peripheral nerve dysfunction proposes that a proximal nerve lesion along an axon, or the presence of concomitant metabolically induced peripheral neuropathy (as observed in diabetes mellitus), predisposes the nerve to injury at a more distal site along its course because of impaired axoplasmic flow (24,25,26,27 and 28). The double-crush syndrome may also predispose a patient to persistent symptoms despite appropriate nonsurgical or surgical management (29).
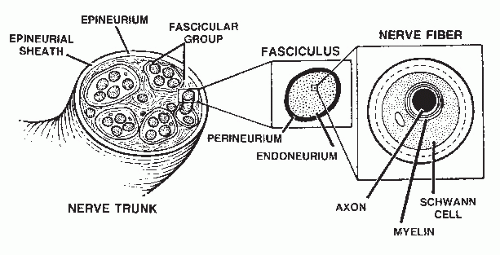 Figure 66.1 Peripheral nerve trunk functional and structural anatomy. |
nerve trunk laceration (30,31 and 32), blunt trauma, and compartment syndrome (33,34), fracture or dislocation, injection injury (4,35,36,37,38 and 39), and excessive traction with resultant intraneural hematoma, have been implicated (40,41 and 42). Nerve entrapment also has other iatrogenic causes including tourniquet compression (43,44), pressure related to positioning of the anesthetized patient during surgery, bandage or cast pressure (45), and surgical misadventure (43,46,47). Postoperative scarring secondary to normal wound healing may also create acquired neuropathy, even after proper incision planning, layer dissection, hemostasis, nerve manipulation, and wound closure. Finally, local infection and hematoma causing postinflammatory fibrosis may effect peripheral entrapment neuropathy.
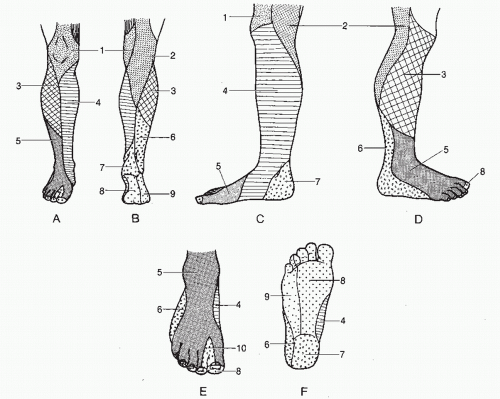 Figure 66.2 Peripheral nerve distribution. A: Anterior. B: Posterior. C: Medial. D: Lateral. E: Dorsal. F: Plantar. 1, medial and intermediate femoral cutaneous nerves (L2-3); 2, posterior femoral cutaneous nerve (S1-3); 3, lateral sural cutaneous nerve (L5, S1-2); 4, saphenous nerve (L3-4); 5, superficial peroneal nerve (L4-5, S1); 6, sural nerve (L5, S1-2); 7, medial calcaneal branch of tibial nerve (S1-2); 8, medial plantar nerve (L4-5); 9, lateral plantar nerve (S1-2); 10, deep peroneal nerve (L4-5). |
TABLE 66.1 Motor Innervation to the Leg and Foot | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
TABLE 66.2 Etiology of Localized Acquired Peripheral Neuropathy | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
advisable. Chronic compartment syndrome should also be considered in the differential diagnosis (53). Similarly, chronic tenosynovitis or a smoldering infection (abscess or osteomyelitis) may mimic the pain of localized nerve entrapment. Patients who may stand to gain secondarily from ongoing symptoms can also create diagnostic difficulties, and consultation may be helpful. Finally, peripheral polyneuropathy associated with metabolic, toxic, or infectious processes must also be included in the differential diagnosis.
founded on the Joule-Thompson principle (also known as the Kelvin effect), which states that gas under pressure escaping through a small orifice expands and rapidly cools. The endothermic rapid cooling process absorbs energy, in the form of heat, from the surrounding environment. When applied in a high-frequency cyclic fashion to tissues containing peripheral nerve, the resultant freeze-thaw cycle causes axonotmesis. Although contraindicated in the presence of infection, coagulopathy, and pain of unknown origin, cryoanalgesia has shown some efficacy for the treatment of interdigital neuroma, peripheral neuropathy, complex regional pain syndrome, as well as periungual warts and myxoid cysts (65,66,67 and 68).
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


