Lesser Digital Deformities: Etiology, Procedural Selection, and Arthroplasty
Jeffrey S. Boberg
Jason J. Willis
Lesser digital deformities are perhaps one of the most common problems afflicting the foot and ankle. They primarily occur in the sagittal plane but often have an accompanying transverse or frontal plane component. The deformity occurs at the interphalangeal and metatarsophalangeal joints (MTPJs) and involves all related tendon and ligamentous structures, adding to the overall complexity of digital disorders (1). Furthermore, they may be static or dynamic, flexible or rigid, and congenital or acquired and may occur as an isolated deformity or in conjunction with other pathology (2).
Regardless of the etiology, nearly all digital deformities result from a loss of balance about the MTPJ. This causes varying degrees of dorsiflexion (extension) at the MTPJ with concurrent plantar protrusion of the metatarsal head secondary to retrograde toe pressure and plantarflexion (flexion) of the proximal interphalangeal joint (PIPJ). Consequently, these deformities are responsible for generating pain in the digit as well as the lesser MTPJs. The terms most commonly utilized to describe these lesser digital sagittal plane deformities include hammer toe and claw toe.
A hammer toe is a digital deformity occurring in the sagittal plane that involves dorsiflexion at the MTPJ, plantarflexion at the PIPJ, and dorsiflexion at the distal interphalangeal joint (DIPJ) (Fig. 13.1A).
A claw toe deformity displays dorsiflexion of the MTPJ and plantarflexion of the PIPJ as well as of the DIPJ. Though often associated with cavus foot deformity or neuromuscular disorders, such as Charcot-Marie-Tooth disease, it is seen in a flatfoot as well (Fig. 13.1B).
ANATOMY
A thorough understanding of the anatomical structures that encompass the lesser digits as well as the lesser MTPJs is paramount when taking into consideration the complex pathophysiology of and surgical treatments for lesser digital deformities.
The primary function of the extensor digitorum longus (EDL) is dorsiflexion of the foot during the swing phase of gait ending at heel contact (3). As the EDL courses across the ankle, it divides into four separate tendon slips, with one going to each of the lesser digits. Distally, the slips split and anatomically insert into the middle and distal phalanges. The extensor digitorum brevis (EDB) has only three tendon slips, one each for the second, third, and fourth digits. It inserts into the fibrous expansions of the long extensor tendon at the level of the MTPJ. These tendons form the extensor hood apparatus (4).
The extensor hood apparatus is an extremely important and unique anatomical structure. At the level of the MTPJ, its medial and lateral fibers unite plantarly with the capsule, deep transverse metatarsal ligament, and the flexor tendon sheath, thereby functionally inserting into the MTPJ. Consequently, the pull of the EDL and EDB tendons creates significant dorsiflexory power of the proximal phalanx at the MTPJ and minimal dorsiflexory power at the PIPJ or DIPJ (5,6). As the MTPJ undergoes dorsiflexion, the passive tension that develops on the flexor tendons produces plantarflexion at the PIPJ and DIPJ due to the limited extensor forces at these joints. This results in a claw toe deformity. Normally, toes do not claw during the swing phase due to the plantarflexory stabilization of the MTPJ by the lumbricales.
During the stance phase of gait, the flexor digitorum longus and brevis (FDL, FDB) aid in providing plantarflexory stability at the MTPJs to the lesser digits (7). The FDL divides into four separate tendon slips in the second layer of muscles in the plantar aspect of the foot. Each tendon slip then inserts into the distal phalanx of the lesser digits causing plantarflexion of the MTPJs and interphalangeal joints (IPJs) in the non-weight-bearing foot. The FDB also has four tendon slips that course to each of the corresponding lesser digits. The insertion of the FDB tendons is at the middle phalanx of the lesser digits, which causes plantarflexion at the MTPJ and PIPJ while non-weight-bearing.
However, during the stance phase of gait, the flexor tendons cannot plantarflex the toes due to the reactive force of the ground against the foot (3). The proximal pull of the FDL results in extension of the MTPJ and flexion of the IPJs as the toe buckles proximally. A claw toe deformity is the result. However, if the FDB is contracting as well, then the middle phalanx will be pulled against the ground resulting in passive extension of the DIPJ. Therefore, a hammer toe deformity is the result. Thus, the flexor tendons dorsiflex the proximal phalanx at the MTPJ and are responsible for both hammer toe as well as claw toe deformities.
However, this scenario does not occur normally. In the stance phase of the gait cycle, the interossei muscles, which insert into the plantar aspect of the base of the proximal phalanx and joint capsule, act to stabilize the proximal phalanx in
a plantarflexion. (4) Then, as the flexors begin to contract, the toe is unable to buckle proximally. Instead, they provide a stabilizing retrograde force on the metatarsals and a stable insertion for the flexor muscles.
a plantarflexion. (4) Then, as the flexors begin to contract, the toe is unable to buckle proximally. Instead, they provide a stabilizing retrograde force on the metatarsals and a stable insertion for the flexor muscles.
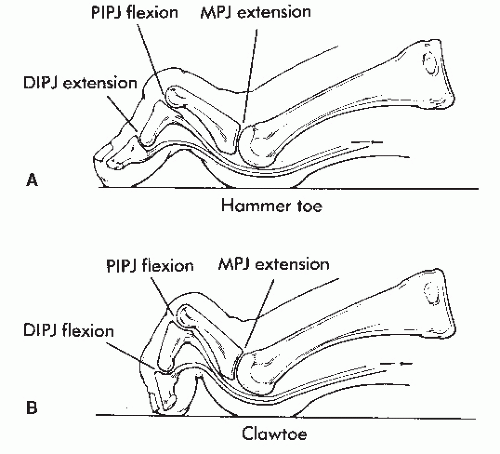 Figure 13.1 A: Hammered digit syndrome can lead to a classic hammer toe with dorsiflexion of the MTPJ, plantar flexion of the PIPJ, and hyperextension of the DIPJ. B: Claw toe results in dorsiflexion of the MTPJ and plantarflexion of both the PIPJ and DIPJ. |
ETIOLOGY
Although the exact cause of lesser digital deformities is multifactorial, biomechanical dysfunction is widely accepted to be the number one contributing factor to abnormal digital function. Ultimately, digital deformities are the result of loss of extrinsic and intrinsic muscle balance at the lesser MTPJ. The three major categories proposed to explain lesser MTPJ dynamic muscle imbalance include flexor stabilization, flexor substitution, and extensor substitution.
FLEXOR STABILIZATION
Perhaps the most common cause of digital deformities is pronation. The flexor tendons are supinators of the rearfoot. During pronation, they fire earlier and stay contracted longer in an attempt to stabilize the subtalar and midtarsal joints (8). Consequently, during the late-stance phase of gait, the FDL gains a mechanical advantage over the small interosseous muscles. Additionally, the intrinsic muscles, which are also supinators of the midfoot, may become fatigued in the pronated foot. However, they also may be weak for a variety of reasons, including peripheral neuropathy or tarsal tunnel.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


