CHAPTER 45 Lumbar Disc Disease
The location of the anatomic pain generator in patients with low back pain is often difficult to discern. Pain can originate from several anatomic structures within the spine making it difficult for the patient and the physician to localize. Experimental and clinical studies suggest that the intervertebral disc (IVD) is an important source of back pain in 10% to 39%1,2 of cases of chronic low back pain.
Natural History
At some point during their lifetime, 60% to 80% of adults can be expected to experience low back pain. The annual incidence of back pain in adults is 15%, and its point prevalence is about 30%.3 By the age of 30 years, almost half of adults have experienced a substantive episode of low back pain.4 Most symptoms are short-lived; it is generally believed that 80% to 90% of episodes of low back pain resolve within 6 weeks of onset regardless of the type of treatment.5
Although resolution of symptoms is the common and expected outcome, there is also a high recurrence rate. Croft and colleagues6 reported that although 90% of subjects ceased to pursue consultation about symptoms within 3 months, most still had substantial low back pain and related disability. Additionally, only 25% of the patients who sought consultation for low back pain had fully recovered within 12 months. In a survey of the British general population, 38% of adults reported a significant episode of low back pain within a 1-year period, of which a third had experienced symptoms for longer than 4 weeks.7 Inability to return to work within 3 months of symptom onset is a poor prognostic indicator. Only 20% of patients still disabled after 1 year return to work, and only 2% return after 2 years.8
The clinical onset and course of low back pain may be prolonged for many patients and may best be represented as a continuum of back-related disability and distress.9 Numerous patients presenting with acute low back pain have a prior history of chronic back pain.10 The strongest predictive factor for a new episode of low back pain is a previous episode.11,12
The natural history of DDD is largely unknown. Smith and colleagues13 reported on the outcome of 25 patients with a positive discogram who were treated nonoperatively and found that 68% of patients improved by the 3-year minimum follow-up. Although 60% of the patients were involved with workers’ compensation and 32% were being treated for psychiatric diagnoses, this study suggests that at least two thirds of patients with discogenic pain improve with conservative therapy. The retrospective study design and small sample size limit the conclusions, and because only patients with significant symptoms typically undergo discography, the natural history of untreated symptomatic DDD is likely to be even better.
In their classic description, Kirkaldy-Willis and Farfan14 classified the degenerative process into three distinct phases: dysfunction, instability, and stabilization. In the first phase, the disc loses its normal function as the degenerative process begins. A period of relative instability ensues as degeneration progresses with intermittent episodes of pain. During the instability phase, abnormal motion occasionally can be seen on flexion-extension x-rays; however, more often the spinal segments during this phase of degeneration show no demonstrable radiographic instability. The final phase—stabilization—results when the spinal segment has restabilized because of loss of height and compression of disc tissue, and the patient typically no longer has episodes of back pain. The problem with this theory is that often patients who meet diagnostic criteria of DDD radiographically—loss of height, osteophytes, or even olisthesis—or by magnetic resonance imaging (MRI)—signal changes compared with adjacent levels—are completely symptom-free. Waris and colleagues,15 in a study with 17 years of follow-up MRI, showed that young patients with DDD did show radiographic evidence of progression, but it was not significantly associated with low back pain or a higher rate of surgery.
Relevant Anatomy
The disc is composed of the inner gelatinous nucleus pulposus surrounded by the collagenous anulus fibrosus. Sheets of interlacing lamellae of collagen within the anulus provide tensile strength, which limits the expansion of the viscoelastic nucleus. The nucleus pulposus consists of a matrix of collagen, glycosaminoglycans, and water, which provide compressive stiffness and allow the tissue to undergo reversible deformation. The anatomy of the IVD allows the disc to absorb and dissipate loads on the spinal column and allows motion between adjacent spinal segments. The IVD has sparse cellularity; cells comprise approximately 1% to 5% of the tissue volume. The disc is bordered above and below by a sheet of hyaline cartilage called the vertebral endplate. Pores in the endplates provide channels for diffusion of nutrients to the disc.16
The IVD is largely avascular and aneural, with vascularity and innervation in a healthy disc limited to the peripheral fibers of the anulus. The sinuvertebral nerve innervates the disc, posterior longitudinal ligament, ventral dura, posterior anulus, and blood vessels. It comprises a sensory branch from the ventral root and a sympathetic branch from the gray rami communicans near the distal pole of dorsal root ganglion. The sinuvertebral nerve is believed to have three segmental levels of overlap, which makes it difficult to localize pain originating in the disc, dura, and posterior longitudinal ligament. Nakamura and colleagues17 treated 33 patients with selective L2 nerve root block with good relief of back pain. The authors hypothesized that the main afferent pathways of pain from lower lumbar IVDs in patients with discogenic back pain are sympathetic in nature and are mediated through the L2 nerve root via the sinuvertebral nerve; however, this hypothesis has yet to be validated.
Changes in Disc Structure with Aging and Degeneration
The number of arterioles supplying the peripheral disc diminishes significantly as remaining blood vessels are obliterated by calcification of the cartilaginous endplates. Loss of endplate vascularity and porosity leads to a reduction in the influx of nutrients and efflux of waste products. Lactate levels increase locally within the hypovascular disc secondary to increased production and decreased removal. Cell apoptosis occurs as a result of decreased tissue pH,18 and the biosynthetic reparative capability of the disc is impaired further.
The degenerative process resulting from matrix changes and internal structural disruption sets the stage for abnormal motion at the degenerated segment. Changes in disc structure alter the loading response and alignment of the spinal column. These changes can influence the facet joints, ligaments, and paraspinal muscles, which may also become pain generators. Pain does not always correlate with morphologic changes in the disc and mechanical compression, however.19 Macnab20 described traction osteophytes around the vertebrae originating 2 mm from the anterior endplate, at the site of attachment of the outermost annular fibers. These osteophytes were thought to be signs of abnormal biomechanics, caused by traction at the insertion of the annular fibers into the vertebral bodies. Subsequent studies found these osteophytes to be inconsistently present.
Associated Factors
Various risk factors have been implicated in the pathogenesis of lumbar disc degeneration. In a review of factors associated with IVD degeneration in elderly adults, Hangai and colleagues21 cited increased age, high body mass index, occupational lifting, sporting activities, and factors associated with atherosclerosis as risk factors. Multiple studies show the genetic contribution to degenerative low back pain.22 Battie and colleagues23 estimated the familial contribution to IVD degeneration to be 34% to 61%. Cigarette smoking has also been implicated and seems to have an adverse vasoconstrictive and atherosclerotic effect on the nutrition of the IVD.24,25 Type of occupation has also been shown to have an adverse effect on lumbar spinal segment degeneration, increasing the risk of symptomatic DDD. Studies have implicated occupations that require repetitive lifting or pulling, prolonged sitting26 such as motor vehicle driving,27 and whole-body vibration.28
Arun and colleagues29 used serial postcontrast MRI to study the effect of prolonged mechanical load on diffusion into the IVD. The authors reported that 4.5 hours at a load corresponding to 50% body weight significantly retarded the diffusion of small solutes into the center of the IVD, and it required 3 hours in an unloaded recovery phase to return the diffusion rate to that seen in the unloaded disc. Prolonged mechanical load can cause a disruption of diffusion, which may accelerate disc degeneration; however, this hypothesis has not been confirmed clinically.
The genetic predisposition to lumbar DDD and lifetime exposures were studied in a classic monozygotic twin study by Battie and colleagues.23 These investigators reviewed 115 male identical twin pairs for exposures to common risk factors such as occupation, recreational activities, driving, and smoking. Disc degeneration was determined by MRI and clinical evaluation. In the upper lumbar spine, only 7% of the variability was explained by occupation, 16% was explained by age, and 77% was explained by familial aggregation. In the lower lumbar spine, recreational physical loading explained 2% of variability, age explained 9%, and familial aggregation explained 43%. Battie and colleagues23 concluded that primarily genetic and other unexplained factors result in DDD, whereas commonly implicated environmental factors have only modest effects. In a 5-year follow-up study of the same twin population, the same investigators reaffirmed that genetics have a dominant role in progression of DDD, whereas occupational lifting and leisure activity had only modest effects.30 The important role of genetic factors has been corroborated in other twin studies,31,32 but it seems to be less of an explanatory factor for back pain in older people.33
Several gene loci have been discovered that are associated with increased risk for DDD. Type IX collagen was one of the first gene loci identified with some aberrant alleles imparting a threefold or fourfold increase in relative risk.34–36 More recent publications also implicate collagen type XI, interleukin (IL)-1, aggrecan, vitamin D receptor, matrix metalloproteinase (MMP)-3, and cartilage intermediate layer protein (CILP) as candidate genes.37 The discovery of these genetic risk factors has yet to result in new useful diagnostic and treatment modalities, however.
Pathophysiology
Internal Disc Disruption
Crock19 coined the term internal disc disruption in 1970 and defined it as a painful increase in biologic activity of the IVD after injury with normal radiographic, computed tomography (CT), and myelogram examinations but an abnormal discogram. IDD as a cause of discogenic back pain is controversial. The advent of MRI has dramatically improved the detection of this entity—IDD manifests as a dark disc with relatively preserved height and contour on MRI. Pain in IDD is thought to be caused by mechanical and chemical stimulation of nociceptors within the anulus or on the surface layers of the anulus and the overlying ligamentous tissue. The hallmark of IDD is the absence of disc herniation, prolapsed disc material, segmental instability, or other radiographic abnormality.19,38 Nerve root irritation, radicular pain, and neurologic deficits are also absent.
Radiographic changes associated with DDD—significant disc space narrowing, endplate osteophyte formation, endplate sclerosis, and gas formation within the disc space—are not seen in IDD.39 MRI (dark disc) and positive discography (concordant pain in the abnormal level and not at normal adjacent levels) are required to make the diagnosis of IDD. Because of the poor sensitivity and specificity of discography, many clinicians question the existence of IDD as a clinical entity.
Degenerative Disc Disease
The precise pathophysiologic mechanism for chemically mediated induction of hyperalgesia within the disc has yet to be fully elucidated. Radial annular tears provide a route for nuclear material and noxious chemicals to leak from the disc and contact the dural sac and nerve roots; some studies have shown that autologous nucleus pulposus alone has the capacity to produce an inflammatory response. Additionally, degradative changes can occur within nerve roots exposed to nuclear material even in the absence of mechanical compression.38,40–42 Weinstein and colleagues43 investigated the reproduction of pain on discography and concluded that various neurochemical changes within the disc are expressed by sensitized annular nociceptors. These nociceptors are terminal nerve endings of sensory neurons that selectively respond to painful stimuli by the release of substance P.44 These chemicals are leaked into the epidural space and are transported into the axons of the exiting nerve roots. Within the nerve root, they alter the excitability of type C nerve fibers and initiate the production of inflammatory agents such as prostaglandins, which results in radicular pain.20,45,46
In addition to material from the nucleus pulposus, many other substances in the degenerated disc have been implicated in pain generation. The role of nitric acid and phospholipase A2 in irritation of nerve roots has been well documented.45,47–50 Phospholipase A2 has been implicated in multiple aspects: (1) direct activation of nociceptors, (2) nerve injury from degradation of cell membrane phospholipids, and (3) nerve injury from inflammatory mediators created from the arachidonic acid cascade (i.e., prostaglandins and leukotrienes).51–53 Burke and colleagues54 reported on the elevation of inflammatory mediators within the disc, such as IL-6, IL-8, and prostaglandin E2. Other studies have shown the presence of inflammatory cytokines in the facet joints,55 suggesting facet involvement as a pain generator via a biochemical mechanism as well. Ohtori and colleagues56 reported on ingrowth of nerve tissue immunoreactive for tumor necrosis factor and prostaglandin P in 18 surgically harvested vertebral endplates of patients with Modic stage I and II changes who had undergone surgery. Their findings suggest that axon ingrowth into the vertebral endplate in association with Modic changes was induced by tumor necrosis factor and may be related to pain generation.
Neurovascular proliferation within and around degenerated disc elements has been proposed as another mechanism of pain generation. Normal IVDs have sparse innervation and vascularity that is distributed mainly within the outer lamellae (3 mm) of the anulus fibrosus,57,58 whereas degenerated discs have significant neurovascular ingrowth within the inner anulus and nucleus pulposus.59 Immunoreactive staining and acetylcholinesterase studies have shown penetration of nerve fibers within the inner third of the anulus in association with neovascularized granulation tissue.47,57 Peng and colleagues60 reported a histologic study of 19 IVDs harvested from surgery compared with normal control discs. The distinctive histologic characteristic of painful discs was a zone of richly innervated vascular granulation tissue extending from the outer anulus to the nucleus along the edges of fissures. Proliferation of vascular channels and sensory nerve endings rich in calcitonin gene-related peptide has also been observed in the endplate region and vertebral body adjacent to the degenerated disc. These findings suggest a role for the vertebral endplate and body as additional pain generators in DDD.61
Other studies suggest that the sensory nerve supply within the IVD is similar to visceral innervation patterns,62 with calcitonin gene-related peptide immunoreactive fibers that pass through the sympathetic trunks.63 This visceral pattern of innervation is potentially susceptible to central sensitization, which may complicate chronic low back pain further with psychosomatic overtones.64 Psychosocial and chronic non–back pain syndromes have been implicated in more recent publications as having a significant effect in patients with low back pain.65–69
Clinical Picture
Internal Disc Disruption
The pain is characterized as a deep, dull ache in the lower lumbar region, exacerbated by rotation, flexion, and side-bending movements, and partially relieved by rest. Sitting intolerance may be a primary complaint, and pain is often relieved in a lateral recumbent position. Occasionally, there is a complaint of pain in the buttock or posterior thigh, but there is a conspicuous lack of radiculopathic symptoms. In the rare instances of associated leg pain, it is usually a late finding and pain does not follow any dermatomal pattern. In a study involving intradiscal electrothermal annuloplasty in 25 patients, O’Neill and colleagues70 showed that stimulation of the IVD may result in low back and referred leg pain in patients presenting with symptoms of IDD. The distal distribution of pain was found to depend on the intensity of stimulation, and occasionally pain extending below the knee was produced.
Diagnostic Imaging
Plain Radiography
Plain radiographs are the recommended initial imaging modality for patients with a complaint of low back pain. Classic comparative and cost benefit studies have been done to determine when and what radiographs to obtain.71,72 In 1982, Liang and Komaroff73 published a comparison study between performing radiographs on all patients versus performing radiographs only on patients whose pain did not improve within 8 weeks of presentation. They found that risks and costs did not justify obtaining radiographs on initial presentation. Scavone and colleagues74 reviewed the radiographs of 782 patients and found that spot lateral and oblique films added diagnostic information in only 2% of patients. They recommended that a spine series in patients with low back pain should consist only of anteroposterior and lateral films. Generally, flexion-extension and oblique views are necessary only in patients suspected to have instability or a pars fracture. The presence of “red flags” increases the chances of diagnostic radiographic findings and may prompt the physician to obtain early radiographic studies. These “red flag” indications are summarized in Table 45–1.75
TABLE 45–1 Practice Guidelines—“Red Flags”
From Institute for Clinical Systems Improvement (ICSI): Adult Low Back Pain. Bloomington, MN, ICSI, 2008.
Magnetic Resonance Imaging
The MRI finding of a HIZ was originally described by Aprill and Bogduk76 in 1992 and is believed to be specific for an annular tear (Fig. 45–1). Postmortem studies have shown three types of tears that can occur in the anulus: concentric, transverse, or radial.77,78 A concentric tear is a crescentic or oval cavity created by a disruption in the short transverse fibers interconnecting the annular lamellae and is usually not visible on MRI. Concentric tears are occasionally referred to as delamination. A transverse tear represents a rupture of Sharpey fibers near their attachments to the ring apophysis at the disc periphery; these tears are typically thought to be clinically insignificant. A radial tear extending from the nucleus pulposus to the outermost surface of the posterior anulus is manifest on MRI as a HIZ.79 HIZ is visualized on spin-echo T2-weighted images as a high-intensity signal located within the anulus fibrosus and is clearly distinguishable from the nucleus pulposus.
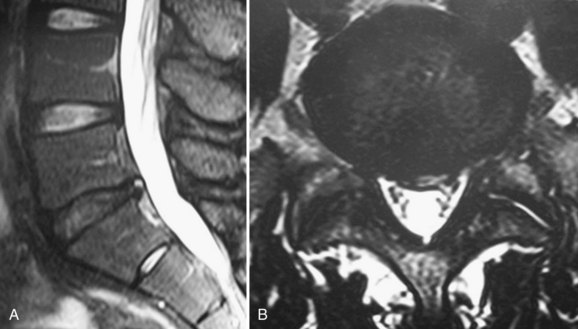
Endplate changes (Fig. 45–2) that occur with disc degeneration have been well described by Modic and colleagues.80 Stage I change represents edema and is characterized by decreased signal on T1 and bright signal on T2 within the endplate. In stage II, fatty degeneration in the bone adjacent to the endplates is represented by bright signal on T1 and intermediate signal on T2 sequences. Stage III changes correspond with advanced degenerative changes and endplate sclerosis and are characterized on MRI by decreased signal intensity on T1-weighted and T2-weighted images.

FIGURE 45–2 A and B, T1-weighted (A) and T2-weighted (B) sagittal MRI showing Modic stage I endplate changes.
When interpreting MRI findings, the clinician must be careful to consider the high prevalence of clinically false-positive findings. Abnormal disc findings on MRI are often found in clinically asymptomatic individuals. Boden and colleagues81 showed that approximately 30% of asymptomatic individuals have a major finding on lumbar MRI scans. In patients older than 60 years, such abnormal findings are almost universally present regardless of symptoms. Jensen and colleagues82 reported on 98 asymptomatic patients 20 to 80 years old and found that 52% overall had disc bulge in at least one level on MRI. Stadnik and colleagues83 showed an unusually high rate of disc bulge (81%) and annular tears (56%) on MRI in 30 asymptomatic volunteers.
Abnormal MRI findings in asymptomatic patients are not indicators of future problems. Borenstein and colleagues84 reported on 50 of the 67 patients from the study by Boden and colleagues81 at a 7-year follow-up interval and found that incidental MRI findings were not predictive of the development or duration of low back pain. Jarvik and colleagues85 studied 148 veterans with no symptoms of low back pain for at least 4 months. They found an incidence of moderate to severe desiccation in at least one disc in 83% of patients, disc bulge in 64%, and loss of disc height in 58%. In a 3-year follow-up of the same cohort, the investigators found no association between the development of new back pain and incidental MRI findings such as Modic changes, disc degeneration, annular tears, or facet degeneration. The greatest risk factor for developing low back pain in the 3-year interval was depression.65
Jarvik and colleagues86 also published a report on the use of early MRI in the primary care setting. They randomly assigned 380 patients with low back pain to receive initial spine imaging via rapid MRI or plain radiography. Jarvik and colleagues86 reported that substituting rapid MRI for x-ray studies in the primary care setting offered little additional benefit to patients in terms of secondary outcomes measures at 1 year and had the potential to increase the cost of care by $320 per patient (in 2002 dollar value). Carragee and colleagues87 performed a prospective study of 200 asymptomatic patients to determine the rate at which new episodes of low back pain are associated with changes on MRI. On follow-up MRI in 51 patients who developed an episode of low back pain, 84% had no new finding. The most common new findings were disc signal loss (dark disc), progressive facet arthrosis, and increased endplate changes. New findings were not more common in patients developing back pain after minor trauma. The conclusion was that new findings on MRI within 12 weeks of onset of a serious episode of low back pain were unlikely to represent any significant structural change and preexisted the onset.
Contrast-Enhanced Magnetic Resonance Imaging
Lappalainen and colleagues,88 in an animal study of surgically created annular tears, showed that gadolinium-enhanced MRI did not detect all tears; specifically, peripheral, small tears were not visualized, but these tears would still represent clinically significant disc disruption. Yoshida and colleagues89 investigated the relationship between T2-weighted gadolinium DTPA–enhanced MRI and a positive pain response with discography of 56 lumbar discs in 23 patients with chronic low back pain. The sensitivity, specificity, positive predictive value, and negative predictive value of the unenhanced T2-weighted images in detecting the symptomatic disc were 94%, 71%, 59%, and 97%, whereas the same values for gadolinium DTPA–enhanced images were 71%, 75%, 56%, and 86%. The findings of Yoshida and colleagues89 support the use of unenhanced T2-weighted MRI in detecting symptomatic disc pathology in appropriately selected patients, while avoiding unnecessary discography in patients with chronic low back pain.
High-Intensity Zone
In an attempt to find a noninvasive means of diagnosing IVD pathology with a high degree of certainty, several studies have investigated the correlation between positive provocative discography and various findings on MRI, such as HIZ, decreased disc intensity (dark disc), and Modic vertebral endplate changes. In their original publication, Aprill and Bogduk90 correlated the finding of a HIZ with CT discography and found an 86% positive predictive value for a positive discogram; however, the predictive value and clinical significance of HIZ on MRI has been brought into question more recently. Multiple authors91–94 have found a positive correlation between the finding of a HIZ and concordant pain on discography similar to the findings of Aprill and Bogduk,90 whereas others95,96 have documented the correlation but found unacceptably low sensitivity.
In a study of 62 patients 17 to 68 years old, Kang and colleagues97 found that only a HIZ in association with disc protrusion correlated with concordant pain on discography. Specificity was 98%, and positive predictive value was 87%; however, the sensitivity was still low at 46%. HIZ in association with either a normal or a bulging disc on MRI was not found to be associated with positive discogram. In a 30-patient study, Ricketson and colleagues98 were unable to find any correlation between the presence of a HIZ on MRI and a concordant pain response on discography; however, these authors noted that a HIZ was never visualized in a disc found to be morphologically normal on discography. Further studies49,92,99–101 attempting to correlate positive HIZ findings on MRI and painful discography suggest that although lumbar IVDs with posterior combined annular tears are likely to produce pain, the validity of these signs for predicting discogenic lumbar pain is limited.
Although the exact prevalence is unknown, a HIZ can be seen occasionally in asymptomatic individuals.44 Carragee and colleagues67 reported the prevalence of a HIZ in 59% of symptomatic patients and 24% of asymptomatic patients. In the asymptomatic group, 69% of the discs with a HIZ were positive on discography, whereas 10% of the discs without a HIZ were positive. Carragee and colleagues67 also reported that 50% of the discs with a HIZ were positive on discography in patients with normal psychometric testing compared with 100% positive discography results in patients with abnormal psychometric testing or chronic pain. They concluded that the presence of a HIZ does not reliably indicate the presence of symptomatic IDD because of the high prevalence of HIZ in asymptomatic patients.
In 2004, Mitra and colleagues102 published a study of 56 low back pain patients with the finding of a HIZ followed longitudinally for 6 to 72 months with MRI. Changes in HIZ on follow-up MRI—either an increase in intensity or spontaneous resolution—were not correlated to changes in visual analog scale (VAS) score, Oswestry Disability Index (ODI), or symptoms, which calls into question the clinical significance of HIZ. Although HIZ on MRI has been found in some studies to have good specificity and positive predictive value for concordant pain generation on discography, it has low sensitivity, high false-positive rates, and questionable clinical significance.
Dark Disc
Whether a dark disc by itself is painful is another controversial topic. Most patients with a dark disc are asymptomatic; however, in some patients, the disc can be a source of pain. Milette and colleagues103 found that loss of disc height and abnormal signal intensity were highly predictive of symptomatic tears extending beyond the anulus. Horton and Daftari104 reported a positive discogram in 50% of patients with dark discs without evidence of an annular tear. An isolated dark disc with concordant pain on provocative discography is often considered to be pathologic in the absence of other potential sources of pain and in the absence of confounding psychosocial issues; however, as discussed previously, this evidence is weak.
Modic Endplate Changes
The various stages of Modic changes are thought to be specifically linked with phases of the degenerative disc process. Toyone and colleagues105 evaluated MRI scans of 74 patients with Modic changes and found that stage I changes tended to be associated with complaint of low back pain and correlated to segmental hypermobility. Other investigators also described Modic stage I changes as specifically associated with low back pain.106,107 In a large retrospective review by Thompson and colleagues,108 Modic changes in 736 patients were correlated to provocative discogram. These authors found that Modic stage I changes had a high positive predictive value (0.81) for a positive discogram. Modic stage II changes had a lower positive predictive value (0.64), and the predictive value of Modic stage III changes was not statistically significant.
In the original description of vertebral body marrow changes by Modic and colleagues,80 the conversion between signal characteristics from stage I to stage II was described in five of six patients over the course of 14 months to 3 years. Mitra and colleagues109 performed a more recent prospective evaluation of 48 patients with Modic stage I changes. At 12 months to 3 years of follow-up, 37% were found to have progressed to Modic stage II, 15% partially progressed, and 40% had more extensive Modic stage I changes. Stage I changes are believed to represent the unstable, dynamic phase of the degenerative process and tend either to convert to a stage II pattern or to become more pervasive. Modic stage II changes are thought to be stable and less associated with painful episodes, but there have been reports of stage II changes converting back to stage I.110 Kuisma and colleagues111 reported the prevalence of Modic changes in 60 patients treated nonoperatively for sciatica to be 23%. In a longitudinal follow-up of the same patients at 3 years, 14% were noted to have changed type. The levels that did not convert were found to have more extensive Modic changes. Development of Modic change at previously unaffected levels was found in 6%.
Many authors have explored the correlation between Modic changes on MRI with positive concordant pain on discography. Sandhu and colleagues112 found that both were relatively specific for discogenic pain, with no significant correlation between them. Braithwaite and colleagues113 found the Modic changes did not predict positive response on discography; they concluded that Modic changes may represent a specific but relatively insensitive sign of discogenic low back pain. Kokkonen and colleagues114 observed that contrast injection during discography reflected well pain of discogenic origin, whereas the pain associated with endplate damage was usually not shown by CT discography. These authors found a stronger association between endplate degeneration and disc degeneration than between endplate degeneration and annular tears, which may explain why Modic changes have been found to be less sensitive for discogenic pain than discography.
Conversely, other studies have found better correlation between back pain and Modic changes than the correlation between back pain and discography. Carragee and colleagues66 reported on 100 prospectively followed asymptomatic patients who were at high risk for developing disabling back pain. Of all the incidental diagnostic findings, only moderate or severe Modic changes of the vertebral endplates were found to be weakly associated with subsequent development of a disabling episode of back pain. Other structural MRI findings and concordant pain with discography correlated only weakly with previous back pain episodes and had no association with future disability or medical consultations for back pain. Psychosocial, neurophysiologic (chronic nonlumbar pain), and occupational factors strongly predicted future disabling episodes and consultations for back pain.
In a cross-sectional study of 109 women from two groups, nursing or administrative professions, Schenk and colleagues115 found that Modic changes and nerve root compromise were the only MRI findings that were statistically significant predictors of low back pain. Signs of disc degeneration, disc herniation, HIZ, and facet arthritis were found in both groups but were not significant risk factors for low back pain.
Similar findings were reported in a study by Kjaer and colleagues,116 in which complaint of low back pain was correlated to MRI findings in a random selection of 412 Danish subjects. Although Modic changes occurred in less than 25% of subjects (16% Modic stage I and 7% Modic stage II), this finding had the strongest correlation with complaints of back pain. When the subjects were evaluated clinically, the authors found that patients with radiographic evidence of DDD and Modic changes had the best clinical evidence of disc disease. Clinical findings in patients with radiographic evidence of disc degeneration without Modic changes were not significantly different from the baseline population. Kjaer and colleagues117 concluded that Modic change was a critical finding in relation to history of low back pain and clinical findings. In a follow-up study of the same Danish population, Modic changes correlated with type of occupation, history of smoking, and overweight. The odds ratio for heavy labor combined with smoking was 4.9 for the presence of Modic changes on MRI.118
A meta-analysis review of Modic changes by Jensen and colleagues119 found that the median prevalence of Modic changes from all studies was 43% in patients with nonspecific low back pain. A positive association between low back pain and Modic changes was reported in 7 of 10 studies with odds ratios between 2.0 and 19.9.
Axially Loaded Magnetic Resonance Imaging
There has been interest more recently in the potential role of axially loaded MRI in evaluating patients with lumbar spinal diseases. The idea is to use axial loading to reproduce better the anatomy of the disc under physiologic load. The utility of axially loaded MRI has been studied much more extensively in patients with spinal stenosis and spondylolisthesis.120–123 Danielson and Willen124 observed a significant decrease in dural cross-sectional area between a psoas-relaxed position and axial compression in extension in 56% of asymptomatic individuals. The decrease was most pronounced at L4-5 and was worse in older individuals. Although the clinical role of axially loaded MRI in patients with discogenic back pain has not yet been established, Saifuddin and colleagues125 postulated that lumbar spine MRI with axial loading may increase the sensitivity for the detection of HIZs; however, this hypothesis has not been tested.
Discography
There is significant controversy in the literature surrounding the usefulness of discography for the evaluation of the integrity of the lumbar disc. Some investigators consider discography to be the most important tool in the diagnosis of IDD,43,126 but more recent outcome studies127 and a practice guideline by the American Pain Society128 have recommended against the use of provocative discography in the diagnosis of discogenic back pain.
Discography is the only physiologic modality used to determine if a specific disc is a pain generator. Although several attempts have been made to explain the pathogenesis of pain provocation during discography, the precise pathomechanism is not well understood. There are four components to the evaluation of a discogram: (1) the pressure and volume of fluid injected into the disc, (2) the morphology of the disc being injected, (3) the subjective pain response at the level of interest, and (4) the pain response when adjacent control levels are injected.129,130 The subjective pain response to low-pressure provocation is the most important determinant of disc derangement; reproduction of the patient’s symptoms on injection of the diseased level is essential to a positive test. A normal disc can accept 1 to 1.5 mL of contrast medium. If 2 mL or more of contrast agent is easily introduced, some degree of disc degeneration is assumed.
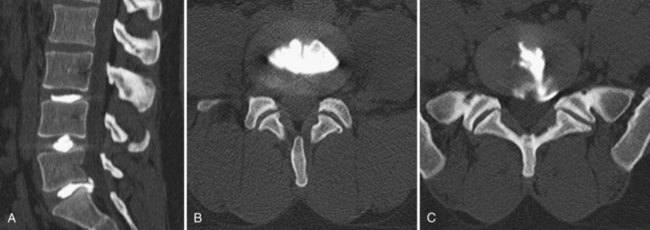
The use of postdiscography CT has also been reported to increase the sensitivity for the diagnosis of radial tears of the anulus.131 Because of low specificity and sensitivity, postdiscography CT is not as helpful, however, in the diagnosis of IDD. Most authors believe that to be diagnostic, not only should the pain be concordant on low-pressure injection, but also a normal control disc should be pain-free (Fig. 45–3).
Despite being used since 1948, discography remains controversial. Holt126 and Massie132 published in the 1960s on the high false-positive rate of lumbar discography, which was found to be 26% by Holt. Walsh and colleagues133 later published a rigorous study on the reliability of lumbar discography. Their study compared 10 normal volunteers with 7 symptomatic patients. Although 17% of the normal discs were found to be morphologically abnormal, there were no positive pain responses. Walsh and colleagues133 concluded that with modern techniques the false-positive rate of lumbar discography is not as high as reported by Holt.126
Derby and colleagues134 found similar results in a more recent study of 90 patients with low back pain and 16 controls. Morphologically, the prevalence of grade III annular tears was 58% among the asymptomatic control population. Presumably, asymptomatic discs in symptomatic individuals on pressure-controlled discography showed pain levels and responses similar to the control group, whereas patients with true-positive discography showed pain characteristics concordant with their usual symptoms. Derby and colleagues134 concluded that pressure-controlled discography can differentiate between asymptomatic discs and morphologically abnormal discs.
Carragee and colleagues68 studied the false-positive rate of low-pressure discography in a comparison of 69 volunteers with no significant low back pain and 52 patients undergoing discography in consideration for treatment of discogenic pain. Low-pressure discography was positive in at least one level in 27% of the patients with low back pain and in 25% of the controls. The false-positive rate of discography was 25% and correlated with psychosocial factors and history of chronic pain of a non-lumbar origin. In another publication from Carragee’s group,69 psychosocial factors and chronic nonlumbar pain, such as cervical pain and somatization disorder, also correlated with positive discography in patients without symptoms of low back pain. These authors concluded that false-positive rates can be low with strict application of the Walsh protocol133 in patients who do not have positive psychometric issues or other chronic pain syndromes.
In contrast to reports of high false-positive rates, two more recent meta-analyses of low-pressure discography report strong evidence to support the role of discography in identifying patients with discogenic pain.135,136 Combined data from all studies showed an overall false-positive rate of 9.3% per patient and 6% per disc. False-positive rates among asymptomatic patients were 3% per patient and 2.1% per disc. Chronic pain was not found to be a confounder, and strength of evidence was reported as level II-2 in support of the diagnostic accuracy of discography.
Finding a “gold standard” with which discography results can be compared remains a problem. Few studies have compared the use of discography and outcomes after surgical fusion, which is perhaps the best measure for the validity of discography. Colhoun and colleagues,137 in a study of 137 patients, reported 89% favorable outcomes in patients with positive concordant pain on discography versus 52% favorable outcomes among patients who had no painful response. Madan and colleagues138 had different findings; 81% of 41 patients who underwent fusion based on MRI findings had satisfactory outcomes versus 76% of 32 patients who had surgery based on discography. Perhaps the most rigorous study to date was published by Carragee and colleagues.139 In their study, success of surgical fusion was compared in 32 patients with single-level positive discogram and a matched cohort of 34 patients with single-level spondylolisthesis; 72% of the patients with spondylolisthesis met the highly effective success criteria for surgery versus only 27% of the patients with discogenic pain. Minimal acceptable success criteria were 91% and 43%. Carragee and colleagues139 calculated a best case positive predictive value for discography of 50% to 60% and concluded that provocative discography was not highly predictive of single-level discogenic back pain.
In an attempt to improve on the poor reliability of discography, interest has turned to functional anesthetic discograms, also called discoblocks. A discoblock is a modification of discography, in which a local anesthetic, usually bupivacaine, is infused with the contrast agent into the disc to enhance the diagnostic capability of the procedure. Relief of pain after discoblock is considered diagnostic for discogenic pain. Ohtori and colleagues140 published a randomized controlled study comparing standard provocative discogram with discoblock in diagnosing discogenic low back pain. Anterior lumbar interbody fusion (ALIF) procedures were performed in 15 patients whose discogenic pain was diagnosed with the aid of discography and 15 patients whose pain was diagnosed with the aid of discoblock. Outcome measures (ODI, VAS, and Japanese Orthopaedic Association score) at 3-year follow-up showed better results that were statistically significant in the group in which diagnosis was aided by discoblock.
Regardless of the details of how discography is performed, some authors have posed the question of potential ill effects resulting from perforating the lumbar disc. Carragee and colleagues127 more recently published a report on the effect of lumbar discography in precipitating accelerated degeneration in a matched cohort study. The 10-year follow-up showed that discs that had been punctured had a greater progression of disc degeneration—35% versus 14% in the control group. There were 55 new disc herniations in the discography group versus 22 in the control group. Carragee and colleagues127 concluded that despite using modern discography techniques with small-gauge needles, there is still an increased risk of disc degeneration, disc herniation, changes in disc and endplate signal, and loss of disc height when discography is performed.
Although discography has the potential to assist in diagnosing disc derangement, its reliance on the patient’s subjective pain response can also be problematic where secondary gain may be an issue. Psychosocial factors and chronic nonlumbar pain have also been shown to alter the diagnostic capabilities of the procedure. Finally, consideration of the consistent reports of the high false-positive rates and new findings of accelerated degeneration in discs that undergo discography make it difficult to recommend the procedure for the diagnosis of discogenic back pain. The validity of lumbar discography is very much in doubt, which is underscored by a more recent practice recommendation published by the American Pain Society. The society’s current recommendation is that provocative lumbar discography should not be used for making the diagnosis of a discogenic source of pain in the setting of nonradicular low back pain.128 The value of using discography to assess the levels to be operated on in patients with multilevel disc degeneration has not been adequately established scientifically.
Treatment
In 2009, the American Pain Society published five practice guidelines on the management of chronic nonradicular back pain based on the best available evidence for the various diagnostic and treatment modalities available. These recommendations are summarized in Table 45–2.128 These treatment modalities and others not mentioned in the treatment recommendations are discussed in detail along with brief summaries of the current supporting and opposing literature.
TABLE 45–2 Summary of Recommendations of American Pain Society Specifically in Regard to Management of Chronic Nonradicular Low Back Pain
From Chou R, Loeser JD, Owens DK, et al: Interventional therapies, surgery, and interdisciplinary rehabilitation for low back pain: An evidence-based clinical practice guideline from the American Pain Society. Spine (Phila Pa 1976) 34:1066-1077, 2009.
Nonoperative Treatment
Nonoperative treatment of lumbar disc disorders has been extensively discussed in the literature.141 Physical therapy, pharmacology, and spinal manipulations all have been supported by multiple studies of reasonable validity, but it is difficult to evaluate fully most of these studies because of a generalized lack of randomized control design, blind observers, compliance measures, and cointerventions. Additionally, very little of the literature on these nonoperative treatments is specific for the diagnosis of IDD or DDD but rather is generalized to chronic and acute low back pain, which may have multiple etiologies.
Bed Rest and Advice to Stay Active
The use of bed rest and its duration has long been debated in the literature. Treatment schedules ranging from 2 days to 6 weeks have been described.142–144 The currently accepted recommendation75 is limited bed rest for a maximum of 2 days because longer durations of bed rest may be detrimental to the patient’s general health while offering no benefit to the back pain. Allen and colleagues145 published a review of studies documenting bed rest as treatment for 15 different conditions and found that for patients with acute low back pain there was significant worsening of outcome measures. The updated Cochrane Review of bed rest for treatment of acute low back pain reported that there is high-quality evidence that advice to rest in bed is less effective than advice to stay active.146 Progressive return to activity and the initiation of a formal physical therapy or home exercise program are recommended after any initial short period of rest.
Verbunt and colleagues147 explored reasons why patients sometimes use prolonged bed rest in the setting of acute episodes of low back pain. Among the study population of 282 patients, 33% reported using bed rest, and 8% remained in bed for longer than 4 days. Behavioral factors, catastrophizing, and fear of injury were associated with use of prolonged bed rest. History of back pain and pain intensity were not associated with patient use of prolonged bed rest. Additionally, patients who used prolonged bed rest in the early phase of acute low back pain were more disabled after 1 year.
Patient education and advice to stay active is now the favored recommendation. A more recent Cochrane review148 of patient education and advice to stay active showed strong evidence that individual instructional sessions of 2.5 hours are more effective in returning patients to work than no intervention; however, in the setting of chronic back pain, patient education was less effective than more intensive interventions. Education sessions of shorter duration and written information were no more effective than no intervention. Another meta-analysis149 of 39 randomized controlled studies evaluated advice to stay active alone or as an adjunct to other interventions such as back school or specific exercise routines. Advice as an adjunct to a specific exercise program was the most common form of treatment implemented and the best supported of the treatments studied for chronic low back pain. Outcomes among patients with acute low back pain were generally poor, but advice to stay active alone was found to be the best recommendation.
Brox and colleagues150 published a systematic review of brief education in the clinical setting involving examination, information, reassurance, and advice to stay active. The authors found strong evidence that brief education was more effective for return to work but was no more effective than usual care for reduction of pain. There was limited evidence that dissemination of a back book or an Internet session was less effective than exercise. The authors concluded that a back book should not be distributed to patients as an alternative to another form of treatment.
Brace Wear and Other Orthotics
Another common conservative management technique involves the use of limited brace wear either with a recommendation to stay active or in conjunction with another form of nonoperative therapy. Calmels and colleagues,151 based on the results of a randomized clinical trial, recommended the limited use of a lumbar belt to improve functional status, pain, and medication use. Oleske and colleagues152 performed a randomized clinical trial of back supports and patient education in work-related back pain. These authors found no effect on patient self-report of recovery or lost work time between brace use and controls, but back supports were found to have some value in preventing recurrence of work-related back pain. A more recent Cochrane systematic review153 of brace treatment for low back pain failed, however, to find sufficient evidence to support the use of lumbar supports to treat low back pain. Moderate evidence was found that braces are no more effective than no treatment or physical training in preventing episodes of back pain.
Use of shoe insoles has been recommended in the past for treatment and prevention of nonspecific low back pain. A more recent Cochrane systematic review154 of six randomized controlled trials reported strong evidence that use of insoles does not prevent episodes of low back pain. There was limited evidence that insoles alleviated low back pain, but no conclusions or recommendations were made for use in the treatment of patients with low back pain.
Physical Therapy
There are multiple randomized controlled trials in the literature in support of many therapy routines or programs. Although a comprehensive review of all the various programs is not undertaken here, there have been some important updates in recent years worthy of discussion. More recent prospective randomized trials comparing physical therapy with fusion have emphasized the importance of a multidisciplinary approach with cognitive therapy, fear avoidance counseling, and intensive exercise programs.155–157 A systematic review150 found moderate evidence that fear avoidance training emphasizing exposure is more effective than graded activity increase for improvement of pain, disability, and fear avoidance.
Intensive interdisciplinary rehabilitation with emphasis on cognitive and behavioral intervention was one of the treatment recommendations made by the American Pain Society.128 Interdisciplinary rehabilitation was defined by the society as an integrated intervention with rehabilitation plus a psychological or social or occupational component. The American Pain Society recommended that interdisciplinary therapy should be offered as a viable alternative before proceeding to surgical treatment. Noninterdisciplinary or “traditional” physical therapy is also efficacious in this patient population, but no one specific program, method, or technique is significantly better than another.
Back schools are another commonly discussed therapy modality, and there is some indication that low-intensity back schools may have some efficacy. Heymans and colleagues,158 in a randomized controlled trial, found that patients who attended low-intensity back school experienced fewer sick leave days (68 days versus 75 days and 85 days) than usual care patients and patients who attended high-intensity back school. Functional status and kinesiophobia were improved at 3 months, but there was no difference in pain intensity and perception of recovery between the groups. In another randomized controlled trial, Kaapa and colleagues159 found no significant benefit of back school, however, compared with physical therapy combined with cognitive therapy at 6-month, 1-year, and 2-year follow-up.
A systematic review from the Cochrane Database in 2004160 concluded that there was moderate evidence suggesting that back schools in an occupational setting reduce pain and improve function and return-to-work status compared with other forms of therapy, such as exercises, manipulation, myofascial therapy, advice, placebo, and waiting list controls. Brox and colleagues150 published a separate systematic review of back schools and found moderate evidence that back schools were no better than waiting lists, no intervention, placebo, or general exercises for reduction of pain.
A European economic evaluation of a randomized controlled study161 of intensive group therapy found no significant cost difference between intensive group therapy and standard physiotherapy. There was also no difference in clinical effect between the groups at 1-year follow-up.162 To the authors’ knowledge, there are no economic studies to date of group therapy back schools in the United States. Although low-intensity back school and programs in a work setting may have benefit versus other forms of nonoperative treatment, most of the current literature shows that back schools offer little benefit over standard physical therapy and cognitive therapy.
Adjunctive Modalities
Another treatment option for low back pain includes adjunctive physical therapy modalities such as TENS, electrical muscle stimulation, ultrasound, and iontophoresis. Poitras and Brosseau163 reviewed randomized controlled data on the use of TENS and found that it may be useful for immediate short-term pain reduction but has little impact on patient perception of disability or on long-term pain control. A 2008 Cochrane systematic review of TENS versus placebo164 concluded that there is currently not enough evidence to support the routine use of TENS for management of chronic low back pain. Even less literature is available on the use of iontophoresis and ultrasound in the setting of discogenic back pain. The few randomized controlled trials that exist focus on ultrasound in conjunction with other physical therapy regimens. The efficacy of these modalities in isolation has not been determined.
Chiropractic and Complementary and Alternative Medicine Therapies
Several studies have reported the potential beneficial effects of chiropractic treatment for acute nonspecific low back pain.165–167 The role of chiropractic manipulations for the treatment of IDD or DDD of the lumbar spine has not been studied. Chiropractic manipulation is generally not considered effective in the treatment of chronic back pain resulting from disorders of the IVDs.168 A Cochrane systematic review169 failed to find evidence that spinal manipulative therapy was superior to general practitioner care, analgesics, physical therapy, exercises, or back school in the treatment of acute and chronic low back pain.
Eisenberg and colleagues170 published a randomized trial of usual care therapy versus the addition of the patient’s choice of alternative therapy—chiropractic, acupuncture, or therapeutic massage—in the treatment of acute low back pain. Outcomes based on the Roland-Morris scale and subjective assessment of symptoms showed no statistically significant improvement in patients who underwent alternative therapies compared with patients treated with the usual care of limited bed rest, nonsteroidal anti-inflammatory drugs (NSAIDs), education, and activity modification. The study did show, however, an increase in patient satisfaction with care, which came at an average $244 net increase in cost per patient.
Hurwitz and colleagues171 had similar findings in a randomized prospective study of 681 patients with chronic low back pain comparing chiropractic care with medical treatment with 18 months of follow-up. Although less than 20% of the patients overall experienced pain relief and differences in outcome measures were not clinically significant, patients in the chiropractic group were more likely to perceive that their symptoms had improved.
Other alternative medical therapies include acupuncture, prolotherapy, and massage. The Cochrane systematic review of acupuncture172 showed superiority to placebo sham therapy and a short-term benefit that did not extend beyond first follow-up when acupuncture was used in conjunction with other conventional therapies. A more recent systematic review by Ammendolia and colleagues173 questioned inconclusive evidence of the success of acupuncture versus sham acupuncture and called for further randomized trials to rule out the possibility of a placebo effect.
Prolotherapy is a technique that attempts to regenerate ligamentous and tendinous structures of the spine via injections of various irritant solutions. The treatment is usually performed in conjunction with spinal manipulation. There is no consensus on method, type of solution injected, or frequency of sessions. Most practitioners use various combinations of saline, dextrose, glycerin, phenol, and lidocaine. Many randomized trials and systematic reviews report conflicting efficacy of prolotherapy.174–176 No evidence has been reported for the efficacy of prolotherapy without cointerventions such as spinal manipulation or exercise.
Pharmacotherapy
Judicious use of narcotic pain medications, oral steroids, and NSAIDs in patients with severe, acute back pain can provide good pain relief. Most patients with painful degenerative discs can be treated adequately on an outpatient basis. NSAIDs and acetaminophen (Tylenol) are common over-the-counter medications used to treat back pain. A Cochrane review177 included 65 studies on NSAID use in low back pain. NSAIDs were found to be superior to placebo but had significantly more side effects. There is no documented difference between type of NSAID, including cyclooxygenase-2 inhibitors. Acetaminophen has an effect similar to NSAIDs but reduced risk of associated side effects when taken as directed and in general should be tried before NSAIDs. The Cochrane group concluded that NSAIDs are effective for short-term treatment of acute and chronic low back pain, but the size of the effect is small.
Opioid formulations are commonly used to treat back pain, but considering their widespread use there is a surprising paucity of high-quality randomized controlled data available on their efficacy. A Cochrane database meta-analysis178 of opioid use found only four studies, three of which focused on the use of tramadol. Pooled data found that tramadol, an atypical opioid, was more effective than placebo for pain relief and showed a slight improvement in functional scores. The only randomized controlled study of classic opioids179 was a comparison with naproxen. Opioids were found to be more effective for pain relief but were not more effective for improving function than naproxen. The Cochrane review authors concluded that the benefits of opioids for the treatment of chronic low back pain are questionable, and further well-designed randomized controlled studies need to be performed. Two subsequent systematic reviews180,181 of opioid use in the setting of chronic low back pain concluded that there is evidence to support the efficacy of opioids for short-term relief of pain only. There is little evidence for long-term opioid use, which is fraught with an incidence of aberrant consumptive behavior approaching 25%.
Use of opioid pain medication has many problems ranging from minor side effects such as constipation and nausea to severe complications including respiratory depression, altered mental status, and insidious issues with tolerance and addiction. Another more recent concern with opioid use is related to the combination of opioids and acetaminophen in commonly prescribed formulations.182 The maximum recommended daily dose of acetaminophen for adults and children older than 12 years is 4 g; thus concern arises when patients inadvertently take larger doses in the setting of prescription drug abuse. The potential to inadvertently take hepatotoxic or lethal doses can be a concern in the setting of prescription drug abuse. An advisory committee from the U.S. Food and Drug Administration (FDA)184 recommended the addition of a boxed warning on the risk of acetaminophen overdose and suggested elimination of combination opioid-acetaminophen formulations. Care should be exercised when prescribing opioid pain medications. They are best given for only a few days in the setting of severe acute back pain, and their use in patients with chronic back pain is not recommended.
Oral tapering courses of steroids have also been found useful for decreasing symptoms of low back pain, most specifically in patients with disc herniations.80,185 Steroids can cause gastrointestinal bleeding, and gastrointestinal protective agents should be used simultaneously with oral steroids to reduce the risk of this complication.
Muscle relaxants are another class of medication routinely used in the treatment of muscle spasm associated with low back pain. Their use should be limited to very short courses because of their addictive potential. The Cochrane review186 of muscle relaxants for the treatment of back pain included 30 trials evaluating the use of benzodiazepines, nonbenzodiazepines, and antispasmodic muscle relaxants. Strong evidence for the efficacy of muscle relaxants over placebo was reported for short-term pain relief in the setting of acute back pain. No difference between the various drugs and classes was discerned. More trials to determine the efficacy of muscle relaxants compared with other analgesics and NSAIDs were recommended.
The last class of medications commonly prescribed in the setting of back pain is antidepressants. Their use may be particularly beneficial in patients presenting with chronic low back pain in association with altered mental status, depression, anhedonia, sleep disturbances, agitation, and anorexia. Clinical studies187–189 supporting the use of tricyclic antidepressants (TCAs) have shown an improvement in mood and sleep patterns. Low doses of TCAs also affect membrane potentials of peripheral nerves, which may be a mechanism by which they produce pain reduction. A 2003 review190 of antidepressants in the treatment of chronic low back pain found that TCAs have a moderate effect on pain reduction in patients with no history of depression but reported conflicting evidence for improvement in functional outcomes. Physicians prescribing TCAs should be aware of potentially serious side effects involving orthostatic hypotension and cardiovascular perturbations. In a systematic review,191 selective serotonin reuptake inhibitors, another common class of antidepressants, failed to show efficacy in the treatment of chronic low back pain and should be reserved for emotional or psychiatric disturbances related to back pain and not used as a primary treatment for symptoms of back pain.
Keller and colleagues192 published a meta-analysis of nonsurgical management options for low back pain. These authors reported that behavioral therapy, exercise therapy, and NSAIDs had the largest effect of the modalities studied. Machado and colleagues193 published a separate large meta-analysis of placebo-controlled randomized trials of various forms of nonoperative treatment for nonspecific low back pain. Small improvements in complaints of pain were found in patients treated with traction, physical therapy, antidepressants, and NSAIDs; moderate improvements were found in patients treated with opioid analgesics, muscle relaxants, facet injections, and nerve blocks.
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


