Chapter 54 Knee Bracing for Athletic Injuries
The use of braces in sports medicine has long been surrounded by debate. Does the benefit of a brace justify the potential discomfort and cost? This question must be evaluated in the context of brace use and the desired purpose. Different braces serve different functions. The American Academy of Orthopaedic Surgeons (AAOS) has defined three categories of knee braces24:
Rehabilitative Braces
Rehabilitative braces are designed to provide two functions, to protect a reconstructed/repaired ligament and allow early motion. However, the effectiveness of attaining and the clinical need for both of these purposes has been called into question by the contemporary literature. These braces can be off-the-shelf types with thigh and calf enclosures, hinges, hinge-brace arms, and straps that encircle the brace components (Fig. 54-1). The hinges can be unlocked to allow restricted range of motion and the braces are typically long to improve the lever arm and stability. Custom braces are available at an added cost. Rehabilitation braces are most prevalent in the context of anterior cruciate ligament (ACL) reconstruction and postoperative protocols.

Post–Anterior Cruciate Ligament Reconstruction Bracing
There are two main reasons to brace after ACL reconstruction—to protect the repair and avoid loss of extension. Various authors and surgeons have different opinions and protocols regarding bracing; some are based on experience and some based on the literature. This was clearly illustrated in a survey conducted by Marx and colleagues45 of 397 AAOS members with regard to ACL surgery. When surgeons were asked whether they braced patients postoperatively for 6 weeks, 40% responded “no” and 60% “yes.” Then, when asked if they recommended braces postoperatively for sports participation, 38% responded “no” and 62% “yes.” Despite the disparity in clinical opinion, there have been many prospective randomized clinical trials that evaluated the effect of a postoperative rehabilitation brace and a multitude of systematic reviews (Table 54-1).
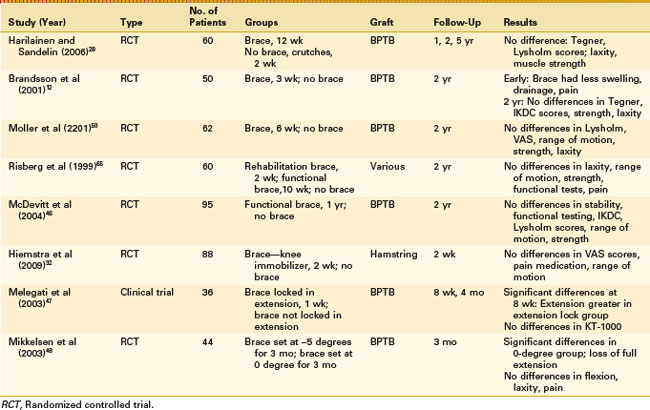
Harilainen and associates28,29 completed a randomized controlled study with a braced and an unbraced group. The braced group used a rehabilitation brace for 12 weeks postoperatively with a gradual increase in weight bearing, whereas the unbraced group was allowed immediate range of motion with the use of crutches for 2 weeks. The 1-, 2- and 5-year follow-up examinations revealed no differences in Tegner activity level, Lysholm knee score, laxity, or isokinetic thigh muscle strength.
Brandsson and coworkers12 also completed a prospective randomized clinical trial on the usefulness of postoperative rehabilitation braces in 50 patients. ACL reconstruction was completed with a bone-patellar tendon-bone (BPTB) autograft and patients were randomized to undergo rehabilitation for 3 weeks with or without a brace. Patients were followed for 2 years and, at the early follow-up visits rehabilitation with a brace resulted in fewer problems with swelling, a lower prevalence of hemarthrosis and wound drainage, and less pain throughout the early recovery period compared with rehabilitation without a brace. The 2-year follow-up revealed no differences between groups with regard to Tegner activity level, International Knee Documentation Committee (IKDC) rating, one-legged hop and isokinetic strength, or KT-1000 knee laxity.
Another randomized prospective clinical trial was completed by Moller and colleagues.50 They randomized 62 patients to 6 weeks of rehabilitation with or without a brace followed by a specific program for up to 6 months. In the early follow-up period, the braced group had slightly higher Tegner scores. At the 2-year follow-up, there were no differences in Lysholm, visual analogue scale (VAS) scores, range of motion, isokinetic strength, or laxity. The authors concluded that a postoperative knee brace provides no additional benefit. Risberg and associates,65 in a prospective randomized study, compared an unbraced population with a braced population that included the use of a postoperative rehabilitative knee brace for 2 weeks and then a functional brace for an additional 10 weeks. There were no differences between the groups except at the 3-month point. Despite greater thigh atrophy, the braced group showed an improved Cincinnati knee score. Otherwise, KT-1000 laxity, Cincinnati knee score, goniometry-measured range of motion testing, computed tomography (CT), thigh atrophy measurement, Cybex testing, functional knee tests, and VAS scores all were equal at 6 weeks, 3 and 6 months, and 1 and 2 years. It should also be noted that 24% of subjects in the brace group discontinued use prior to the 3-month time period.
A complete analysis of bracing after ACL reconstruction was done by McDevitt and coworkers.46 The authors prospectively randomized 95 patients over three institutions to brace wear for 1 year post–ACL reconstruction or no brace. All patients had a BPTB autograft and were held in extension for 3 weeks postoperatively and then followed up at 2 years. No significant differences were found between the groups in knee stability, functional testing with the single-leg hop test, IKDC scores, Lysholm scores, knee range of motion, or isokinetic strength testing. Two braced subjects had reinjuries and three nonbraced subjects had reinjuries.
The referenced studies are, for the most part, high-quality prospective randomized clinical trials that showed no quantifiable long-term benefit to postoperative bracing following ACL reconstruction with regard to activity level, subjective outcome, or knee laxity. However, some surgeons believe that a brace in the immediate postoperative period can provide the patient additional comfort. Hiemstra and colleagues32 looked at patients braced for the first 2 days, with a follow-up of 14 days. They found that bracing did not provide any additional pain relief in the acute period above and beyond that for nonimmobilized patients.
Bracing has also been proposed as a way to reduce any potential flexion contracture. Petsche and Hutchinson56 have identified loss of knee extension as the biggest problem after ACL reconstruction. Potential causes include surgical technique, graft placement, and postoperative contracture. Melegati and coworkers47 have evaluated the effect of bracing BPTB ACL reconstructions in extension for the first week. In this study, 36 subjects were allocated to an extension bracing group or a brace group with 0 to 90 degrees of motion for the first week. All patients were then allowed unrestricted motion after the first week. They found that at the 4- and 8-week postoperative points, there was a significant difference with regard to the two groups; the extension brace group had extension closer to that of the normal knee.
Mikkelsen and coworkers48 have evaluated the concept that the 0-degree setting on a brace does not represent true anatomic 0 degree and that this discrepancy affects the postoperative knee extension in patients who have undergone ACL reconstruction. Five subjects were placed in postoperative dressings and extension braces. Radiographs were taken to determine alignment. With the brace set at 0 degree, no subject had an anatomically straight leg (mean, +2.8 degrees) when compared with the −5-degree (mean, −2.5 degrees) and −10-degree (mean, −4.1 degrees) settings. Then, in a prospective study of ACL-reconstructed knees, they compared the differences between a hyperextension brace (−5 degrees) and an extension brace (0 degree) postoperatively. No significant differences were found between the groups in terms of knee flexion, sagittal knee laxity, or postoperative pain. However, only 2 of 22 patients in the hyperextension brace group had an extension loss more than 2 degrees, whereas 12 of 22 in the extension brace group had a loss more than 2 degrees.
Prophylactic Knee Braces
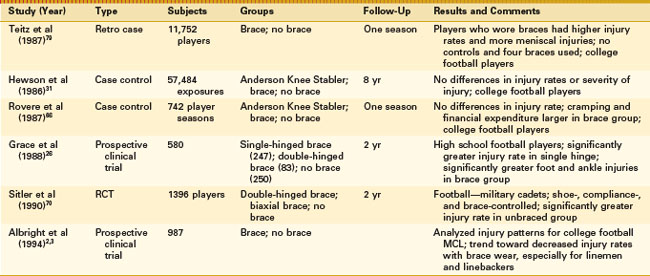
Many athletes at all levels of competition have experienced the agony and devastation of significant knee injuries. Thus, prevention and prophylactic knee bracing have received considerable attention over the last 50 years. This is perhaps most evident in football, in which there is a high percentage of knee injuries; 20% of professional football players never return from ACL reconstruction and those that do often do not reach their preinjury level of play.15 Anderson and colleagues4 were the first to report a prophylactic brace that was predominantly used to protect the MCL of professional football players; however, they also speculated that the brace provided increased anterior and posterior stability. They noted that there was no adverse impact on performance for the braced athlete. No controlled studies were completed at that time, yet bracing in professional and collegiate football experienced a rapid increase. In this section, we will review studies regarding the benefits and drawbacks of prophylactic bracing (Fig. 54-2; Table 54-2).

The reports by Anderson and associates4 led to a significant increase in brace use and studies to evaluate their efficacy in the early and mid-1980s. These early studies failed to demonstrate an appreciable benefit to brace wear, and some documented increased injuries and performance impairments, In 1985, the American Academy of Orthopaedic Surgeons stated that “Efforts need to be made to eliminate the unsubstantiated claims of currently available prophylactic braces and to curtail the inevitable misuse, unnecessary costs, and medical legal problems.”24 The American Orthopaedic Society of Sports Medicine and the Journal of Bone and Joint Surgery took a similar position.19 The American Academy of Pediatrics went a step further and recommended that prophylactic lateral knee bracing not be considered standard equipment for football players because of lack of efficacy and the potential for causing harm.44
Advantages and Disadvantages
No Benefit to Prophylactic Bracing
Teitz and coworkers79 used the members of Division I in the National Collegiate Athletic Association as its study population. They reviewed statistics from 71 colleges in 1984 and 61 colleges in 1985; 6307 players in 1984 and 5445 players in 1985 were analyzed. The player’s position, incidence of injury, type, mechanism, and severity of injury, playing surface, level of skill, and prior knee injury were considered contributing factors. The results showed that in 1984 and 1985, players who wore braces had a significantly higher injury rate than players who did not wear braces. Four different types of prophylactic knee braces were worn, and no attempt was made to differentiate between them with data analysis. The severity of injuries did not differ between the two groups. Player position, playing surface, mechanism of injury, or type of brace did not affect the rates of injury. Injuries were more common during contact and at every skill level in players who used braces. The incidence of ACL injury was similar in both groups, but braced players had more meniscal injuries. The severity of injury was assessed by measuring playing time lost and the need for surgery. Surgical rates were similar for both groups. Although the average playing time lost was less for players who used braces, the increased incidence of injury produced an overall time lost that was greater in players using braces. They concluded that prophylactic bracing would not prevent injuries and might actually be harmful.
Hewson and colleagues31 also completed a study of braced and unbraced football populations over an 8-year period (1977 to 1985). The nonbraced period was reviewed from 1977 to 1981. Following this, the Anderson Knee Stabler (Omni Life Science, Vista, Calif) was mandatory for all practices and games for players at greatest risk, including linemen, linebackers, and tight ends. In the mandatory brace group, 28,191 exposures occurred and, in the nonbraced group, 29,293 exposures. Information was analyzed by type of injury, severity of injury, player’s position, days lost from practice or games, and rate of knee injury/season/100 players at risk. Results showed that the number of knee injuries was similar for the braced and nonbraced groups and the type and severity of injury were similar in all categories. Rovere and associates66 also performed a 2-year study that included all players on the Wake Forest football team using the Anderson Knee Stabler prophylactically during practice and games. A 2-year nonbrace group control period was evaluated and compared with a subsequent braced group. The time and mechanism of injury, diagnosis, and treatment were noted. Brace use did not significantly alter the relative frequency of injuries by player or position, and it was noted that brace wearing was associated with cramping and added financial expenditures.
Grace and coworkers26 evaluated 580 high school football players over a 2-year period; 250 nonbraced athletes were matched according to size, weight, and position with 247 athletes wearing single-hinged braces and 83 athletes wearing double-hinged braces. The athletes who wore the prophylactic single-hinged braces had a significantly higher knee injury rate (P < .001), and the athletes wearing double-hinged braces had a greater number of injuries (no statistical significance). Foot and ankle injuries occurred three times more frequently in the braced group (P < 0.01). Different playing surfaces were used, and no documentation of prophylactic ankle taping was noted. The study results not only questioned the efficacy of prophylactic knee braces, but also called attention to the potential adverse effects on adjacent joints.
Potential Benefit to Prophylactic Bracing
The previous studies suggested no benefit and potential detrimental effects to prophylactic bracing. However, there have also been well-designed studies that purported a benefit for specific football positions. Initially, Garrick and Requa25 completed a review of available studies and noted two studies that suggested a benefit to bracing, those by Schriner67 and Taft and Funderburk.76 However, these studies were only presented at a conference and were never published. Furthermore, there were significant methodologic concerns with the study designs. Garrick and associates were unable to develop a conclusion with regard to brace use secondary to the lack of well-designed clinical trials.
Then, in 1990, Sitler and colleagues70 reported the results of a prospective, well-controlled research study regarding the effectiveness of a single, upright biaxial brace in a 2-year study of 1396 U.S. Military Academy cadets playing intramural tackle football as their mandatory competitive sport. The military population afforded control of the athletic shoe, athlete exposure, brace assignment and compliance, playing surface, and knee injury history. The study was completed over 2 years and at the beginning of each year the subject was assigned to a braced or unbraced group. The brace selected was the DonJoy Protective Knee Guard (DonJoy Braces, Coconut Creek, Fla) a double-hinged, single, upright, off-the-shelf brace applied to the leg with a brace-constrained, no-slip strap and neoprene thigh and calf straps. Individuals with ACL deficiencies, reconstructions, or repairs were excluded from the study. Knee injuries were defined as those that were severe enough to cause a missed practice or game. Nonsurgical evaluation was confirmed by at least two of the three orthopedic surgeons, and the injury was classified accordingly. There were 71 injuries and the overall knee injury rate was 2.46/1000 athlete exposures. The unbraced group had a significantly higher rate of injury than the braced group (3.40/1000 versus 1.50/1000 athlete exposures, respectively). There was also a trend noted toward decreased severity of injury in the braced group. This was a well-designed study with significant control, and the authors concluded that in this study population there is a benefit to prophylactic brace use.
Another well-done study was completed by the Big Ten Sports Medicine Committee. They conducted a 3-year prospective, multi-institutional analysis of medial collateral ligament (MCL) sprains in college football players.2,3 In their study, 987 previously uninjured participants were classified according to their frequency of wearing preventive knee braces. These subjects were then studied and the brace use patterns from 100 injuries were analyzed. The investigators evaluated the following factors:
Performance Impairments With Bracing
Styf and associates73 have studied the intramuscular pressures associated with functional braces. The intramuscular pressures of eight healthy athletes were recorded at rest and during and after exercise in the supine, sitting, and standing positions. There were three braces used in this study, a catheter was connected to an electromagnetic transducer, and intramuscular pressures were measured by an infusion technique. Pressures at rest increased significantly, in all positions, in braced study participants. Muscle relaxation pressure during exercise also increased significantly. Muscle relaxation pressures decreased to prebracing levels after removal of the brace or the distal straps. The results of this study suggested that external compression from a knee brace on leg muscles may induce premature muscle fatigue by reducing perfusion of the working muscle. More recently, Lundin and Styf43 have demonstrated that there is a direct correlation between thigh and tibial strap tensions and intramuscular values. There is also an inverse relationship with local blood perfusion.
Houston and Goemans35 evaluated the performance of braced and unbraced knees. Seven athletes with knee instability underwent four tests. Maximal torque output was measured during knee extension. Isometric torque was measured at a knee angle of 90 degrees at increasing velocities (30, 90, 180, and 300 degrees/second). Maximal unloaded angular velocity was measured during leg extension. Vertical velocity and power were determined using a short stair run. In addition, blood lactate concentration was measured 1 minute after a 15-minute ride on a bicycle ergometer. Maximal torque during isokinetic knee extension without braces was found to be significantly higher, and the differences between braced and unbraced study participants increased as velocity increased. Maximal unloaded knee extension velocity was 20% faster for unbraced individuals during the stair run. In addition to reporting impaired performance for braced study participants, an increased energy expenditure was observed; the blood lactate level increased 41% for braced participants.
This finding of ncreased energy expenditure was also supported by Zetterlund and associates84 who showed increased energy cost during treadmill running at a slow rate in 10 players. They found that oxygen consumption and heart rate significantly increase for braced athletes. However, energy consumption is not the only adverse effect reported with bracing. In the context of proprioception, Osternig and Robertson53 noted significant changes in joint position sense and electromyographic activity in six healthy volunteers when a brace was worn compared with when it was not worn.
Furthermore, Sforzo and colleagues68 showed that wearing a dual-hinged brace did not affect the performance of 25 male football players but did inhibit 10 women’s collegiate lacrosse team members. The testing protocol involved the use of a Cybex II lower extremity isokinetic dynamometer to measure peak quadriceps torque, rise time, and time to fatigue. A Monark cycle ergometer (HealthCare International, Langley, Wash) fitted with a Lafayette impulse counter (Lafayette Instrument Company, Lafayette, Ind) was then used to perform a 30-second maximal effort Wingate test of anaerobic power. Serum lactate accumulation was determined as the difference between postexercise and resting lactate levels. Although the overall performance score was significantly different, the differences were not significant for any one of the parameters.
On the other hand, Veldhuizen and associates81 did not support the theory that bracing weakens the knee. There was no significant difference between braced and unbraced healthy study participants performing testing for isokinetic muscle strength, a 60-m dash, a vertical jump height test, and treadmill running. Knutzen and coworkers37–39 have studied the knee joint kinematics of six braced individuals who ran a 12- to 13-km/hour pace. Knee stability and function were studied during maximum knee flexion in the swing phase, maximum knee flexion during the support phase, maximum external tibial rotation, and maximum internal tibial rotation. It was concluded in this and other reports that rotation and abduction-adduction decrease for braced individuals but does not affect performance.78
Greene and colleagues27 have demonstrated the effects of bracing on speed and agility, as well as the tendency of the brace to migrate, in 30 college football players. Players in full gear ran a 40-yard dash and performed a four-cone agility drill either wearing braces on both knees or wearing no brace, serving as matched controls. Brace migration and subjective measures were recorded after each trial. In the 40-yard dash, times did not significantly differ when using the AirArmor 1 (AirArmor Sports, Scottsdale, Ariz) and OMNI (OMNI Life Science, East Taunton, Mass) braces compared with nonbraced control times. Times with other braces were significantly slower, with the Breg (Breg, Vista, Calif) having the slowest time, followed by DonJoy, McDavid (McDavid USA,Woodridge, Ill) and AirArmor. The AirArmor 1 and McDavid braces showed significantly less superior-inferior migration in the 40-yard dash than the other braces. These findings indicate that specific braces have differential effects on the athlete and that fit is an important factor if migration is prevented.
Related posts:
 Cemented Total Knee Arthroplasty: The Gold Standard
Cemented Total Knee Arthroplasty: The Gold Standard
 Management of Extra-articular Deformity in Total Knee Arthroplasty With Navigation
Management of Extra-articular Deformity in Total Knee Arthroplasty With Navigation
 Patellar Instability
Patellar Instability
 Posterior Cruciate Ligament Reconstruction: Posterior Inlay Technique
Posterior Cruciate Ligament Reconstruction: Posterior Inlay Technique
 Perioperative Management of the Patient With Coronary Stents
Perioperative Management of the Patient With Coronary Stents
 Osteochondritis Dissecans
Osteochondritis Dissecans
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


