surface occupies the anterosuperior aspect. The base of the triangle is proximal and convex. The apex is anteroinferior, located on the anterior border of the malleolus. The anterior border is inclined backward, whereas the posterior border is directed anteroinferiorly. The surface is convex along its long axis and corresponds to the lateral articular surface of the talus. Behind the posterosuperior angle of the triangular articular surface is the round posterior fibular tubercle, which gives origin to the deep component of the posterior tibiofibular ligament. Below the tubercle and behind the triangular articular surface is the digital fossa. The upper segment of the fossa is cribriform, with multiple vascular foramina. The lower segment gives origin to the posterior talofibular ligament. The superficial components of the posterior tibiofibular ligament originate from the posterior border of the peroneal tubercle and digital fossa (see Fig. 2.2).
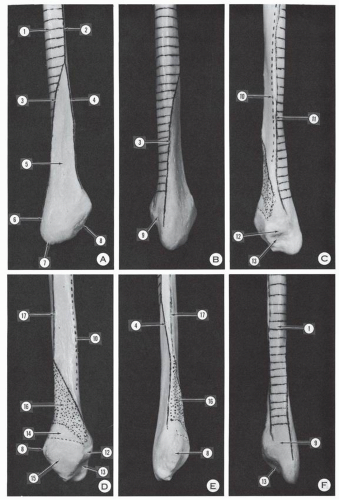 Figure 2.1 Distal fibula and lateral malleolus. (A) Lateral surface. (B) Posterolateral view. (C) Posteromedialview. (D) Medial surface. (E) Anterior surface. (F) Posterior surface. (1, surface of origin of peroneus brevis muscle—this surface becomes posterior distally and continues as posterior surface of lateral malleolus; 2, anterior border of fibular shaft for insertion of anterior peroneal septum; 3, posterior division branch of anterior border [2]—it forms a crest and continues as lateral border of posterior surface of lateral malleolus; 4, anterior division branch of anterior border; 5, subcutaneous surface; 6 posterior border of lateral malleolus; 7, tip of lateral malleolus; 8, anterior border of lateral malleolus; 9, sulcus of peronei tendons; 10, line of insertion of deep transverse fascia of leg; 11, line of insertion of posterior peroneal septum; 12, posterior tubercle of medial surface of lateral malleolus; 13, digital fossa; 14, surface corresponding to peroneotibial recess; 15, articular surface corresponding to lateral surface of talus; 16, insertion of tibiofibular interosseous ligament; 17, insertion line of the interosseous membrane.) The anterior division line (4) of the anterior fibular border and the line of the interosseous membrane (17) join distally. |
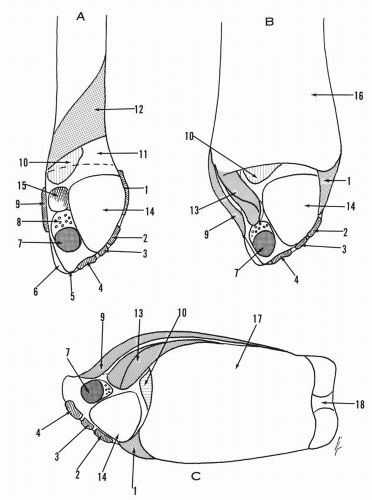 Figure 2.2 (A) Medial surface of distal fibula and lateral malleolus. (B) Same view as in (A). Distal tibia connected to fibula. (C) Inferior view of the distal tibiofibular complex. (1, anterior tibiofibular ligament; 2,main component of anterior talofibular ligament; 3, secondary band of anterior talofibular ligament; 4, calcaneofibular ligament; 5, tip of lateral malleolus, free of insertion; 6, gliding surface of peronei tendons; 7, posterior talofibular ligament; 8, cribriform fossa; 9, superficial component of posterior tibiofibular ligament; 10,synovial fringe; 11, peroneal surface corresponding to tibioperoneal recess; 12, insertion of tibiofibular interosseous ligament; 13, deep component of posterior tibiofibular ligament; 14, articular surface for the lateral surface of the talus; 15, posterosuperior tuberosity; 16, tibia; 17, tibia plafond; 18, medial malleolus.) |
of the sulcus is given as the narrowest, 5 mm; the majority (62%), 6 to 7 mm; and the widest, 10 mm. The lateral border of the posterior surface may become prominent and form a lateral bony ridge. “It helps to form a flange against which the tendons of the peroneal muscles play, and it gives attachment to some of the fibers of the superior peroneal retinaculum.1 The occurrence of this lateral bony ridge, based on Edwards’ data, is as follows: well-developed lateral bony ridge, 22%; slightly developed lateral bony ridge, 48% absence of a developed lateral bony ridge, 30%.-1 The majority of the ridges are 2 mm high, but occasionally the ridges may reach an elevation of 4 mm. Cartilage covering may increase the ridge 1 to 2 mm, and often the ridge is formed by cartilage only1
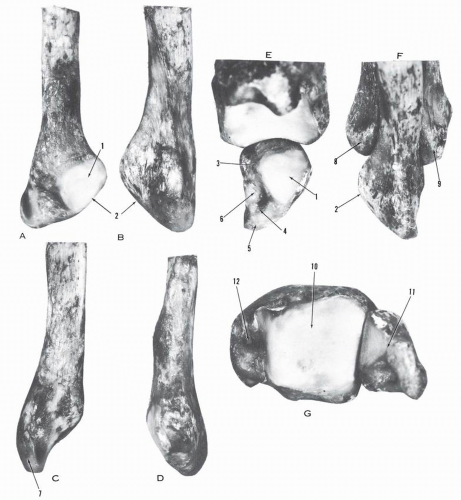 Figure 2.3 (A) Medial view of left fibula. (B) Lateral view of fibula. (C) Posterior view of fibula. (D) Anterior view of fibula. (E) Medial view of tibia-lateral malleolus. (F) Lateral view of distal fibula-tibia. (G) Inferior view of distal tibia-fibula. 1, articular surface; 2, anterior border; 3, posterosuperior tubercle; 4, insertion tubercle of posterior talofibular ligament; 5, tip of lateral malleolus; 6, digital fossa; 7, gliding surface for peronei tendon; 8, anterior tibial tubercle; 9, posterior tibial tubercle; 10, tibial plafond; 11, lateral malleolus; 12, medial malleolus.) |
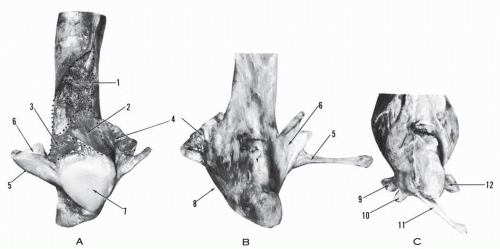 Figure 2.4 (A) Medial view of left distal fibula and lateral malleolus. (B,C) Lateral view of lateral malleolus. (1, insertion of tibiofibular interosseous ligament; 2, fibular component of tibiofibular recess; 3, insertion of synovial fringe; 4, anterior tibiofibular ligament; 5, 6, posterior tibiofibular ligament; 7, articular surface; 8, anterior border; 9, main component of anterior talofibular ligament; 10, secondary component of anterior talofibular ligament; 11, calcaneofibular ligament; 12, posterior talofibular ligament.) |
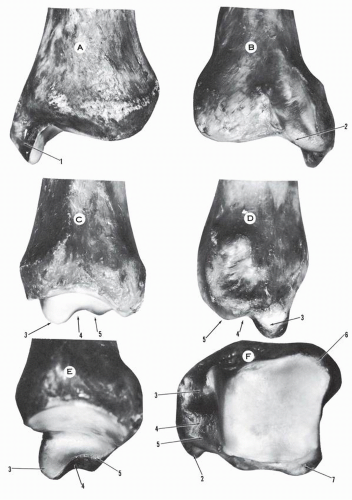 Figure 2.5 (A) Anterior aspect of left distal tibia. (B) Posterior aspect of distal tibia. (C) Lateral aspect of distal tibia. (D) Medial aspect of distal tibia and medial malleolus. (E) Lateral aspect of medial malleolus. (F) Inferior view of distal tibia. (1, medial malleolus; 2, sulcus for tibialis posterior tendon; 3, anterior colliculus; 4, intercollicular groove; 5, posterior colliculus; 6, anterior tibial tubercle; 7, posterior tibial tubercle.) |
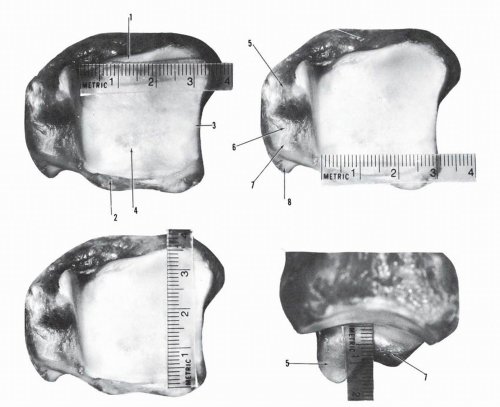 Figure 2.6 Distal tibia and medial malleolus. The anterior border of the distal tibia is longer than the posterior border, and the lateral border of the distal tibia is longer than the medial border. The anterior colliculus of the medial malleolus is 0.5 cm longer than the posterior colliculus. (1, anterior border of distal tibia; 2, posterior border of distal tibia; 3, lateral border of distal tibia—incisura tibialis; 4, tibial plafond; 5, anterior colliculus of medial malleolus; 6, intercollicular groove of medial malleolus; 7, posterior colliculus of medial malleolus; 8, groove for tibialis posterior tendon.) |
is an intra-articular segment. This surface may bear a small articular surface (squatting facet), usually lateral in location and very occasionally medial and lateral. The distribution of these facets is as shown in Table 2.1.
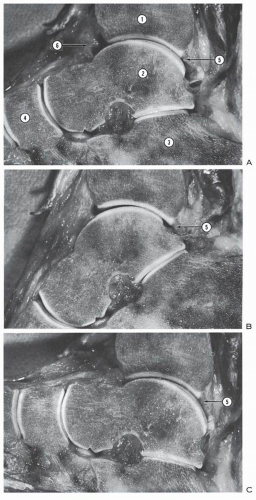 Figure 2.7 Sagittal cross-section of the ankle. (A) Ankle in neutral. (B) Ankle in plantar flexion. (C) Ankle in dorsiflexion. In any position, the articular surface of the distal tibia covers only twothirds of the corresponding talar articular surface. (1, tibia; 2, talus; 3, calcaneus; 4, navicular; 5, deep component of tibiofibular ligament forming a labrum; 6, anterior adipose body with large anterior joint cavity.) |
TABLE 2.1 DISTRIBUTION OF SQUATTING FACETS | ||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||
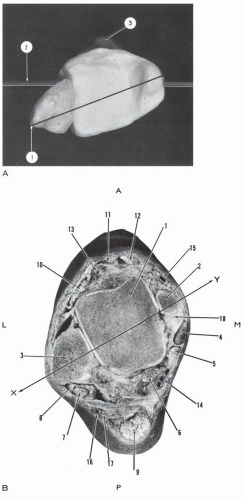 Figure 2.8 (A) Distal tibia-fibula, right ankle, inferior view. (1, bimalleolar axis; 2, transverse axis, transtibial plateau; 3, anterior tibial tubercle.) The bimalleolar axis is oriented posterolaterally. The lateral malleolus is posterior, and the medial malleolus is anterior. (B) Cross-section of left ankle, lower surface, passing 1 cm above the tip of the medial malleolus. (A, anterior; P, posterior; L, lateral; M, medial; 1, talus; 2, anterior colliculus of medial malleolus; 3, lateral malleolus; 4,tibialis posterior tendon and tunnel; 5, flexor digitorum longus tendon and tunnel; 6, flexor hallucis longus tendon-muscle; 7, peroneus longus tendon; 8, peroneus brevis, inverted U-shaped tendon; 9, Achilles tendon; 10, extensor digitorum longus tendon; 11, extensor hallucis longus tendon; 12, tibialis anterior tendon; 13, dorsalis pedis artery and veins; 14, posterior tibial neurovascular bundle; 15, greater saphenous vein; 16, lesser saphenous vein; 17, sural nerve; 18, deltoid ligament, deep talotibial component [note relationship of tibialis posterior tendon and deltoid ligament]; X-Y, bimalleolar axis oriented posterolaterally.) |
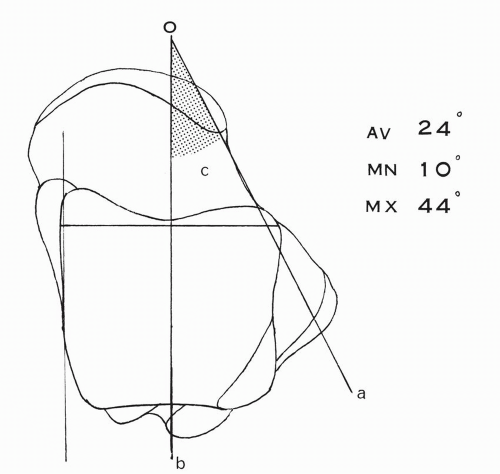 Figure 2.9 Declination angle (c) of the talar neck relative to the body, (a) Long axis of neck, (b) Long axis of body. |
TABLE 2.2 ANGLES OF DECLINATION AND INCLINATION IN TALUS | ||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||
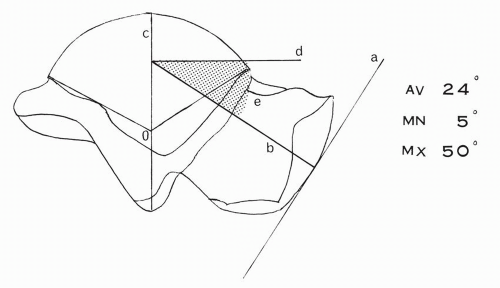 Figure 2.10 Inclination angle (e) of the talar neck relative to the body. The center O of the lateral trochlear arc is determined. The arc is bisected by the radius OC. A tangent is drawn at the apex of the navicular articular surface. A perpendicular line b is drawn at the tangential point. The line b gives the direction of the talar neck and intersects the radius OC of the talar trochlear arc. At this point of intersection, a perpendicular line d is traced, determining the inclination angle e. |
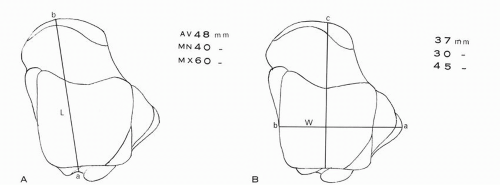 Figure 2.11 Measurements of talus. (A) Length of talus is (L) determined by a line joining the apex of the navicular articular surface to the flexor hallucis longus groove. (B) Width of talus (W) determined with caliper holding the talus at the tip of the lateral process and the middle of the medial trochlear line. The direction of the caliper is maintained perpendicular to the latter. |
apical portion. Rarely, a concavity replaces the convexity in this location. The vertical concavity is determined by the outward projection of the lateral talar process. The angle of projection as measured in 100 tali is 32 degrees average, 55 degrees maximum, and 15 degrees minimum (Fig. 2.14).
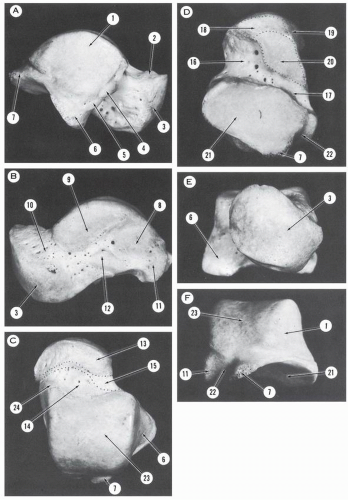 Figure 2.12 Talus. (A) Lateral aspect. (B) Medial aspect. (C) Superior aspect. (D) Inferior aspect. (E) Anterior aspect. (F) Posterior aspect. (1, articular surface—facies malleolus lateralis; 2, cervical collar; 3, articular surface—facies articularis navicularis; 4, 5, tubercles for insertions of anterior talofibular ligaments; 6, lateral process; 7, posterolateral tubercle; 8, oval surface for insertion of talotibial component of deltoid ligament; 9, articular surface—facies malleolaris medialis; 10, talar neck; 11, posteromedial tubercle; 12, tubercle of insertion of deltoid ligament; 13, segment of talar neck located within talonavicular joint; 14, segment of talar neck located within talotibial joint; 15, extra-articular segment of talar neck where a bursa may be found against which glides medial root of inferior extensor retinaculum; 16, sinus tarsi; 17, canalis tarsi; 18, anterior calcaneal articular surface of the talar head; 19, articular segment of talar head corresponding to superomedial and inferior calcaneonavicular ligaments; 20, middle calcaneal articular surface of talar neck; 21, posterior calcaneal articular surface of the talar body; 22, canal of the flexor hallucis longus tendon; 23, trochlear surface; 24, anteromedial extension of trochlear. |
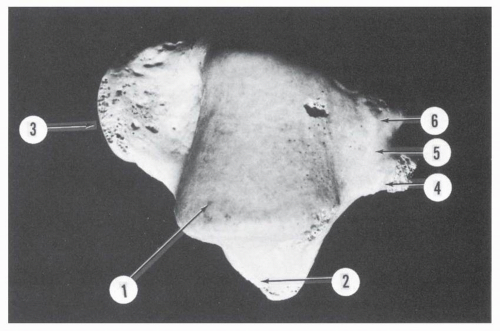 Figure 2.13 Superior aspect of talus. (1, talar pulley; 2, lateral process; 3, talar head; 4, posterolateral tubercle; 5, canal of flexor hallucis longus; 6, posteromedial tubercle.) |
TABLE 2.3 DIFFERENCE IN ANTERIOR AND POSTERIOR TRANSVERSE DIAMETERS | ||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||
TABLE 2.4 FREQUENCY OF OCCURRENCE OF MEDIAL EXTENSION FACET | ||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||
anteroposteriorly. The anterior third of this curve is part of a circle with a radius smaller than that of the lateral surface. The posterior two-thirds is an arc of a circle, the radius of which is larger than that of the lateral profile.6 Inman, contouring the trochlear surface in planes perpendicular to the functional axis of the ankle, found the medial side of the trochlea to be an arc of a circle in 80% of the tali and to deviate from it in the remaining 20%.3 The average arc on the medial side is 103 degrees ± 14.3
TABLE 2.5 FREQUENCY OF OCCURRENCE OF LATERAL EXTENSION AND SQUATTING FACETS | ||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||
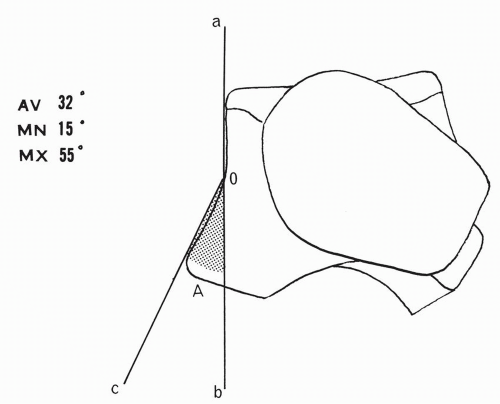 Figure 2.14 Angle of lateral projection (A) of talar lateral process. aob, tangential line to lateral surface; co, tangential line to lateral process. |
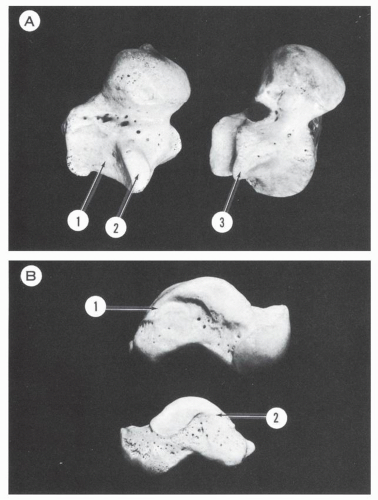 Figure 2.15 (A) Inferolateral view of tali. (1, posterior calcaneal articular surface with 2, facies externa accessoria; 3, absent accessory facet.) (B) Medial view of tali. (1, 2, posterior extension of medial articular facet.) |
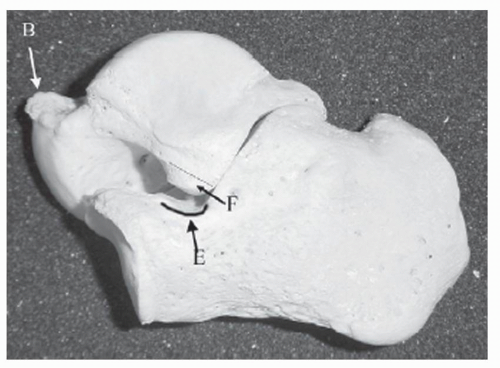 Figure 2.16 Lateral view of the talus and calcaneus, showing an accessory anterolateral talar facet (F), beaking of the dorsal aspect of the talar neck (B), and a calcaneal neck anterior extension facet (E). (From Martus JE, Fermino JE, Caird MS, et al. Accessory anterolateral facet of the pediatric talus. An anatomical study. J Bone Joint Surg Am. 2008;90:2453.) |
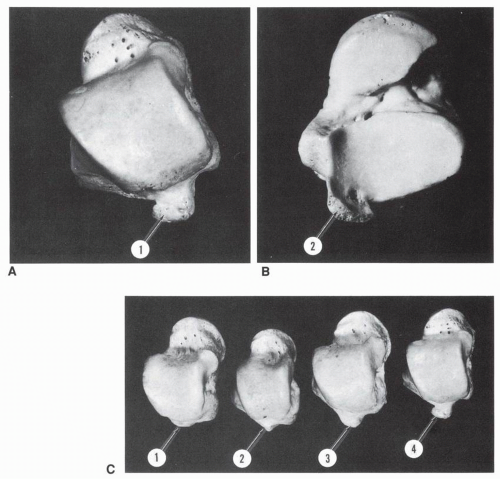 Figure 2.17 (A) Trigonal process, superior view. (B) Trigonal process, inferior view. Its articular surface is in continuity with that of the posterior calcaneal articular surface. (C) Variations in the size of the trigonal process. (1, absent; 2, moderate; 3, medium; 4, large.) |
large and may extend downward over the os calcis, contributing to a talocalcaneal coalition (Fig. 2.20).
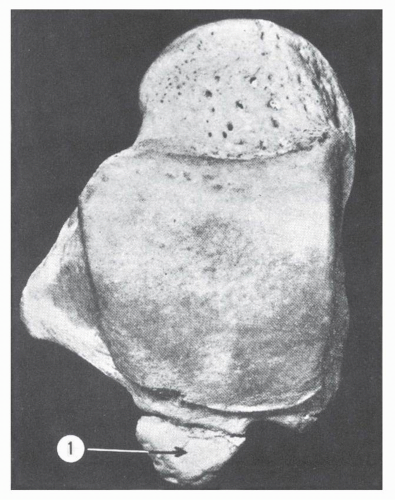 Figure 2.18 Os trigonum (1). (From Dwight T. Variations of the Bones of the Hands and Feet: A Clinical Atlas. Philadelphia: JB Lippincctt; 1907:14-23.) |
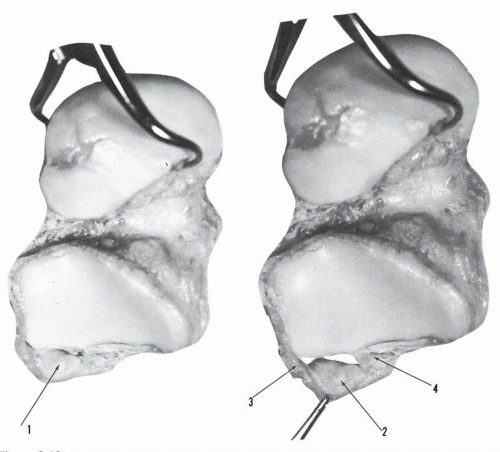 Figure 2.19 Os trigonum. (1, 2, inferior articular surface; 3, 4, ligaments of attachment on each side: thin anterior capsular structure has been removed.) |
TABLE 2.6 FREQUENCY OF OCCURRENCE OF OS TRIGONUM IN ADULTS | ||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||
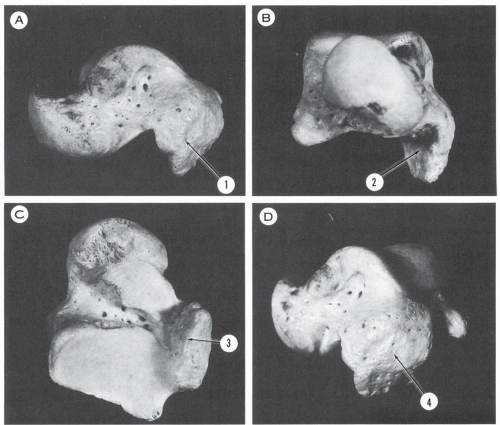 Figure 2.20 Talus. (A) Medial aspect. (B) Anterior aspect. (C) Inferior aspect. (D) Posteromedial aspect. Large posteromedial talar tubercle (1 to 4) probably forming a coalition with its corresponding calcaneus. |
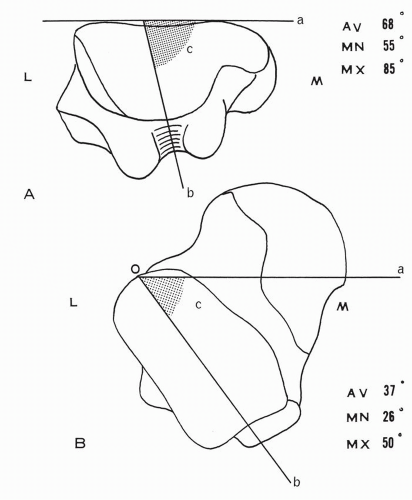 Figure 2.21 Angles of talus. (A) Posterior aspect of talus. Inclination angle (c) of the sulcus for the flexor hallucis longus tendon. (B) Inferior surface of talus. Angle (c) formed by the long axis ob of the posterior calcaneal surface with a line oa parallel to the anterior trochlear border. (L, lateral; M, medial.) |
corresponding to the inferior calcaneonavicular ligament (Figs. 2.22 and 2.24). A ridge may delineate these surfaces. Occasionally, a separation notch is seen between the surfaces; if the notch is deep enough, a near-complete separation occurs between the middle and anterior calcaneal surfaces. In rare instances, a complete separation is present.
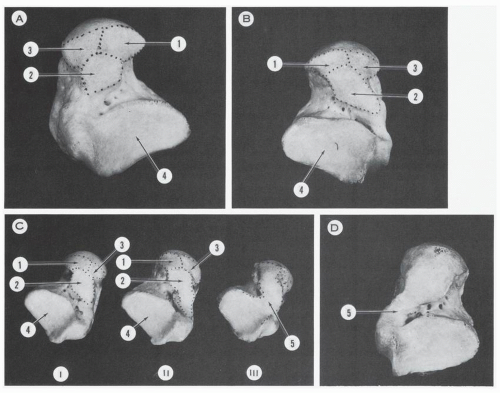 Figure 2.22 Variations in size and contour of the inferior articular surfaces of the talus. (A) Common configuration of the articular surfaces. (B) Posterior extension of the middle calcaneal surface. (C) (I) Moderate posterior extension of middle calcaneal surface. (II) Marked posterior extension of middle calcaneal surface. (III) Fusion (5) of all articular surfaces, obliterating the tarsal canal and a segment of the sinus tarsi. (D) Fusion (5) of the middle and posterior calcaneal surfaces on the medial aspect of the tarsal canal, which is still maintained. (1, anterior calcaneal articular surface of talar head; 2, middle calcaneal articular surface of talar neck; 3, articular segment of talar head corresponding to superomedial and inferior calcaneonavicular ligament; 4, posterior calcaneal articular surface of talar body.) |
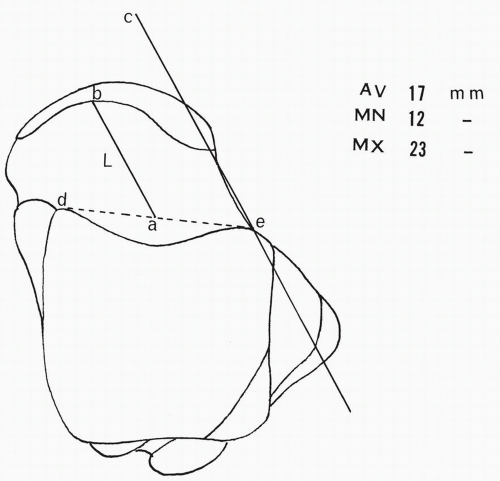 Figure 2.23 Length of talar neck L. An anterior trochlear line de is drawn as indicated. The midpoint a is determined. A line ec is drawn along the talar neck. From the point a a line ab is drawn, parallel to line ec. The segment ab is considered the length of the talar neck, and it terminates where the articular surface is encountered. |
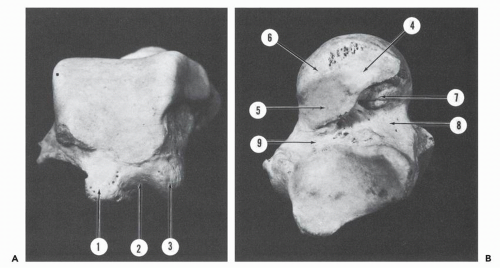 Figure 2.24 (A) Posterior aspect of talus. (B) Inferior aspect of talus. (1, posterolateral tubercle; 2, sulcus for flexor hallucis longus tendon; 3, posteromedial tubercle; 4, anterior calcaneal articular surface; 5, middle calcaneal articular surface; 6, articular segment of head corresponding to superomedial and inferomedial calcaneonavicular ligaments; 7, tubercle for cervical ligament; 8, sinus tarsi; 9, tarsal canal.) |
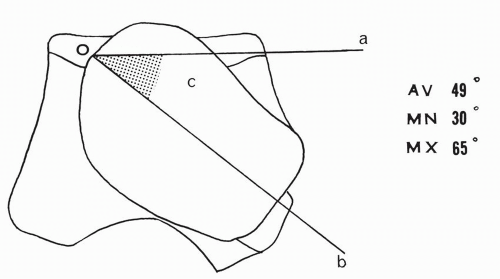 Figure 2.25 Angle (c) of lateral rotation of the talar head,(do, line parallel to trochlear surface; bo, long axis of head) |
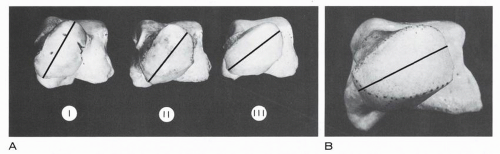 Figure 2.26 Variations in lateral rotation of talar head. (A) (I) Marked rotation. (II) Moderate rotation. (Ill) Minimal rotation. (B) Minimal rotation. |
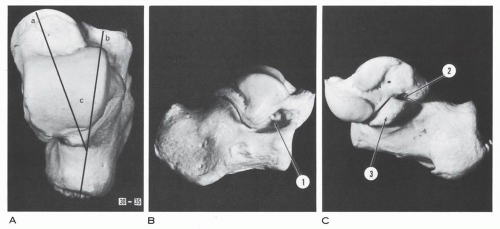 Figure 2.27 Talocalcaneal relationship. (A) Superior view—angle between long axis of calcaneus b and axis of talar neck a, 30 to 35 degrees. (B) Lateral view. (C) Medial view. (1, sinus tarsi; 2, medial opening of tarsal canal between posterior border of sustentaculum tali and anterior border of talar posteromedial tubercle; 3, sustentaculum tali.) |
the width was 53 mm maximum and 26 mm minimum.15 In the present series of 50 calcanei, the length was 75 mm average, 83 mm maximum, and 65 mm minimum; the width was 40 mm average, 46 mm maximum, and 35 mm minimum. The average breadth × 100/length index in the present series is 53 and may range between 50 and 60.15 The height of the os calcis is close to 50% of the length; in 50 calcanei, the average height was 40 mm, maximum 47 mm, and minimum 33.5 mm. The calcaneus is in the form of an irregular rectangle solid and presents six surfaces: superior, inferior, lateral, medial, posterior, and anterior.
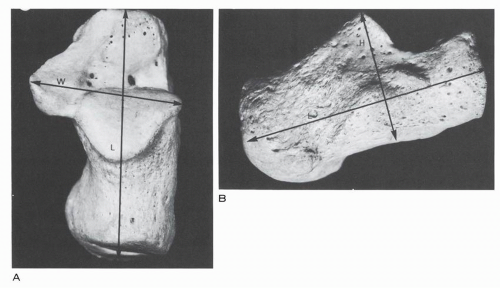 Figure 2.28 Dorsal (A) and lateral (B) views of calcaneus. (H, height; L, length; W, width.) |
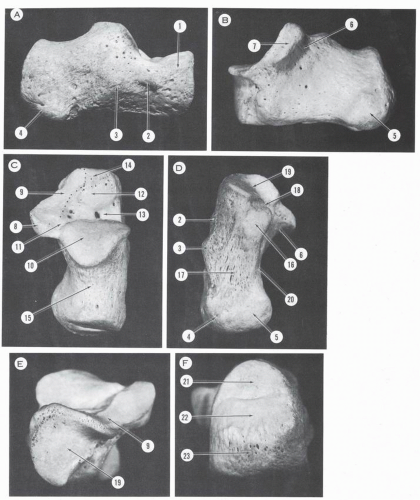 Figure 2.29 Calcaneus. (A) Lateral surface. (B) Medial surface. (C) Superior surface. (D) Inferior surface. (E) Anterior surface. (F) Posterior surface. (1, great apophysis; 2, trochlear process; 3, eminentia retrotrochlearis; 4, lateral tuberosity; 5, medial tuberosity; 6, canal for flexor hallucis longus tendon; 7, medial surface of sustentaculum tali; 8, posterior border of sustentaculum tali; 9, fused anterior and middle talar articular surfaces; 10, posterior talar articular surface; 11, canalis tarsi; 12, sinus tarsi—bony eminence; 13, sinus tarsi—fossa calcanei; 14, sinus tarsi—insertion surface of bifurcate ligament; 15, posterior third of superior surface; 16, anterior tuberosity of inferior surface; 17, longitudinally striated inferior surface; 18, coronoid fossa; 19, cuboidal articular surface; 20, medial calcaneal canal; 21, upper third of posterior surface, corresponding to pre-Achilles bursa; 22, 23, middle and lower thirds of posterior surface, corresponding to insertion of Achilles tendon.) |
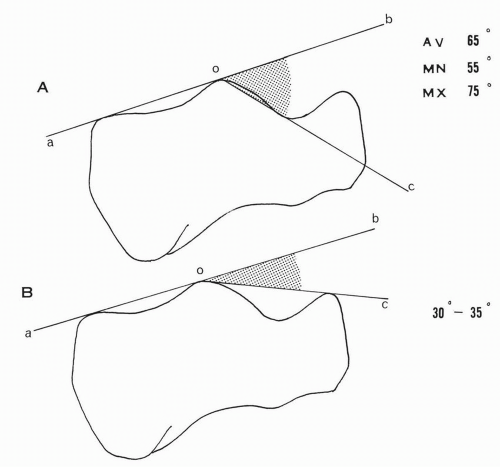 Figure 2.30 (A) Angle of inclination boc of the posterior talar articular surface. (B) Boehler tuberjoint angle boc. |
posterior facets are united into a single surface. The distribution of these variations is shown in Table 2.8 (Fig. 2.31).
TABLE 2.7 FREQUENCY OF OCCURRENCE OF ACCESSORY FACETS | ||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||
TABLE 2.8 FREQUENCY OF OCCURRENCE OF VARIATIONS IN CALCANEI | |||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |||||||||||||||||||||||||||||||||||||||||||||||||
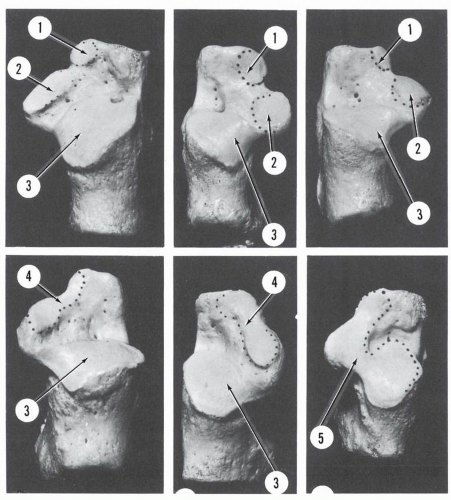 Figure 2.31 Variations of the articular surfaces on the superior aspect of the os calcis. (1, anterior talar articular surface; 2, middle talar articular surface; 3, posterior talar articular surface; 4, fused anterior and middle talar anticular surfaces;5, fused anterior, middle, and posterior talar articular surfaces.) |
articularis talaris anterior. The posteromedial corner of the sinus tarsi continues with the calcaneal or tarsal canal.
peroneal tubercle and occurred in 42.5% (Agra) and 2.42% (Lucknow).
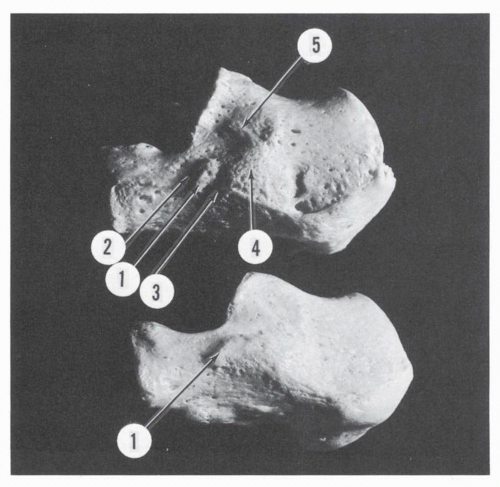 Figure 2.32 Lateral aspect, calcanei. (1, trochlear process; 2, sulcus for peroneus brevis tendon; 3, sulcus for peroneus longus tendon; 4, eminentia retrotrochlearis; 5, tubercle for calcaneofibular ligament.) |
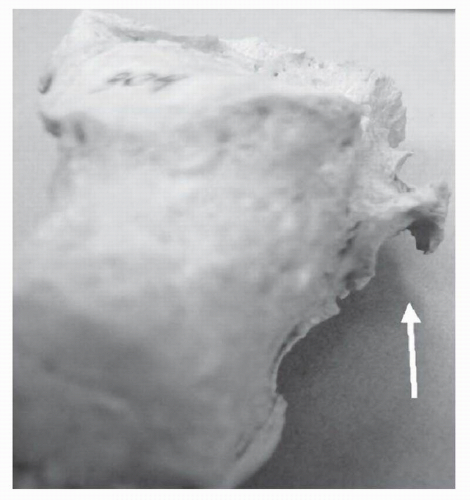 Figure 2.33 Tunnel type peroneal tubercle (arrow). (From Hyer CF, Dawson JM, Philbin TM, et al. The peroneal tubercle: Description, classification, and relevance to peroneus longus tendon pathology. Foot Ankle Inter. 2005;11: Figure 4.) |
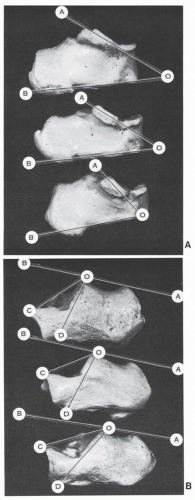 Figure 2.34 (A) Variable inclination of sustentaculum tali—angle AOB. (B) Variations of inclination angle BOD and of tuber-joint angle (Boehler) BOC. (Top, marked inclination; center, moderate inclination; bottom, minimal inclination.) |
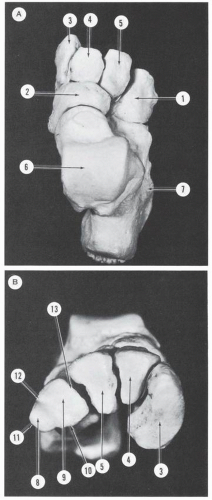 Figure 2.35 (A) Dorsal aspect, tarsus. (B) Transverse arch formed by the cuneiforms and the cuboid, which is also wedgeshaped. (1, cuboid; 2, navicular; 3, medial cuneiform; 4, middle cuneiform; 5, lateral cuneiform; 6, talus; 7, calcaneus. Cuboidal surfaces; 8, 9, lateral and medial aspect of anterior articular surface; 10, inferior border; 11, apex; 12, dorsolateral border; 13, medial border.) |
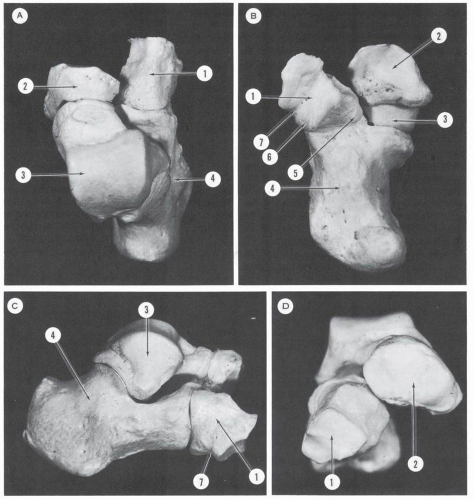 Figure 2.36 Subtalar and midtarsal skeleton. (A) Dorsal aspect. (B) Plantar aspect. (C) Lateral aspect. (D) Anterior aspect. (1, cuboid; 2, navicular; 3, talus; 4, calcaneus [elongated ˜ contour of Chopart joint is seen]; 5, beak of cuboid; 6, sesamoid facet of cuboid; 7, canal of peroneus longus.) |
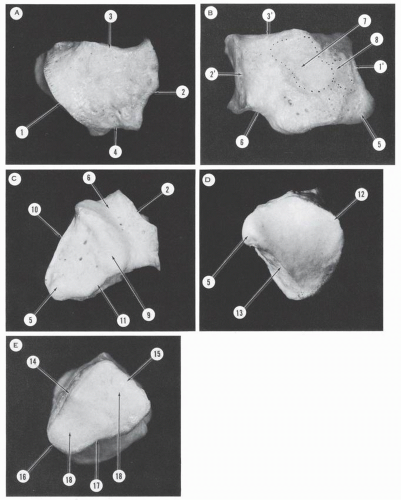 Figure 2.37 Cuboid, right. (A) Dorsal surface. (B) Medial surface. (C) Inferior or plantar surface. (D) Posterior surface. (E) Anterior surface. (1, posterior border of dorsal surface; 2, anterior border of dorsal surface; 3, medial border of dorsal surface; 1′’, posterior border of medial surface; 2′, anterior border of medial surface; 3′, superior border of medial surface; 4, lateral border of dorsal surface; 5, beak of cuboid; 6, groove for peroneus longus; 7, articular surface for third cuneiform; 8, articular surface for scaphoid; 9, tuberosity of cuboid; 10, posterior border of inferior surface; 11, medial border of inferior surface; 12, superior border of posterior surface; 13, inferior border of posterior surface; 14, superolateral border of anterior surface; 15, superomedial border or base of anterior surface; 16, apex of anterior surface; 17, inferior border of anterior surface; 18, articular surfaces corresponding to metatarsals 4 and 5.) |
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


