and the acetabular rim, the anterior inferior iliac spine (AIIS), or the ischium. There may also be impingement of the soft tissues in these regions as the capsule and adjacent muscles become compressed with what is normally physiologic motion. Occasionally, extra-articular impingement can induce a pattern of instability. These may occur along with intra-articular impingement from the head/neck offset. The extra-articular bone does not enter the hip joint with motion, unlike a “cam” deformity. Therefore, the osseus abnormality does not directly injure the labral–cartilage junction. Labral or cartilage injury may happen secondarily with subluxation of the hip, as motion is limited by extra-articular impingement. This process has been observed in surgical hip dislocation in the hip with femoral anteversion. As the hip externally rotates and the posterior and superoposterior facet of the trochanter impinges on the ischium, the femoral head subluxates in the anterior direction. This anterior subluxation may cause increased tension on the anterior acetabular labrum and labral pathology and pain. In this scenario the iliopsoas tendon may act as a secondary stabilizer to the hip and the resultant tendon symptoms (6).
The goals of this chapter are to examine the pathomechanics of extra-articular impingement, discuss the common anatomic abnormalities that place the hip at risk, and describe diagnostic and treatment considerations.
Pathoanatomy
Pelvic Anatomy
The pelvis, acetabulum, and proximal femur have subtle variations between individuals. This is more apparent in the differences between the male and female pelvis. The female pelvis is wider to accommodate gestation and delivery. The femoral head is placed more medial to allow the hip center of rotation to be closer to the center of gravity, and thus the hip may be deeper or more overcovered than in males (1). Therefore, the acetabular rim may have a higher likelihood of impingement on the proximal femur.
AIIS has variations in its prominence and location in reference to the acetabulum. The description of this variation was published by Zaltz et al. (7). They described three different patterns and hypothesized that this region is commonly visualized at the crossover sign described by Reynolds et al. (8). When the AIIS is prominent or in close proximity to the acetabular rim it may act as a site of impingement. Arthroscopic observations by Larson et al. (9) support this mechanism by noting localized synovitis in the subspine region. The term subspine impingement has described the situation of impingement of regions of the proximal femur versus this AIIS and subspine region. With a shorter femoral neck, femoral retroversion, or a prominent anterior facet or intertrochanteric ridge, extra-articular regions of the proximal femur may impinge on the anterior acetabular rim or the AIIS with hip flexion or flexion/slight abduction and internal rotation.
Potential variations in size and location of the ischium may result in impingement of the greater trochanter against the ischium in external rotation. The inclination of the pelvic wing may also lead to impingement of the greater trochanter in different positions.
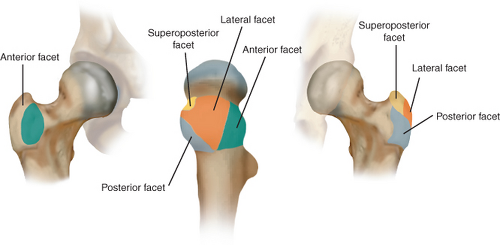 Figure 43.1. Facets of the greater trochanter. |
Proximal Femur
The most significant anatomic contributions to extra-articular impingement arise from the proximal femur and greater trochanter. There are many different variations in the greater trochanter. The greater trochanter consists of four facets: (Fig. 43.1) (10) (1) The anterior facet, which is variable in size. It is the location of one of the insertions of the gluteus minimus; (2) the posterior facet, which is the most and posterior aspect of the greater trochanter; (3) the lateral facet; and (4) the superior-posterior facet.
The classic example of a proximal femoral abnormality that limits hip motion and results in extra-articular impingement is Legg–Calvé–Perthes (LCP). In LCP the overgrowth of the greater trochanteric apophysis relative to the capital portion of the femoral physis results in a short, widened femoral neck and a large, more proximally positioned trochanter (Fig. 43.2). The proximal, overgrown greater trochanter may impinge on the ilium with abduction, limiting abduction. The anterior aspect and facet of the trochanter may impinge on the AIIS or the anterior aspect of the acetabular rim with hip flexion and internal rotation. The posterior aspect and
facet of the overgrown greater trochanter may impinge on the ischium or posterior/inferior ilium with external rotation. The result of trochanteric impingement is limitation in hip abduction and internal and external rotation (11).
facet of the overgrown greater trochanter may impinge on the ischium or posterior/inferior ilium with external rotation. The result of trochanteric impingement is limitation in hip abduction and internal and external rotation (11).
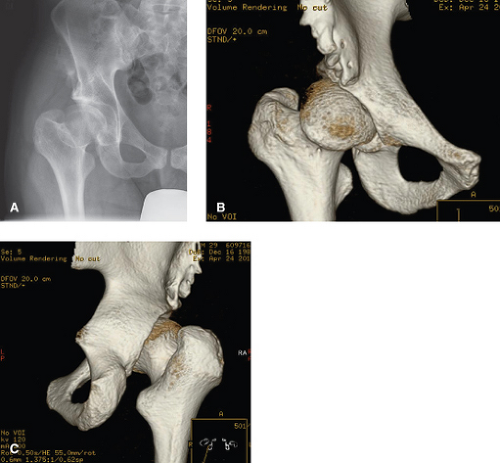 Figure 43.2. Anterio-posterior radiograph (A) and 3D CT scan (B,C) of a hip with residual Perthes deformity. The greater trochanter is larger and more proximal. The femoral neck is shorter and wider. |
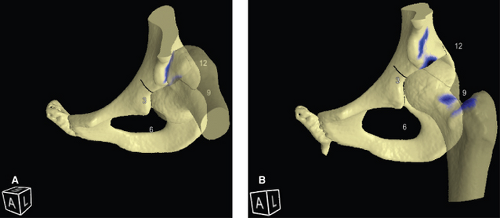 Figure 43.3. A 3D CT motion simulation of impingement of the anterior facet of the greater trochanter versus the lateral aspect of the AIIS (A) and the subspine region of the acetabular rim. The blue represents the region of bony impingement (B). Soft tissue impingement is not represented in this model. |
In the non-Perthes hip, more subtle variations in the position or the size of the greater trochanter and trochanteric facets may result in extra-articular impingement with physiologic range of motion. Variation in femoral neck length would also change the distance of the greater trochanter facets to the pelvis, potentially impacting the presence of trochanteric impingement with hip motion. Proximal femoral version also affects the location of the greater trochanter relative to the pelvis and contributes to extra-articular impingement. In proximal femoral anteversion, the greater trochanter may be more posterior and at greater risk of impinging with the inferior ilium or ischium (12). In retroversion, portions of the distal femoral neck or anterior trochanter may impinge on the anterior acetabulum with hip flexion.
Pathomechanics of Extra-Articular Impingement
Anterior Facet or Intertrochanteic Ridge on the Aiis/Anterior Acetabulum
A prominent anterior facet may impinge on the acetabular rim or the AIIS in hip flexion and internal hip rotation. This type of impingement occurs if the anterior facet or the AIIS is enlarged (Fig. 43.3




Related posts:

Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
