64
Lunotriquetral Instability
Loryn P. Weinstein and Allen T. Bishop
History and Clinical Presentation
A 48-year-old right hand dominant mechanic presented for evaluation of right ulnar-sided wrist pain. Two weeks earlier he had slipped in his shop and landed on a dorsiflexed wrist. The primary impact was to the hypothenar eminence. Subsequently, he developed intermittent ulnar-sided wrist pain, exacerbated by radialulnar deviation. Grip strength was diminished, and he felt his wrist give way when torquing heavy tools. These symptoms reduced his work productivity and prevented him from participating in his weekly bowling league.
Physical Examination
No wrist swelling or obvious deformity was noted. There was point tenderness dorsally over the triquetrum. Range of motion was diminished in all planes. A painful clunk was palpable with radialulnar deviation. Compression of the triquetrum with a radially directed force elicited pain. Excessive laxity was present with lunotriquetral (LT) ballottement when compared with the contralateral wrist. Grip strength was reduced 20% compared with the contralateral, nondominant side. He was neurovascularly intact.
Diagnostic Studies
Anteroposterior, lateral, and oblique radiographs of the wrist were normal. An arthrogram was obtained (Fig. 64–1).
Relative malalignment between the lunate and the triquetrum may be apparent on lateral radiographs. Bisectors of the lunate and triquetrum intersect to form an LT angle (normal = 14 degrees, range −3 to +31 degrees). Patients with LT dissociation will exhibit a negative angle (mean value = − 16 degrees). A volar intercalated segmental instability (VISI) pattern is present in some (chronic) cases.
Radial deviation and clenched-fist anteroposterior views can be useful. Palmar flexion of the scaphoid and lunate without movement of the triquetrum confirms the loss of proximal row integrity.
Arthrography is a useful imaging tool for LT instability. Passage of dye through the LT interspace documents the presence of a perforation, tear, or dissociation. Age-related LT perforations and tears have been frequently demonstrated in asymptomatic individuals. Therefore, arthrogram findings require clinical correlation. A videotaped arthrogram with motion sequences demonstrating abnormal dye pooling associated with abnormal proximal row kinetics is useful as a confirmatory study.
Bone scans, tomograms, and magnetic resonance imaging (MRI) have limited utility in the setting of LT instability. Standards for MRI of LT ligaments are not yet available.
PEARLS
- A standardized PA wrist radiograph yields useful information about ulna variance and impaction.
- LT and TFCC pathology often coexist.
- Dynamic imaging is useful to confirm the presence of LT pathology.
PITFALLS
- Beware of false-positive and false-negative arthrograms Clinical correlation is required.
- Viewing the LT articulation from the midcarpal joint is important to exclude nondissociative midcarpal instability.

Figure 64–1. Patient arthrogram.
Differential Diagnosis
Nondissociative midcarpal instability
Lunotriquetral instability
Ulnar impaction syndrome
Triangular fibrocartilage complex (TFCC) injury
Pisotriquetral injury
Extensor carpi ulnaris (ECU) subluxation
The differential diagnosis of ulnar-sided wrist pain is broad (Table 64–1). However, a history of a specific injury with subsequent instability and “clunking” during radial-ulnar deviation suggests relatively few diagnoses. These include LT instability, nondissociative midcarpal instability, TFCC injury, ulnar impaction syndrome, pisotriquetral injury, and ECU subluxation.
| Diagnosis | Differentiating Findings |
| Triquetrohamate instability | Antecedent trauma, hyperextension mechanism |
| TFCC tear | Painful radial-ulnar deviation and clunk |
| Ulna impaction syndrome | Focal tenderness |
| Pisotriquetral injury | Positive LT provocative tests |
| ECU instability | Positive radiograph findings |
| Positive arthrogram or arthroscopic exam |
TFCC tears can mimic LT instability with an analogous injury history and symptomatic clicking. Provocative LT tests are negative, whereas distal radioulnar joint (DRUJ) and TFCC provocative tests are positive. In some cases, coincident LT and TFCC pathology is demonstrated by arthrography or arthroscopy. Isolated TFCC injury is best visualized by MRI or arthroscopy.
Ulnocarpal impaction syndrome is the result of excessive ulnar positive variance. Pain and weakness with rotational motion are noted. A standard neutral posteroanterior (PA) wrist radiograph will demonstrate ulna positive variance and “kissing” degenerative cysts and sclerosis at the lunate and ulna head. LT and TFCC tears are frequently associated findings. Arthrography or arthroscopy can assess LT and TFCC integrity prior to undertaking an ulnar shortening procedure.
A pisiform fracture may present after acute hypothenar trauma. This is best visualized with a supination oblique or carpal tunnel view radiograph. Radial-ulnar deviation may be painful, but specific LT provocative tests are negative. Pain and crepitance may be found by pisiform compression and translation.
Subluxation of the extensor carpi ulnaris tendon produces an audible snap as the forearm is actively supinated and the wrist is slightly flexed and ulnar deviated. LT provocative maneuvers are negative.
Diagnosis
Lunotriquetral Instability
Lunotriquetral (LT) instability results from a disruption of the dorsal and palmar LT interosseous complex. A spectrum of pathology is possible, proportional to the magnitude and acuity of ligamentous disruption. Degenerative membrane perforation may be asymptomatic. Partial tears of the LT membrane may produce dynamic instability, and complete ligament dissociation may produce a static VISI pattern.
Lunotriquetral instability most commonly follows a specific injury. Hyperextension at the wrist is a common mechanism. Weakness and a decreased range of motion are usually present. Pain is precipitated with radial-ulnar deviation, and sometimes a “clunk” is audible. The individual may perceive instability or a giving-way sensation. Ulnar paresthesias are occasionally present.
Point tenderness is localized to the LT junction. A painful clunk may be palpable with radial-ulnar deviation. Diminished grip strength and radiocarpal motion are common.
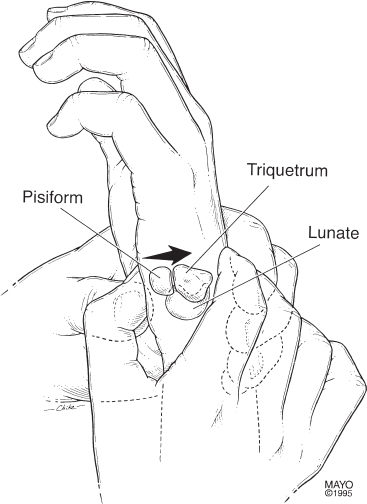
Three provocative maneuvers for LT instability have been described: the compression, ballottement, and shear tests. Compression of the triquetrum in the ulnar snuffbox using a radially directed force may elicit pain, suggesting LT or triquetrohamate pathology. Ballottement of the LT ligament is performed by grasping the pisotriquetral unit between the thumb and index finger of one hand and the lunate between the thumb and index of the other. An anteroposterior translation motion is performed between these bones. Pain and dorsal palmar laxity greater than that on the opposite side signify a positive test. The shear test is performed with the elbow supported on the hand table and the forearm in neutral rotation. The examiner’s contralateral thumb is placed dorsally over the lunate as the ipsilateral thumb loads the pisotriquetral joint from the palmar side (Fig. 64–2). The test is positive when pain, crepitance, or abnormal LT mobility is elicited. Comparison with the contralateral wrist is important for all provocative tests.