CHAPTER 56 Minimally Invasive Posterior Approaches to the Spine
Surgical Anatomy of the Posterior Paraspinal Muscles
The posterior lumbar paraspinal muscles are responsible for maintaining spinal posture in its neutral position. Furthermore, the paraspinal muscles guard the spine from excessive bending that would otherwise endanger the integrity of the intervertebral discs, facet joints, and ligaments.1 It is the body’s dynamic stabilizing system that prevents pain and injury to spinal column due to the repetitive loads during the course of daily activities. The posterior paraspinal muscles are composed of several muscle groups that run along the thoracolumbar spine and attach caudally to the sacrum, sacroiliac joint, and iliac wing.
Posterior spine surgery using midline approaches inherently causes damage to surrounding muscles.2,3 Muscle injury leads to long-term muscle atrophy, which in turn leads to decreased force production capacity of the muscle.2,4–12 The multifidus muscle is most severely injured when using this approach for several reasons. First, its medial location inherently requires it be displaced most during retraction. This predisposes the muscle to greater retraction pressures and makes it more vulnerable to disruption of its neurovascular supply.2,7 Of equal importance, the midline posterior approach inevitably leads to disruption of the multifidus tendon attachment to the spinous process, as well as the integrity of the dorsolumbar fascia.
Key Concepts for Minimally Invasive Spine Retraction Systems
A key advancement in minimally invasive surgery came from Foley and colleagues13 with the development of the tubular retractor. A cylindrical retractor allows the surgical corridor to be opened via serial dilation using sequentially larger concentric tubes. This decreases the need for muscle stripping during the exposure. Furthermore, a tubular retractor maximizes the surface contact area, which in turn minimizes the pressure per unit area. Another key concept in MIS is use of a retractor holder mounted to the table instead of using a “self-retaining” mechanism. In a self-retaining retractor system, constant pressure on the tissues must be exerted to hold the retractor in place. Studies show that the maximum intermuscular pressure around a tubular retractor decreases by 50% within 3 seconds.14 Thereafter, the pressure is undetectable. With self-retaining retractors, the pressure remains unchanged.
Posterior Lumbar Approaches
Tubular Microdiscectomy
The treatment of herniated discs via MIS tubular microdiscectomy is the most common technique currently used in the United States. This system, developed by Foley and Smith, consists of a series of concentric dilators and thin-walled tubular retractors of variable length. The use of the tubular retractor, rather than blades, allows the retractor itself to be thin walled (0.9 mm). The tube circumferentially defines a surgical corridor through the erector spinae muscles. The appropriate depth of retractor prevents the muscle from intruding into the field of view. The retractor allows for the appropriately sized working channel to permit spinal decompression. The typical retractor size is 14 to 18 mm for microdiscectomy (Fig. 56–1). Surgery is typically performed using an operating microscope. Several randomized controlled trials have been performed to compare traditional open microdiscectomy with minimally invasive tubular microdiscectomy.15–17 These studies all show that tubular microdiscectomy is safe and efficacious compared with well-established traditional techniques. Clinically significant superiority was not shown, likely reflecting the difficulty is demonstrating differences between the two already successful procedures.
Lumbar Decompression
An important goal of minimally invasive posterior surgery is maintaining the tendinous attachment of the multifidus to the spinous process. During a traditional laminectomy, the spinous process is removed and the multifidus muscle is retracted laterally. Upon wound closure, the multifidus origin can no longer be repaired to the spinous process. The midline approach affords a symmetric view of the posterior elements, which allows for safe resection of the lamina, ligamentum flavum, and medial facets. The symmetric view allows the surgeon to readily identify and orient the surgical corridor. However, a thorough decompression can be achieved without need for removal of the spinous process. In a technique originally described by McCulloch and colleagues,18 the spinal canal can be approached through a unilateral portal via a hemilaminectomy technique. Decompression of the central canal and contralateral recess can be achieved by angling the tubular retractor dorsally to view the undersurface of the spinous process and contralateral lamina (Fig. 56–2). The dural tube can be gently pushed down, and the ligamentum flavum and contralateral superior articular process resected to achieve a bilateral decompression.
The efficacy and safety of minimally invasive posterior lumbar decompression have been assessed in multiple studies.18–24 In a review by Asgarzadie and Khoo,25 this technique provides long-term symptomatic relief equivalent to traditional open surgery but with significant reductions in operative blood loss, postoperative pain, hospital stay, and narcotic usage. The effect of the MIS learning curve remains a significant concern as increased complication rates are seen during the initial series of patients.26 Despite the learning curve, the overall complication rates remain low, even in patients who are elderly or medically frail.27–29
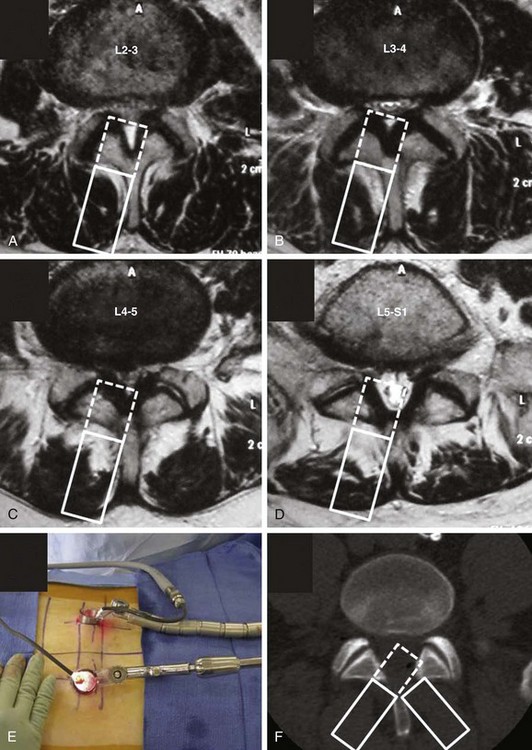
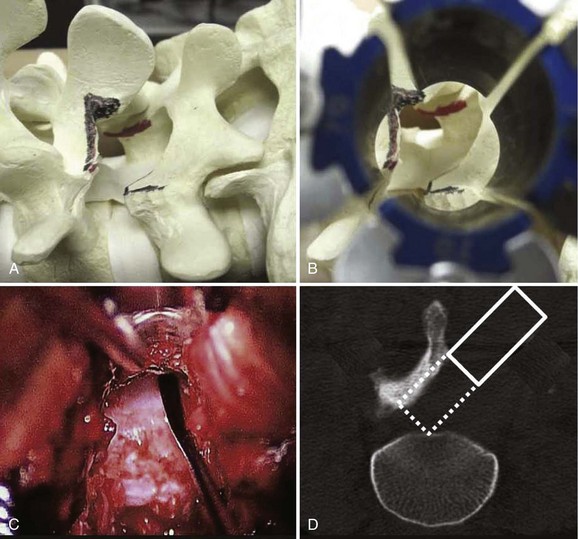
It is important to consider the anatomic variation of the lower lumbar spine with the upper lumbar spine with this particular technique. At L3 and above, the lamina between the spinous process and facet joint can be narrow (Fig. 56–3). With a unilateral approach, it may be difficult to reach the ipsilateral recess without excessively removing the ipsilateral inferior articular process. An option is to use a bilateral cross-over technique to reach the right lateral recess from a left-sided hemilaminectomy and vice versa. Anatomically, the lateral recess is more accessible through a contralateral approach when using the unilateral approach. In a preliminary study of four patients and seven levels of decompression, the total operating time was 32 minutes per level and the estimated blood loss was 75 mL. The average postoperative stay was 1.2 days. All patients had resolution of neurogenic claudication and there were no complications.30
Posterior Lumbar Interbody Fusion
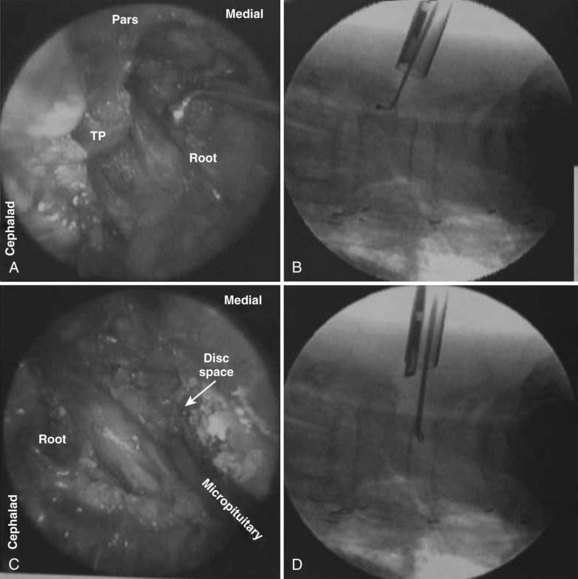
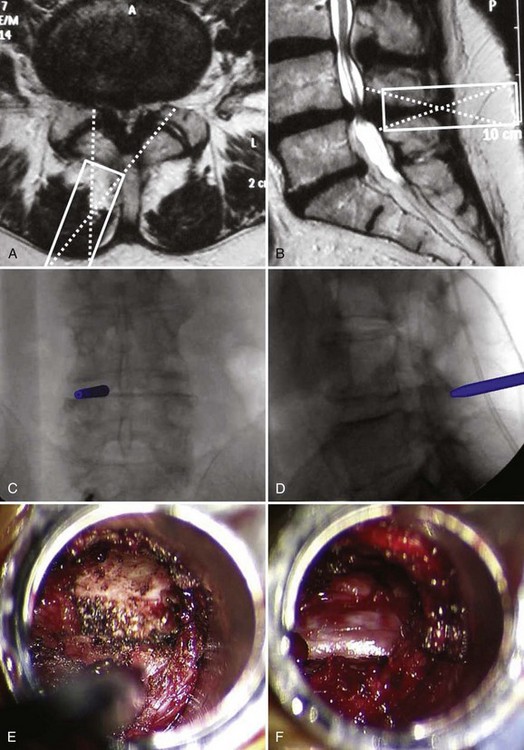
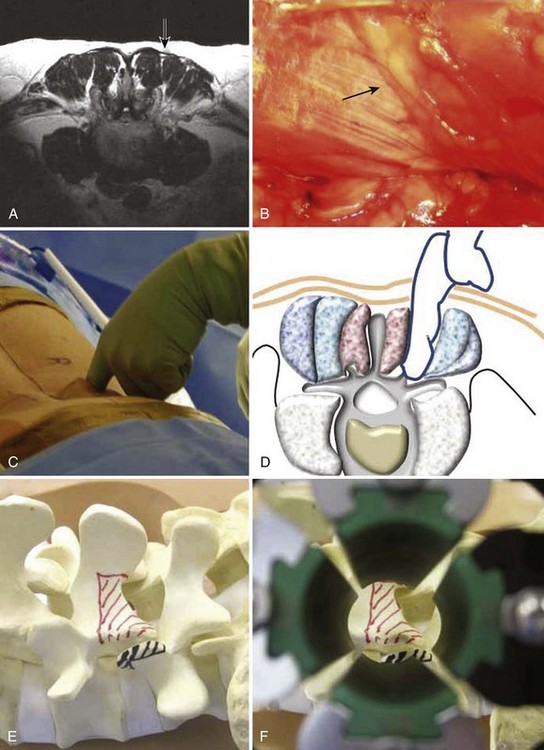
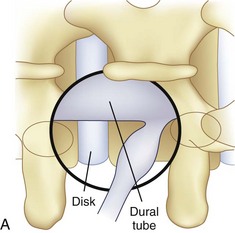
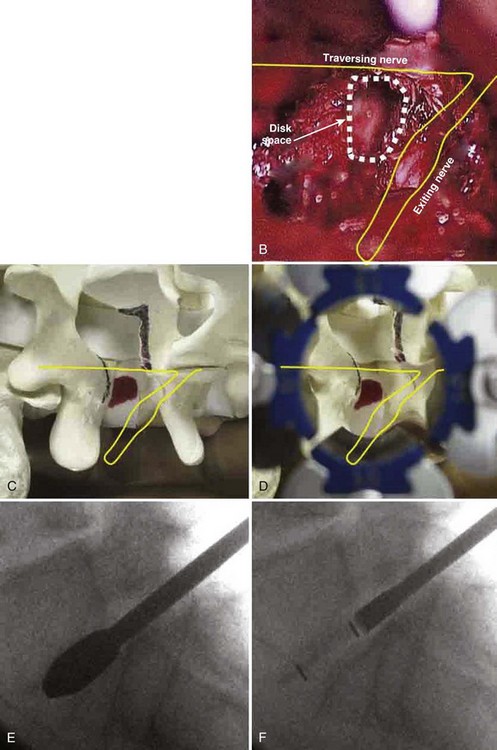
An extension of the minimally invasive hemilaminectomy technique is transforaminal lumbar interbody fusion (MIS TLIF). The unilateral approach is used to perform the analogous decompression and is combined with a complete facetectomy. The surgical corridor is in the neurovascular plane between the multifidus and longissimus muscles (Fig. 56–4). A complete facetectomy allows for decompression of the spinal canal from the ipsilateral to the contralateral side (Fig. 56–5). Access to the disc space is through a window bordered medially by the dural tube, proximally by the exiting nerve root, and distally by the pedicle and superior endplate of the caudad vertebra, thus forming within the Kambin triangle (Fig. 56–6). Angled curettes are used to perform a subtotal discectomy from a unilateral approach. If necessary, an osteotome is used to remove the overhanging rim of the posterior vertebral endplate during discectomy. Fusion is performed using interbody spacers that can be placed anteriorly for maximum lordosis correction. A second cage may be inserted by using the smooth trials to push the first cages to the far side of the disc space. Dual cage constructs may be desirable when there is significant osteoporosis or at L5-S1 in a multilevel fusion.
The clinical safety and efficacy of this technique has been well established. Schwender and colleagues31 reported on 49 patients who underwent MIS TLIF through a paramedian, muscle-sparing approach using an expandable tubular retractor system. Of these patients, 26 patients had degenerative disc disease (DDD) with herniated nucleus pulposus (HNP), 22 had spondylolisthesis, and 1 had a Chance-type fracture as their primary diagnosis. The minimum follow-up was 18 months with a mean follow-up of 22.6 months. Operative time averaged 240 minutes (110 to 310 minutes), and average estimated blood loss (EBL) was 140 mL (50 to 450 mL). No patients required a blood transfusion, and there were no intraoperative complications. Length of hospital stay was 1.9 days on average (1 to 4 days). All 45 patients who had preoperative radicular symptoms had resolution of their symptoms. All patients with mechanical low back pain (LBP) had postoperative improvement of their pain. Four complications were noted postoperatively (two from malpositioned screws, one from graft dislodgement causing new radiculopathy, and the last from radiculopathy caused by contralateral neuroforaminal stenosis). Visual Analog Scale pain scores improved from 7.2 to 2.1, and Oswestry Disability Index scores improved from 46% to 14% at last follow-up.
Numerous studies have since confirmed the safety and efficacy of this technique.32–40 These studies show that MIS TLIF can achieve results comparable with traditional open techniques but with less postoperative pain, decreased blood loss, and shorter hospital stays, particularly when compared with anterior-posterior circumferential fusion.41
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


