The anatomical position
All movement starts from a posture or position, which must be first defined before proceeding to the changes that follow. A common reference must be used to describe the positions, relationships and directions of movement. This reference is the anatomical position, standing upright with the palms of the hands facing forwards, the feet parallel and facing forwards (Figure 2.1). Note that the natural standing position, with the palms of the hands facing the sides, is not used.
Figure 2.1 The anatomical position.
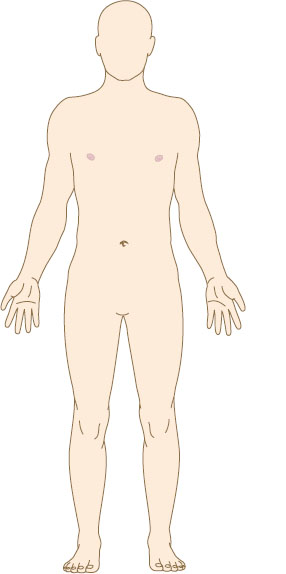
- Look at the articulated skeleton to see the difference between the anatomical position and the natural standing position. In the anatomical position, the bones of the forearm are parallel, and the whole of the palm of the hand can be seen from the front.
- Stand in a natural position, and then change to the anatomical position. Note the change in position of the forearm and hand. Check that the feet are slightly apart and facing forwards.
Planes and axes of movement
The reference anatomical position can now be divided into three planes which lie at right angles to each other. The planes are the fixed lines of reference for movement (Figure 2.2).
Figure 2.2 Planes of movement.
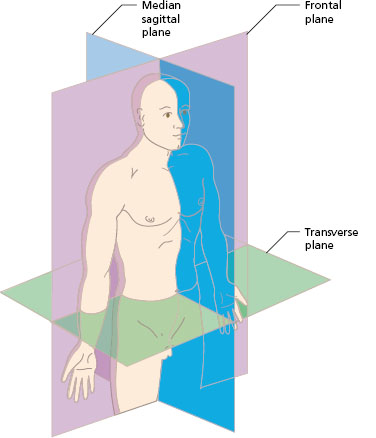
Sagittal (median) plane
The sagittal or median plane is a vertical plane passing through the body from front to back which divides the body into right and left halves. Any parallel plane dividing the body into unequal right and left halves is also said to be a sagittal plane. It is parallel to the sagittal suture in the midline of the skull. The terms medial and lateral relate to this plane. A structure nearer to the median plane is medial, and one further away from it is lateral. For example, the medial ligament of the knee is on the inside of the joint, while the lateral ligament is on the outside.
Coronal (frontal) plane
This plane passes through the body from top to bottom and divides the body into front and back halves. It is at right angles to the sagittal plane. Frontal planes are parallel to the frontal suture of the skull across the crown of the head. The terms anterior and posterior relate to this plane. The anterior shaft of the femur is the front of the bone in the anatomical position, while the posterior shaft is the back of the bone.
Transverse (horizontal) plane
This is parallel to the flat surface of the ground. Planes in this direction divide the body into upper (cranial) and lower (caudal) parts. Crossing the body in this direction, planes are at right angles to the sagittal and frontal planes. The terms superior and inferior relate to this plane. The superior radioulnar joint is near to the elbow (above or towards the head), while the inferior radioulnar joint is adjacent to the wrist (below or towards the ground). When the limbs move to different positions, the terms superior and inferior can become confusing, for example if the arm is above the head. Another way of identifying structures may then be used. The terms proximal and distal mean nearer to the centre of the body or further away from the centre, respectively. The superior radioulnar joint can therefore also be named the proximal joint, and likewise the inferior as distal.
The axis of movement at a joint is at right angles to the plane. Bending the elbow is a movement in the sagittal plane about an axis passing through the frontal plane at the joint. Turning the head from side to side is a movement in the horizontal plane about a vertical axis through the joint between the first and second vertebrae of the neck. It may help to understand plane and axis by thinking of the plane of movement of the wheels of a car, around the axle (axis) at the hub of the wheels. Movements can be classified in terms of the three planes and axes described. Many functional activities, however, occur in diagonal planes. The leg swing in walking does not occur exactly in the sagittal plane at the hip, but in a diagonal plane between the sagittal and frontal planes, so that the foot comes to the ground near to the midline of the body. Movement at the shoulder which carries the arm forwards and slightly across the body is in a diagonal plane.
Structure and movements at synovial joints
Most of the movements of the body occur at the synovial joints. See Chapter 1 for the structure of a typical synovial joint. The synovial joints are classified by the axes of movement (uniaxial, biaxial and multiaxial) and by structure, as follows.
Figure 2.3 Types of synovial joint: (a) hinge; (b) pivot; (c) ellipsoid; (d) ball and socket; (e) plane; (f) saddle.
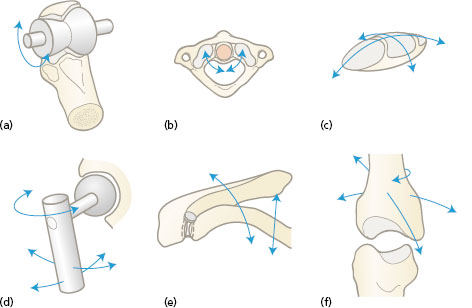
- A hinge joint allows movement in one direction only, in the sagittal plane. It is a uniaxial joint. Examples of a hinge joint are the elbow (Figure 2.3a) and the ankle.
- A pivot joint is restricted to rotational movement around a vertical axis in the horizontal plane. It is a uniaxial joint. Examples are the atlantoaxial joint in the neck, which turns the head to look sideways (Figure 2.3b), and the joints in the forearm that allow the hand to turn so that the palm faces backwards.
- An ellipsoid joint has oval joint surfaces that allow movement in the sagittal and frontal planes, but no rotaion. It is a biaxial joint. Examples are the radiocarpal (wrist) joint (Figure 2.3c), and the joints at the base of the fingers (metacarpophalangeal joints).
- A ball and socket joint allows movement in three planes (Figure 2.3d). It is a triaxial or multi-axial joint. Examples are the shoulder and hip joints.
- A plane joint has flat articular surfaces that allow limited gliding or twisting movement between the bones. An example is the joint between the acromion of the scapula and the clavicle (Figure 2.3e). Plane joints may be arranged in series, so that the cumulative effect of the limited action at each joint gives considerable movement overall. The synovial joints between the bony arches of adjacent vertebrae are examples of plane joints, which together give the overall movements of the trunk (see Chapter 10, Joints of the vertebral column).
- A saddle joint has a surface that resembles a saddle (a concave convexity) with a reciprocally curved surface sitting on it. The movements are in two planes with a limited range of rotation as well. The first carpometacarpal joint at the base of the thumb is a saddle joint (Figure 2.3f).
The range of movement possible at each synovial joint depends on three main factors.
- The shape of the bony articulating surfaces determines both the direction and extent of the movement. For example, the shallow socket of the shoulder joint allows a wide range of movement.
- The position, strength and tautness of the surrounding ligaments affects range. By regular stretching exercises from an early age, gymnasts and ballet dancers can stretch certain joint ligaments to achieve a greater range of movement.
- The strength and size of the muscles surrounding the joint affects range. Bulging muscles around a joint halt movement when the two moving segments come into contact. For example, bending the elbow is limited by contact of the forearm with the upper arm. Other muscles may restrict movement by their position in relation to a joint. Tight hamstring muscles at the back of the thigh limit bending of the hips in touching the toes.
Movement terms
Starting from the anatomical position, paired terms are used to distinguish the direction of movement of body segments in the three planes described (Figure 2.4).
Flexion and extension are movements in the sagittal plane. Flexion movements bend the body part away from the anatomical position. Extension is movement in the opposite direcion back to the anatomical position and beyond into a reversed position (Figure 2.4a). In flexion, the angle between the bones is usually decreased, e.g. flexion of the elbow bends the forearm forwards and upwards towards the arm, and flexion of the knee takes the leg backwards towards the thigh. Flexion movements curl the body into a ball, while extension stretches the body out.
Figure 2.4 Movements at joints: (a) flexion and extension; (b) abduction and adduction; medial and lateral rotation.
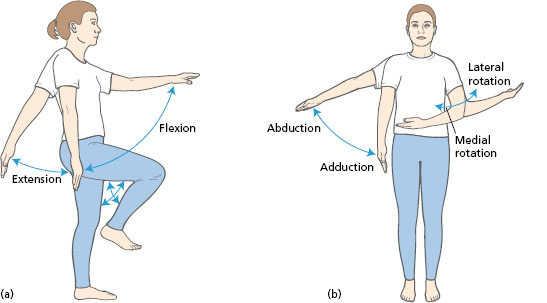
Abduction and adduction are movements in the frontal plane. Abduction movements carry a body part away from the midline. Adduction is movement in the opposite direction towards the midline (Figure 2.4b). In the hands and feet, the movements are related to the central axis of the segment. The fingers move away from the middle finger, and the toes move away from the second toe.
When the return movement continues beyond the anatomical position, the terms ‚hyperextension’ and ‘hyperadduction’ may be used (hyper means ‘more than’).
Rotation is movement in the horizontal plane about a vertical axis. When the bone is rotating away from the midline, or towards the posterior surface, the movement is known as lateral rotation (or external rotation). In the reverse movement, the bone turns in towards the midline of the body and the movement is known as medial rotation (or internal rotation) (Figure 2.4b).
Circumduction is a term used to describe a sequence of movements of flexion, abduction, extension and adduction. The bone moves round in a conical shape, with the apex of the cone at the moving joint and the base at the distal end of the bone. True circumduction does not include rotation.
The paired movement terms are also used to name the groups of muscles producing them. Muscles that bend the fingers are known as flexors of the fingers, while the extensors straighten the fingers. The abductors of the hip carry the leg sideways.
- Stand in the anatomical position. Move each of the large joints in turn, e.g. shoulder, elbow, wrist, hip, knee, ankle.
- Record the movements possible at each of the joints.
Most body movements do not start at the anatomical position, but they are described with reference to that position. To analyse a movement, the starting position must first be defined. For example, lifting a glass from a table to the mouth starts with the shoulder in a neutral position, the elbow flexed, the wrist extended and the fingers flexed around the glass. The changes at each joint are then described as the movement proceeds. To drink, the shoulder must be flexed and the elbow flexed further to bring the glass to the lips.
- Observe some simple everyday activities, such as standing up from sitting, climbing stairs, reaching to a high shelf, and pulling down a blind.
- Record the starting position and list the movements made at each of the joints involved.
Group action and types of muscle work
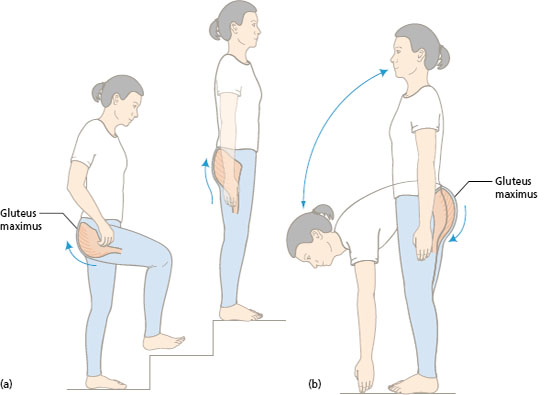
Muscles produce movements at joints by pulling on the bones to which they are attached. To describe a muscle, its attachments are named. One end of the muscle is usually fixed and the bony attachment at the other end moves. The attachment that is usually held steady is known as the origin of the muscle and is usually more proximal. The moving end is called the insertion and is often more distal. Some muscles can work from either end. For example, the muscle that extends the hip (gluteus maximus) pulls the thigh backwards as in climbing stairs (Figure 2.5a). If the trunk is flexed forwards, this hip extensor acts in reverse to pull the pelvis upwards and straighten the trunk on the leg (Figure 2.5b).
Figure 2.5 Muscle attachments. Action of the gluteus maximus in extension of the hip: (a) distal attachment moves; (b) proximal attachment moves.