Meniscus Root Repair
Eric J. Kropf
Christopher D. Harner
INTRODUCTION
While a wide spectrum of meniscal tear patterns have been well described, “root tears” represent a unique clinical entity that deserves particular attention. During weight-bearing activities, the menisci function as “shock absorbers” dissipating axial loads and containing hoop stresses. In turn, the articular cartilage is shielded from excessive forces. Normal meniscal function is dependent upon several key anatomic features including circumferentially oriented collagen fibers, the coronary ligaments, and the anterior and posterior root attachments that securely anchor the meniscus to the central tibial plateau (10). Root tears compromise this key attachment site and, as a result, have been shown to significantly alter knee kinematics and function (1,7).
The posterior root attachments play a greater role in maintenance of knee stability and are therefore more susceptible to injury. The posterior root of the lateral meniscus is commonly injured in association with acute anterior cruciate ligament (ACL) tears (3,9). More recently, tears of the posterior root of the medial meniscus have been recognized. Such tears have been implicated as a cause of medial meniscal extrusion, joint space narrowing, and rapidly progressive arthritis (6). Following an increased awareness of this specific injury pattern, root repair techniques have been developed. Our technique, which was developed as a modification to our medial meniscal transplantation technique, seeks to restore meniscal function and knee biomechanics by arthroscopically repairing the meniscal root back to the native insertion site.
In this chapter, we describe our current technique for arthroscopically assisted repair of the posterior medial meniscal root. Importantly, a similar repair of the lateral meniscal root can be performed with several minor modifications. The same principles apply to the lateral meniscus.
PREOPERATIVE PLANNING
Clinical Presentation/Physical Exam
Tears of the posterior root of the lateral meniscus are typically seen with acute ACL injury. The valgus twisting mechanism forcefully loads the lateral compartment and can injure the meniscal root. In all patients with acute ACL injury, especially those with extremely large bone bruise patterns, lateral root tears should be suspected.
Root tears of the posterior horn of the medial meniscus typically present with a bimodal distribution (2). Patients ≥40 years of age classically present after an acute sports-related injury often in conjunction with other ligamentous knee injury. Patients ≥40 years of age present following seemingly minor trauma (missing a step, rising quickly from a seated position, etc.) with acute, severe medial knee pain. The patient may note an audible “pop” and swelling. In the most common clinical scenario, physical examination typically reveals an overweight to obese female who walks with an antalgic gait. A minor effusion and slightly limited flexion are common (2,5). Medial joint line tenderness is present, often in the more posterior aspect of the knee.
Imaging
Standardized plain radiographs are performed in all patients who present with acute knee pain or injury. This typically includes a weight-bearing posteroanterior (PA) view (Fig. 23.1), weight bearing 30-degree flexion lateral, and a patellofemoral view. Early degenerative changes may be seen in slightly older patients, but radiographs
will be negative in the vast majority of patients. Magnetic resonance imaging has a high false-negative rate for avulsions or radial tears at the level of the posterior root (7) (Fig. 23.2). A high index of suspicion is imperative to detect root tears.
will be negative in the vast majority of patients. Magnetic resonance imaging has a high false-negative rate for avulsions or radial tears at the level of the posterior root (7) (Fig. 23.2). A high index of suspicion is imperative to detect root tears.
 FIGURE 23.1 Plain radiographs (PA flexion weight-bearing view of bilateral knees) in a 55-year-old woman who presented with 3 months of posteromedial knee pain. |
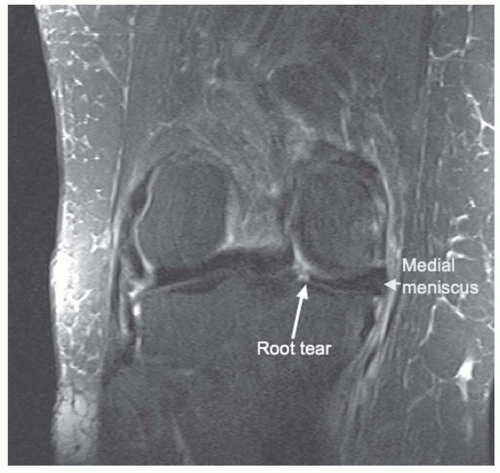 FIGURE 23.2 T2-weighted fat-suppressed coronal image of the right knee. A root tear of the posterior horn of the medial meniscus is seen (white arrow). |
INDICATIONS/CONTRAINDICATIONS
Lateral Meniscus Root Tears
Tears of the posterior root of the lateral meniscus typically occur as the result of acute trauma, often in association with ACL injury. Indications for lateral root repair are similar to those for ACL reconstruction. In the physiologically young patient who wishes to return to his/her previous level of activity, we recommend
repair of the lateral root typically in conjunction with ACL reconstruction. Patients with advanced degenerative changes and low demands (sedentary lifestyle) are typically not surgical candidates.
repair of the lateral root typically in conjunction with ACL reconstruction. Patients with advanced degenerative changes and low demands (sedentary lifestyle) are typically not surgical candidates.
Medial Meniscus Root Tears
With increasing awareness of this clinical entity, indications for repair of the posterior horn of the medial meniscus are evolving. In the young, active patient, we typically recommend meniscal root repair to restore the integrity and ideally, function of the medial meniscus. Unfortunately, the more common clinical scenario involves the overweight to obese 40- to 50-year-old female who presents with acute medial sided knee pain. In this setting, treatment options must be tailored based on the symptoms and desired functional goals of the individual patient. Irrespective of the ultimate treatment plan, we routinely counsel all patients in this population about the benefits of weight management and activity modification, specifically avoidance of deep squatting and repetitive pounding exercises. For patients who are minimally symptomatic, have low functional demands, are of advanced age or simply wish to avoid surgery, we recommend rest, ice, a brief initial course of nonsteroidal anti-inflammatories (2 weeks), and activity modification.
Patients who were previously asymptomatic or minimally symptomatic who present with an acute posterior horn medial meniscus root tear and worsening symptoms are typically good candidates for meniscal root repair. Advanced age, severe degenerative changes, and excessive varus malalignment are contraindications to surgical repair.
SURGICAL TECHNIQUE
Setup
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


