The nerve supply to the foot and ankle is provided by the branches of the sciatic nerve. The saphenous nerve, a branch of the femoral nerve, gives limited contribution. The branches of the sciatic nerve innervating the foot and ankle are the sural nerve, the superficial peroneal nerve, the accessory deep peroneal nerve, the deep peroneal nerve, and the posterior tibial nerve with its medial and lateral plantar nerves.
SURAL NERVE
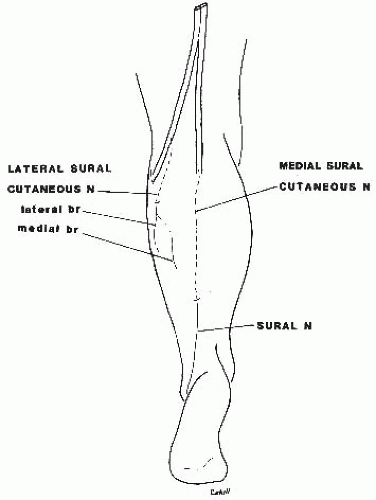
The sural nerve is formed by the union of the medial sural nerve—a branch of the tibial nerve—and the anastomotic peroneal communicating nerve arising from the lateral sural nerve or the common peroneal nerve (Figs. 8.1, 8.2 and 8.3).
When the anastomotic branch is absent, the medial sural nerve usually predominates and covers the territory of the sural nerve. Occasionally the lateral sural nerve or the peroneal communicating nerve takes over the same territory of innervation. The frequency of occurrence of such variations is as indicated in Table 8.1.
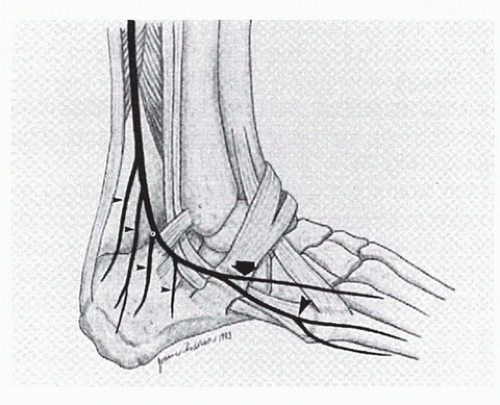
The medial sural nerve (median sural nerve, external saphenous nerve, tibial saphenous nerve) arises from the tibial nerve in the popliteal space. It courses between the two heads of the gastrocnemius muscle covered by the deep aponeurosis. It pierces the latter in the middle of the leg, receives the anastomotic peroneal communicating nerve, and forms the sural nerve. The sural nerve courses along the lateral border of the Achilles tendon and is anterolateral to the short saphenous veins. It turns around the posterior border of the lateral malleolus and passes 1 to 1.5 cm from the tip of the lateral malleolus, from which it is separated by the tendons of the peronei and their sheaths (Figs. 8.4 and 8.5). At the level of the tuberosity of the fifth metatarsal, the nerve divides into two terminal branches, lateral and medial (Fig. 8.6). The lateral branch is a direct continuation of the main nerve and terminates as the dorsolateral cutaneous nerve of the fifth toe. The larger medial branch obliquely crosses the dorsolateral aspect of the foot; it passes over the tendon of the long extensor of the fifth toe and divides over the anterior aspect of the fourth interosseous space into the dorsomedial cutaneous nerve of the fifth toe and the dorsolateral cutaneous nerve of the fourth toe.
The sural nerve provides the lateral calcaneal branches (Fig. 8.7). One such branch originates 5 cm above the lateral malleolus and another 1.3 cm above and behind the tip of the lateral malleolus in 98% of the cases.1 The sural nerve also supplies the lateral malleolar branch and an anastomotic branch that crosses the dorsum of the foot obliquely, passes under the dorsolateral vein, and unites with the lateral branch of the superficial peroneal nerve. Articular branches are provided by the sural nerve to the inferior tibiofibular joint, the ankle joint, and the talocalcaneal joint.
The anastomosis between the medial sural nerve and the peroneal communicating branch usually takes place at mid leg but may occur as low as in the lower quarter of the leg or as high as above the level of the knee joint.2
Avery common location of the sural nerve is at “10 cm above the tip of the lateral malleolus just at the lateral border of the Achilles tendon.”1 The diameter of the sural nerve is 2 mm average (1.25 to 2.75 mm), according to Kosinski, or 3 mm average according to Horwitz.1, 2
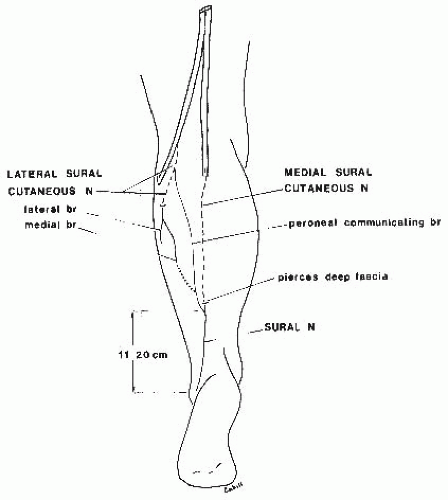
Ortiguela et al.3 investigated the anatomy of the sural nerve complex based on the dissection of 20 cadaveric limbs. All limbs had a medial sural cutaneous nerve and a sural nerve. A lateral sural cutaneous nerve was present in 19 of 20 limbs and, in 16 of 20 limbs, a peroneal communicating branch from the lateral sural cutaneous contributed to the sural nerve (Fig. 8.8).
The sural nerve was present in all specimens. In 80% of the specimens, it was formed by the union of the medial sural cutaneous nerve with the peroneal communicating branch at a point 11 to 20 cm proximal to the lateral malleolus (Fig. 8.8). In the remaining 20%, the sural nerve was simply the continuation of the medial sural cutaneous nerve (Fig. 8.9). The sural nerve coursed distally and laterally near the lesser saphenous nerve to pass 1.0 to 1.5 cm to the lateral malleolus. Two to 3 cm distal to the lateral malleolus, the nerve arborized into multiple cutaneous branches. The proximal diameter of the sural nerve ranged from 2.5 to 4 mm and distally from 2.0 to 3.0 mm.
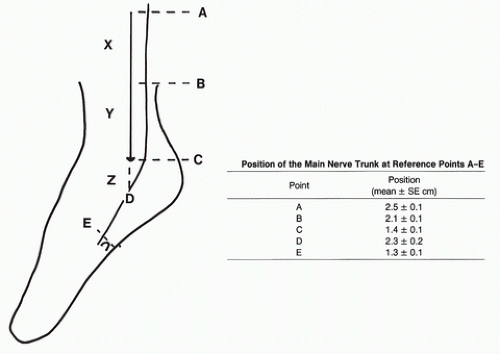
Eastwood et al.4 conducted an anatomic-metric study of the sural nerve based on the dissection of 20 preserved cadaveric limbs. As illustrated in Figure 8.10, the parameters were determined and the position of the nerve trunk at reference points A-E was defined as indicated in Table 8.3. Furthermore, the branches of the sural nerve were described as major (>2 mm), smaller branches as minor and their distribution was indicated in the defined reference zones of Table 8.2. This translates as two (1.9) major and two minor (2.15) branches posteriorly and as three (2.8) minor branches and 0.6 branches anteriorly.
The authors were able to describe 95% confidence limits for the course of the sural nerve trunk (Table 8.3). Thus a longitudinal incision in the region of the fibula should be in front of the anterior limits for the course of the main trunk. Therefore, it should not be more than 1.7 cm posterior to the fibular crest at 10 cm proximal to the lateral malleolus (point A), 1.5 cm posterior at 5 cm proximal to the tip of the lateral malleolus (point B), and no more than 0.6 cm posterior to the tip of the malleolus itself (point C). With the foot in equines, it should not extend more than 0.7 cm distal to the tip of the lateral malleolus (point D) if the main trunk is to be avoided. Similarly, an incision designed to pass posterior to the sural nerve should be behind the posterior limits of the position of the main trunk (Table 8.3).
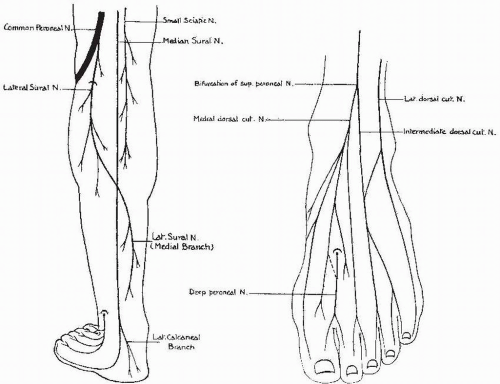
Figure 8.1 Sural nerve type A (53%) formed by the medial sural nerve only. The lateral sural nerve terminates in the posterior aspect of the leg. The sural nerve forms the lateral dorsal cutaneous nerve of the dorsum of the foot and provides an anastomotic branch to the intermediate dorsal cutaneous nerve—a branch of the superficial peroneal nerve, which is increased. (Kosinski C. The course, mutual relations and distribution of the cutaneous nerve of the metazonal region of the leg and foot. J Anat. 1926;60:274.)
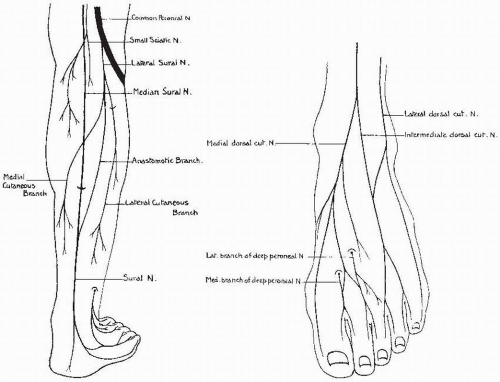
Figure 8.2 Sural nerve type B (40%) formed by two roots: the medial and lateral sural nerves, connected by an anastomotic branch. The sural nerve forms the lateral dorsal cutaneous nerve of the foot united to the intermediate dorsal cutaneous nerve by an anastomotic branch. The deep peroneal nerve is increased, with a medial branch innervating the first web space and a lateral branch innervating the second web space. (Kosinski C. The course, mutual relations and distribution of the cutaneous nerve of the metazonal region of the leg and foot. J Anat. 1926;60:274.)
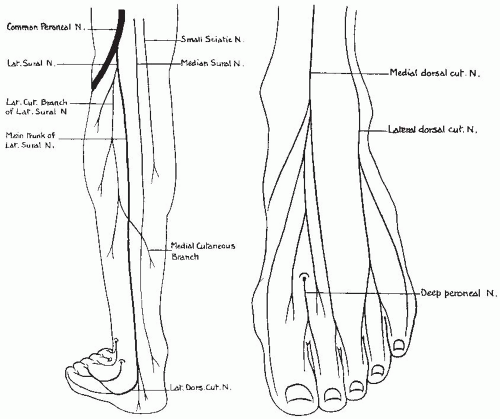
Figure 8.3 Sural nerve type C (6%) formed by the lateral sural nerve only arising from the common peroneal nerve. The sural nerve forms the lateral dorsal cutaneous nerve, which is increased. (Kosinski C. The course, mutual relations and distribution of the cutaneous nerve of the metazonal region of the leg and foot. J Anat. 1926;60:274.)
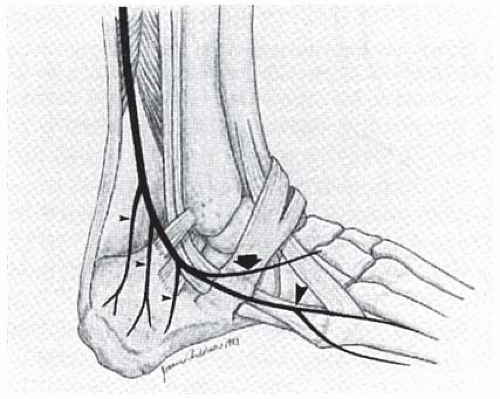
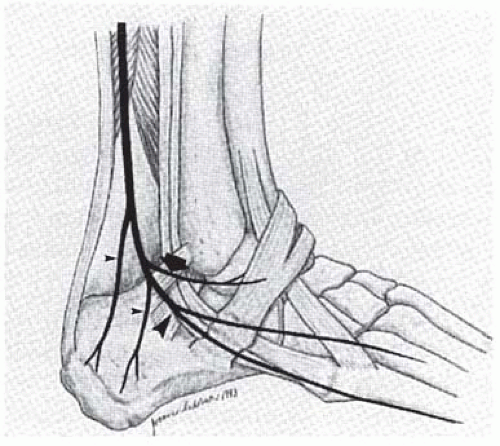
Lawrence and Botte5 investigated the course and branching patterns of the sural nerve based on the dissection of 17 cadaver specimens. At 7 cm proximal to the lateral malleolus, the sural nerve was at a mean 26.0 mm (range, 16-36 mm) posterior to the edge of the fibula. The lesser saphenous vein was located superficial and lateral to the nerve. At the same level, the sural nerve was 2 mm lateral to the lateral order of the Achilles tendon. In the retromalleolar region the sural nerve gave off an average of three branches (range, 1-5) that continued to the lateral aspect of the heel as lateral calcaneal branches (Figs. 8.11, 8.12, and 8.13). In 24% (one case) there was a lateral malleolar branch (Fig. 8.12). In the hindfoot the sural nerve was located at a mean distance of 14.0 mm (range 3-22 mm) posterior and 14.0 mm (range, 1-26 mm) inferior to the tip of the lateral malleolus.
TABLE 8.1 FREQUENCY OF OCCURRENCE OF SURAL NERVE OR OTHER NERVE FUNCTIONING AS SUCH
Functioning as Sural Nerve (%)
Author
No. Legs
Sural Nerve with Two Roots (%)
Medial Sural Nerve
Lateral Sural Nerve or Peroneal Communicating Nerve
Catania
94
51
35
14
Kosinski
287
40.2 (type B)
53.8 (type A)
6 (type C)
Andreassi
144
63.9
34.7
1.4
Sockolow
500
52.2
43.8
3.6
Mogi
180
83.3
16.7
0
P’an
286
81.5
13.3
5.2
Williams
257
83.7
15.9
0.4
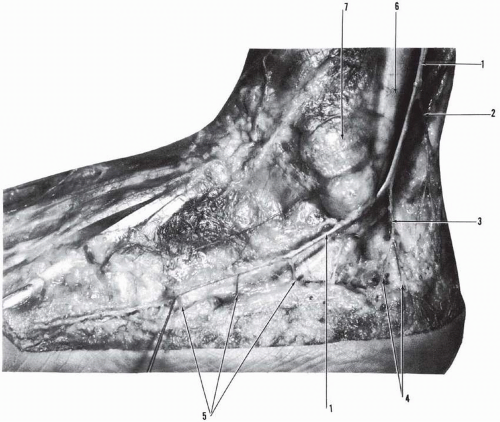
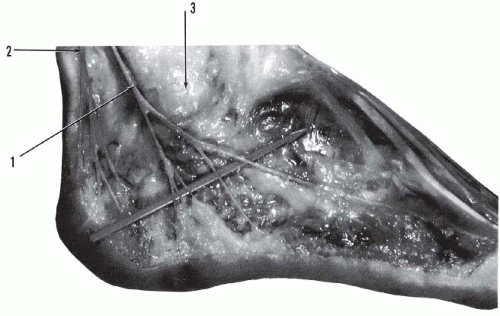
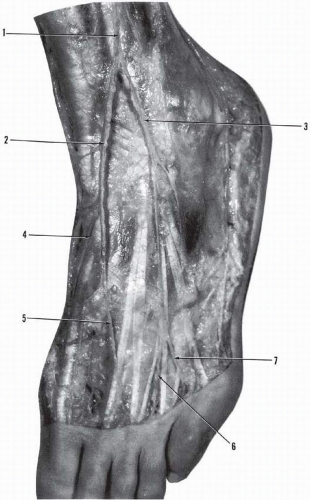
Figure 8.4 Sural nerve. (1, sural nerve; 2, branch of sural nerve to posterolateral aspect of Achilles tendon area and calcaneal region; 3, lateral calcaneal branch of sural nerve with bifurcation branches [4]; 5, branches of sural nerve to lateral border of foot; 6, peronei tendons; 7, lateral malleolus [sural nerve passes 1 to 1.5 cm below tip of lateral malleolus].)
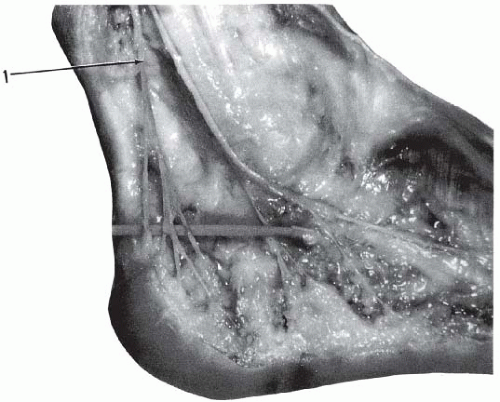
Figure 8.5 Sural nerve (1) dividing into lateral branches to the heel and the lateral border of the foot; lateral calcaneal nerve (2) dividing into multiple branches, lateral malleolar fat pad (3).
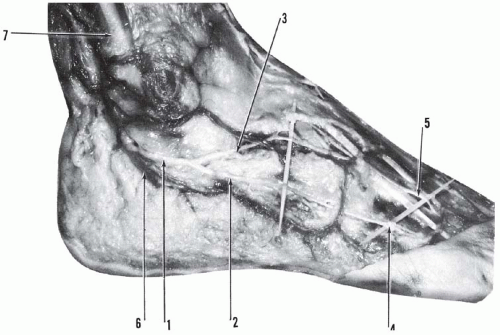
Figure 8.6 Lateral aspect of the right foot and ankle. (1, sural nerve dividing into lateral branch [2] forming dorsolateral cutaneous nerve [4] and medial branch [3] uniting with intermediate dorsal cutaneous nerve [5] of superficial peroneal nerve; 6, shorter saphenous vein; 7, peronei tendons.)
In the hindfoot, the sural nerve bifurcated and formed either terminal branches or a terminal branch and an anastomotic branch. A bifurcation or trifurcation occurred in 91% (16 specimens). An anastomotic branch traversing medially toward the sinus tarsi was present in 24% (four cases) and remained superficial to the extensor digitorum brevis. This branch either formed an anastomosis with the intermediate dorsal cutaneous nerve or arborized in the region of the sinus tarsi (Fig. 8.11). The lateral branch of the bifurcation continued toward the base of the dorsolateral branches of the fifth metatarsal.
Figure 8.7 Lateral calcaneal nerve (1) bifurcating into two branches: anterior and posterior. The anterior branch subdivides into four branches supplying the lateral and posterior aspect of the heel. The posterior branch is just lateral to the insertion of the Achilles tendon and supplies the lateral posterior aspect of the heel.
Figure 8.8 Cutaneous nerves on the back of the leg that contribute to sural nerve. In 3 of 10 cases, medial branch of lateral sural nerve was anastomosed to peroneal communicating branch. (From Ortiguela ME, Wood MB, Cahill DR. Anatomy of the sural nerve complex. J Hand Surg. 1987;12A(6):Figure 1.)
Figure 8.9 Formation of sural nerve as direct continuation of medial sural cutaneous nerve. (From Ortiguela ME, Wood MB, Cahill DR. Anatomy of the sural nerve complex. J Hand Surg. 1987;12A(6):Figure 5.)
Ikiz et al.6 conducted a comprehensive study of the sural nerve based on the dissection of 30 lower limbs. The sural nerve originated from the union of the medial and lateral cutaneous nerves of the leg which arise from the tibial nerve and the common peroneal nerve (see Fig. 8.19).
TABLE 8.2 TOTAL NUMBER OF POSTERIOR AND ANTERIOR BRANCHES OF THE SURAL NERVE IN 20 CASES
Site
Major
Minor
Posterior
X
7
9
Y
20
13
Z
11
21
Total
38
43
Anterior
X
0
12
Y
0
16
Z
13
28
Total
13
56
From Eastwood DM, Irgau I, Atkins R. The distal course of the sural nerve and its significance for incisions around the lateral hindfoot. Foot Ankle. 1992;13(4):200, Table 1.
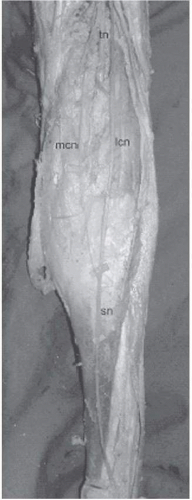
The lateral cutaneous nerve of the leg was present in 83.3% (25 specimens) and absent in 16.6% (five specimens) (Figs. 8.14 and 8.15). The origin of the lateral cutaneous nerve was an average 82.87 ± 74.52 mm below the bifurcation of the sciatic nerve.
The medial cutaneous nerve of the leg derived from the tibial nerve in 93.3% (28 specimens) and was absent in 6.6% (two specimens). The origin of the medial cutaneous nerve was an average of 76.47 ± 67.42 mm below the bifurcation of the sciatic nerve.
An accessory communicating branch existed between the medial and lateral cutaneous nerves in 6.7% (two specimens).
Figure 8.10 Landmarks to locate the sural nerve. Longitudinal arrow drawn along the fibular crest: the tip of the arrow is at tip of the lateral malleolus; curved black line represents the sural nerve; A, 10 cm proximal to tip of lateral malleolus; B, 5 cm proximal to tip of lateral malleolus; C, immediately posterior to tip of lateral malleolus; D, distance directly inferior to the tip of lateral malleolus, in line with the fibular crest; >, represents base of M5; E, at level of base of M5. (From Eastwood DM, Irgau I, Atkins RM. The distal course of the sural nerve and its significance for incisions around the lateral hindfoot. Foot Ankle. 1992;13(4):Figure 1.)
TABLE 8.3 95% CONFIDENCE LIMITS FOR THE ANTERIOR AND POSTERIOR EXTENTS OF THE MAIN NERVE TRUNK DEFINED BY THE MEAN ±1.96 SD AT EACH OF POINTS A-E
Point
Anterior (cm)
Posterior (cm)
A
1.7
3.2
B
1.5
2.7
D
0.6
2.2
C
0.7
3.9
E
2.1
0.5
From Eastwood DM, Irgau I, Atkins R. The distal course of the sural nerve and its significance for incisions around the lateral hindfoot. Foot Ankle. 1992;13(4):200, Table 2.
Figure 8.11 Sural nerve. Three lateral calcaneal branches (small arrow), anastomotic branch (large arrow). Division into dorsomedial and dorsolateral branches of M5 (distal arrow). (From Lawrence SJ, Botte MJ. The sural nerve in the foot and ankle—an anatomic study with clinical and surgical implications. Foot Ankle Int. 1994;15(9):Figure 2.)
Figure 8.12 Sural nerve. Two lateral calcaneal branches (small arrows), a lateral malleolar branch (large arrow), proximal bifurcation (distal arrow). (From Lawrence SJ, Botte MJ. The sural nerve in the foot and ankle—an anatomic study with clinical and surgical implications. Foot Ankle Int. 1994;15(9):Figure 3.)
Figure 8.13 Sural nerve. Four lateral calcaneal branches (small arrows), an anastomotic branch (large arrow), distal bifurcation (distal arrow). (From Lawrence SJ, Botte MJ. The sural nerve in the foot and ankle—an anatomic study with clinical and surgical implications. Foot Ankle Int. 1994;15(9):Figure 4.)
Figure 8.14 Sural nerve(sn),medial cutaneous nerve(mcn),lateral cutaneous nerve(Icn). (From Aktan Ikiz ZA, Ucerler H, Bilge O. The anatomic features of the sural nerve with emphasis on its clinical importance. Foot Ankle Int. 2005;7:Figure 1.)
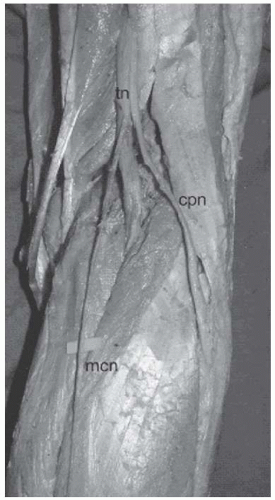
Figure 8.15 Sural nerve. Absence of lateral cutaneous nerve: medial cutaneous nerve(mcn),common peroneal nerve(cpn). (From Aktan Ikiz ZA, Ucerler H, Bilge O. The anatomic features of the sural nerve with emphasis on its clinical importance. Foot Ankle Int. 2005;7:Figure 2.)
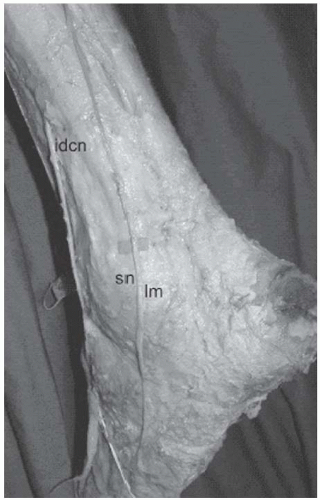
Figure 8.16 Sural nerve passing over the lateral malleolus: sural nerve(sn),intermediate dorsal cutaneous nerve(idcn),lateral malleolus(Im). (From Aktan Ikiz ZA, Ucerler H, Bilge O. The anatomic features of the sural nerve with emphasis on its clinical importance. Foot Ankle Int. 2005;7:Figure 11.)
The formation and course of the sural nerve was classified into five types:
Type 1: The sural nerve was formed by communication of the medial cutaneous nerve originating from the tibial nerve and the lateral cutaneous nerve originating from the common peroneal nerve in 60% (18 specimens).
Type 2: The lateral cutaneous nerve was absent in 16.7% (five cases) and the medial cutaneous nerve reproduced the normal course of the sural nerve.
Type 3: The medial cutaneous nerve became superficial and communicated with the lateral cutaneous nerve in the distal third of the leg in 10% (three specimens).
Type 4: The lateral cutaneous nerve and the medial cutaneous nerve passed down separately and did not form the sural nerve in 6.7% (two specimens).
Type 5: The medial cutaneous nerve was absent in 6.7% (two specimens). The lateral cutaneous nerve divided into three branches and the middle branch followed the standard course of the SN.
The median distance between the most prominent posterior aspect of the lateral malleolus and the sural nerve in all specimens was 12.76 ± 8.79 mm. The mean distance between the tip of the lateral malleolus and the sural nerve was 13.25 ± 6.88 mm. In 13.3% (four specimens) the sural nerve was in contact with the tip of the lateral malleolus and in 10% (three cases) the sural nerve passed over the lateral malleolus (Fig. 8.16).
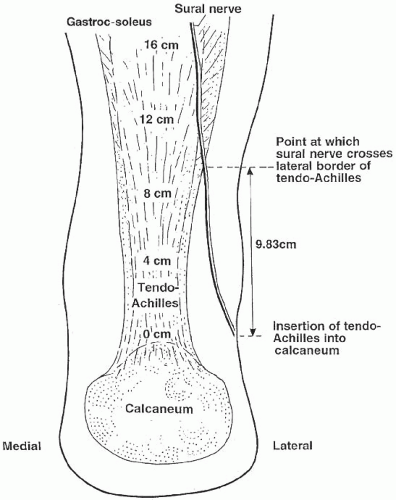
Webb et al.,7 based on the dissection of 30 preserved cadaveric lower limbs, analyzed and described the course of the sural nerve in relation to the Achilles tendon. The widths of Achilles tendon and horizontal distances of the sural nerve to the Achilles tendon lateral border were measured at 0, 4, 8, 12, and 16 cm from the Achilles tendon insertion into the calcaneum. The findings are presented in Table 8.4. At the level of insertion of the Achilles tendon into the calcaneum, the sural nerve was 17.5 mm lateral to the lateral border of the Achilles tendon and this is reduced to 7 mm lateral at 4 cm proximally. The sural nerve curves medially as it courses proximally and crosses the lateral border of the Achilles tendon 9.83 cm (6.55-16 cm) from the calcaneal insertion (Fig. 8.17).
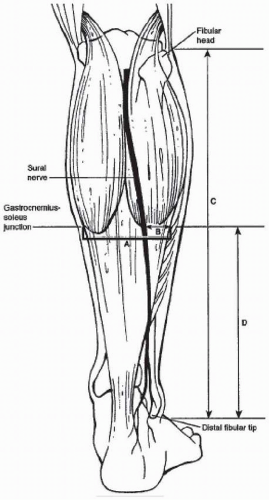
Tashjian et al.,8 based on the dissection of 14 fresh frozen cadaver legs, investigated the distance from the distal tip of the fibula to the gastrocnemius-soleus juncture and then the distance of the sural nerve from the lateral border of the tendon at that level (Fig. 8.18).
TABLE 8.4 WIDTHS OF TA AND DISTANCES OF NERVE FROM MUSCLE/TENDON
Distance from TA Insertion (cm)
TA Width (mm)
Horizontal Distance of Sural Nerve from TA Lateral Border (mm)
0
18.7 (11 to 28)
17.5 (3 to 40)
4
12.7 (8 to 16)
7.00 (3 to 14)
8
16.2 (13 to 31)
2.3 (-4 to 13)
12
28.2 (20 to 44)
-3.3 (0 to-16)
16
38.2 (25 to 58)
-10.4 (0 to-24)
From Webb J, Moorjani N, Radfort M. Anatomy of the sural nerve and its relation to the Achilles tendon. Foot Ankle Int. 2000;21(6):475-477.
Figure 8.17 Posterior view of the Achilles tendon and sural nerve. (From Webb J, Moorjani N, Radfort M. Anatomy of the sural nerve and its relation to the Achilles tendon. Foot Ankle Int. 2000;21 (6): Figure 1.)
Figure 8.18 Posterior aspect of leg with gastrocnemius-soleus complex and sural nerve. (A) Width of gastrocnemius-soleus complex at the level of the musculotendinous junction. (B) Distance between the sural nerve and the lateral border of the gastrocnemius-soleus complex. (C) Length of fibula. (D) Distance from the distal fibula tip to the level of the musculotendinous junction. (From Tashjian RZ, Appel AJ, Banerjee R, et al. Anatomic study of the gastrocnemius-soleus junction and its relationship to the sural nerve. Foot Ankle Int. 2003;6:Figure 1.)
The ratio of the distance of the gastrocnemius-soleus junction from the distal tip of the fibula divided by the length of the fibula was 0.5 (range, 0.5-0.6). The average width of the gastrocnemius-soleus complex at the junction was 58 mm (range, 44-69 mm) and the average distance of the sural nerve from the lateral border of the gastrocnemius-soleus complex at the level of the junction was 12 mm (range, 7-17 mm).
SUPERFICIAL PERONEAL NERVE
The superficial peroneal nerve (musculocutaneous nerve), a branch of the common peroneal nerve, after coursing in the anterolateral compartment of the leg, pierces the deep fascia cruris in the lower third of the leg and divides into the medial and the intermediate dorsal cutaneous nerves of the dorsum of the foot (Fig. 8.19). The piercing of the deep fascia of the leg by the superficial peroneal nerve occurs at different levels. In 100 legs, it occurred 12.5 cm above the tip of the lateral malleolus in 90%; 15 cm above the tip in 1%; 10 cm above the tip in 2%; 7.5 cm above the tip in 5%; and 5 cm above the tip in 2%.1 In 118 legs, it occurred 10.5 cm above the tip of the lateral malleolus in 74.7% and at a higher level in 23.4%.2
When the division of the superficial peroneal nerve into its cutaneous branches occurs at a higher level, the medial dorsal cutaneous branch pierces the fascia cruris at 12.7 cm and the intermediate dorsal cutaneous branch at 4.7 cm above the tip of the lateral malleolus.2 After becoming subcutaneous, the cutaneous common trunk of the superficial peroneal nerve divides into its terminal branches, usually 6.4 cm above the lateral malleolus; this division occurs below this level in 3% and above the same level in 5% (12.5 cm).1 Cutaneous branches are provided by the common trunk, and the largest of these, the lateral malleolar branch, may anastomose with the lateral sural nerve or with an accessory branch of the sural nerve.9
Figure 8.19 Superficial peroneal nerve (1) dividing into the intermediate dorsal cutaneous nerve (3) and the medial dorsal cutaneous nerve (2). The latter subdivides into the dorsomedial cutaneous nerve of the big toe (4) and the common digital nerve to the second web space (5). The intermediate dorsal nerve (3) supplies the dorsal cutaneous nerve of the third (6) and fourth (7) web spaces.
The most common site of the superficial peroneal nerve is “10.5 cm above the tip of the external malleolus just within the anterior border of the fibula in the groove between the peroneal group of muscles and the extensor digitorum longus.”1 In this location the nerve is subcutaneous in 91% and deep to the fascia in 9%.1
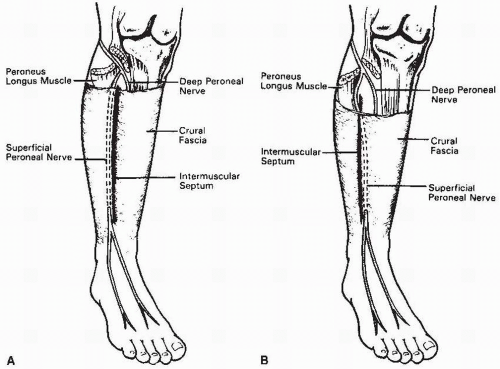
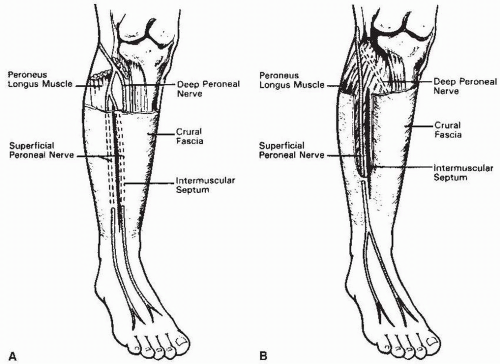
Adkinson and colleagues studied the anatomic variations in the course of the superficial peroneal nerve in 85 legs, with particular attention to the relationship between the nerve and the intemuscular septum between the lateral and anterior compartments of the leg.10 In 73%, the superficial peroneal nerve was located in the lateral compartment and pierced the deep crural fascia an average of 13 cm (range, 3 to 18 cm) proximal to the lateral malleolus (Fig. 8.20). It divided into its terminal branches within 2 cm of its exit point.
In 14%, the superficial peroneal nerve passed into the anterior compartment of the leg and, in 13%, it pierced the crural fascia at 8 to 14 cm proximal to the lateral malleolus (Fig. 8.20). Within 1 to 3 cm of the exit site, the nerve divided into the terminal branches. In one specimen, the nerve divided in the lateral compartment and the two branches pierced the anterolateral intermuscular septum, passed into the anterior compartment, and surfaced through the crural fascia at 13 cm proximal to the lateral malleolus.
In 12%, the superficial peroneal nerve had branches in both the anterior and lateral compartments (Fig. 8.21). The anterior branch pierced the crural fascia at 10 to 17 cm from the lateral malleolus and the lateral branch at 4 to 10 cm. In one leg, the superficial peroneal nerve, located in the lateral compartment, coursed on the superficial surface of the peroneus longus muscle and passed through the crural fascia at 11 cm proximal to the lateral malleolus (see Fig. 8.21).
The intermediate dorsal cutaneous nerve (middle dorsal cutaneous nerve, external branch of the musculocutaneous nerve) is thinner than the medial branch and crosses the fifth and fourth extensor digitorum longus tendons obliquely and superficially. It courses over the third intermetatarsal space. At the anterior aspect of this space, the nerve provides the dorsolateral branch to the third toe and the dorsomedial branch to the fourth toe; it may also send an anastomotic branch to the sural nerve.
The medial dorsal cutaneous nerve is the largest bifurcation branch of the superficial peroneal nerve. It is directed medially toward the inner border of the foot. It crosses the inferior extensor retinaculum and takes a direction nearly parallel to the extensor hallucis longus tendon. The nerve divides into three branches: lateral, middle, and medial. The lateral branch takes off at the inferior border of the inferior extensor retinaculum, crosses the long extensor tendon of the second toe, and—in the anterior aspect of the second intermetatarsal space—divides into the dorsolateral branch of the second toe and the dorsomedial branch of the third toe. The middle branch courses in the interval corresponding to the first intermetatarsal space and, on the anterior aspect of the latter, divides into the dorsomedial branch of the second toe and the dorsolateral branch of the big toe. These two branches are very thin and receive reinforcement from the branches of the deep peroneal nerve. The medial branch is directed medially, crosses the extensor hallucis longus tendon superficially and obliquely, and then runs parallel to the tendon, forming the dorsomedial cutaneous nerve of the big toe. This nerve branch is subcutaneous but is located within or immediately under the superficial fascia of the foot and yet is superficial to the extensor hallucis longus tendon and its investing fascia. The medial cutaneous branch anastomoses at the level of the metatarsophalangeal joint of the big toe with a terminal branch of the saphenous nerve.
Figure 8.20 (A) In 73% the superficial peroneal nerve lies only in the lateral muscle compartment until, as it courses inferiorly, it pierces the crural fascia 3 to 18 cm proximal to the lateral malleolus. (B) In 14% the superficial peroneal nerve passes through the crural fascia from the anterior muscle compartment. (Adkinson DP, Bossem J, Gaccione DR, et al. Anatomical variations in the course of the superficial peroneal nerve. J Bone Joint Surg Am. 1991;73 [1]:112.)
Figure 8.21 (A) In 12% the superficial nerve has branches in both the anterior and lateral compartments. (B) In 1% the superficial peroneal nerve arises from the common peroneal nerve 1 cm from the posterior aspect of the fibular neck and never lies deep to the peroneus longus muscle. The nerve descends instead on the superficial surface of the peroneus longus muscle and pierces the crural fascia 11 cm proximal to the lateral malleolus. It then immediately divides into medial and intermediate dorsal cutaneous nerves of the foot. (Adkinson DP, Bosse MJ, Gaccione DR, et al. Anatomical variations in the course of the superficial peroneal nerve. J Bone Joint Surg Am. 1991;73 [1]:112.)
The accessory deep peroneal nerve, a branch of the superficial peroneal nerve, was first recognized by Bryce and described in three cases.11, 12, 13 The thin branch passed through the substance of the peroneus brevis muscle and terminated once in the ligament of the ankle joint and twice in the extensor digitorum brevis.
A comprehensive study of the same nerve is provided by Winckler, who described it in seven cases (five adults and two newborns).14 The branch of the superficial peroneal nerve to the peroneus brevis muscle, after providing the motor branches to the latter, courses along the posterior border of the peroneus brevis tendon, remains in the compartment of the peronei, and reaches the posterior aspect of the lateral malleolus. At this level the nerve provides branches to the posterior talofibular ligament and to the calcaneofibular ligament and then turns around the lateral malleolus parallel to the tendon of the peroneus brevis, reaches the extensor digitorum brevis and innervates its two lateral heads (to the fourth and third toes), and terminates in the dorsal capsule of the calcaneocuboid joint. Prior to entering the extensor digitorum brevis, the accessory deep peroneal nerve provides branches to the anterior talofibular ligament and to the capsule of the ankle joint.
As described by Winckler, the accessory deep peroneal nerve is associated with a strong development of the peroneus brevis muscle and with the presence of an accessory tendon extending from the peroneus brevis muscle to the fifth toe as the peroneal extensor of the fifth toe.14 The nerve may be purely sensory, innervating the ankle joint or certain articulations of the tarsal and tarsometatarsal joints; however, it is usually mixed, and it is never pure motor, innervating only the extensor digitorum brevis.
Lambert, in an electromyographic investigation of 50 healthy persons, found evidence of the presence of this accessory deep peroneal nerve in 22% of the examined limbs.15
DEEP PERONEAL NERVE
The deep peroneal nerve, after piercing the extensor digitorum longus muscle, joins the anterior tibial artery. In the upper third of the leg the nerve is situated between the extensor digitorum longus and the tibialis anterior muscle. In the middle third the nerve is located between the extensor hallucis longus and the tibialis anterior muscle. In the distal third of the leg the deep peroneal nerve passes behind the obliquely directed extensor hallucis longus muscle-tendon, and at 2.5 to 5 cm above the ankle the nerve is located between the latter tendon and the extensor digitorum longus tendon.1
The deep peroneal nerve is lateral to the anterior tibial artery proximally and distally, but some variations are possible. Horwitz, in a study of 100 legs, mentions that in 90% of the cases the nerve is lateral to the artery in the upper and middle thirds of the leg and then at 10 cm above the ankle joint the nerve is anterolateral to the artery; at 5 cm above the joint the nerve is again lateral to the artery.1 In 4% the nerve is lateral initially, crosses the artery posteriorly, and is medial farther down.1 In 1% the nerve is lateral initially, crosses the artery anteriorly, and is medial to the latter distally.1
The deep peroneal nerve divides into a medial and a lateral terminal branch at 1.3 cm above the ankle joint in 98% of the cases (Fig. 8.22).1 In 2% the branching occurs at 6.4 cm above the ankle joint or at the level of the ankle joint.1 At the level of the ankle the deep peroneal nerve is located under the reflected segment of the extensor pulley of the extensor hallucis longus tendon.
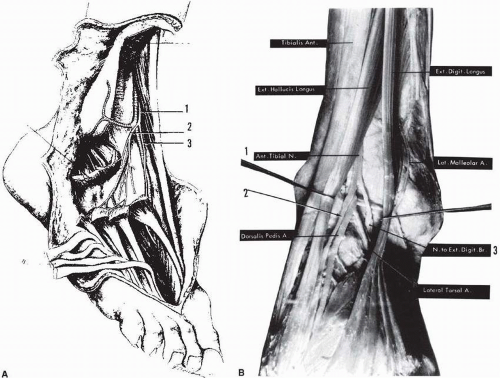
Figure 8.22 (A) The deep peroneal nerve (1) divides into lateral (2) and medial (3) branches at the level of the ankle joint. The lateral branch (2) supplies the extensor digitorum brevis muscle from the deep surface. It also provides articular branches. The medial division branch (3) courses under the extensor digitorum brevis of the hallux and reaches the dorsum of the first web space (the nerve has been sectioned at that level). (Hovelacque A. Anatomie des Nerfs Craniens et Rachidiens et du Systeme Grand Sympathique. Paris: Doin; 1927:612.) (B) The deep peroneal nerve (1) (or anterior tibial nerve) divides into a medial branch (2), which will reach the first web space and the lateral branch (3) or nerve to the extensor digiti brevis. (Cosentino R. Atlas of Anatomy and Surgical Approaches in Orthopedic Surgery, Vol II. The Lower Extremity. Springfield, IL: Charles C Thomas; 1960: Figure 96.)
The medial branch usually is located medial to the dorsalis pedis artery. It is the larger branch and continues in the direction of the nerve. Initially it is located between the extensor hallucis longus tendon and the medial border of the extensor hallucis brevis muscle. It is crossed superficially and obliquely by the latter and reaches the first intermetatarsal space, where it pierces the deep dorsal aponeurosis of the foot. It is now located between the extensor hallucis brevis tendon medially and the long extensor of the second toe laterally. The nerve divides into two branches and supplies the dorsolateral cutaneous branch to the big toe and the dorsomedial cutaneous branch to the second toe (Fig. 8.23). Quite often the deep peroneal nerve joins the branches of the superficial peroneal nerve in going to the first web space.
The lateral branch of the deep peroneal nerve is directed anterolaterally, penetrates and innervates the extensor digitorum brevis muscle, and terminates into very thin branches that are applied against the tarsal skeleton and form the second, third, and fourth dorsal interosseous nerves. These branches provide the nerve supply to the tarsometatarsal, the metatarso-phalangeal, and interphalangeal joints of the lesser toes.
The average diameter of the deep peroneal nerve is 1 to 3 mm, and the most constant site is 2.5 cm above the level of the ankle joint anteriorly, under the upper arm of the inferior extensor retinaculum between the extensor hallucis longus medially and the extensor digitorum longus laterally.1
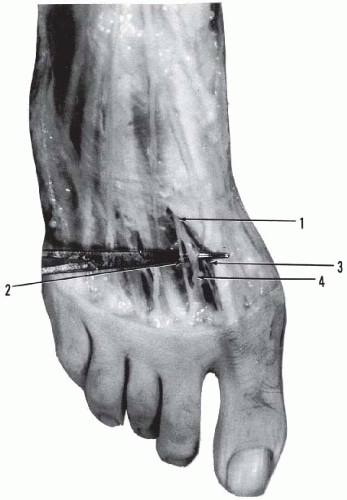
Figure 8.23 Neurovascular bundle of the first web space. Deep peroneal nerve (1) dividing into dorsomedial nerve (2) of the second toe and dorsolateral nerve (3) of the big toe; first dorsal metatarsal artery (4).
The dorsal cutaneous nerve supply to the dorsum of the foot is very variable. Statistical information based on a collective study of 229 feet reported by the Anatomical Society of Great Britain and Ireland16 is presented in Figures 8.24, 8.25, 8.26, 8.27. When the territory of the sural nerve increases, that of the intermediate dorsal cutaneous branch decreases, and vice versa. In the same series, only in one case did the saphenous nerve supply the inner side of the big toe, and in another one it reached the inner side of the head of the first metatarsal bone.16
Clarification is required at this time in regard to the data provided by this collective study as a misinformation has been initiated recently and is developing rapidly. In early October 1890, five questions were issued by the Committee of Collective Investigation of the Anatomical Society of Great Britain and Ireland. The fourth question concerned the distribution of the cutaneous nerves on the dorsum of the foot and toe.
At the Second Annual Report of this Committee for the year 1890-1891, the report was given by Arthur Thomson Lecturer on anatomy. Fifteen anatomists had participated and the report indicated that “A total of 229 feet have been examined and, in tabulating the results, the graphic method has been adopted in preference to the description. Twelve types are figured and lettered A, B, C, etc in order of their frequency. …” Their results were presented in a table depicting the 12 varieties. In our study, we have presented the 12 types with only improved graphics and due reference was given to the work of the Anatomical Society.
Only gold members can continue reading. Log In or Register to continue