Chapter 119 Management of Extra-articular Deformity in Total Knee Arthroplasty With Navigation
Total knee arthroplasty is challenging in the presence of extra-articular deformity as the anatomic landmarks may be altered, traditional instrumentation may not be applicable, and ligament balance may be compromised. Additionally, with prior surgery, complicating hardware may be present. The ability to obtain a neutral mechanical axis is reported to be central to the long-term survival of total knee replacements.18,33,46,48 Extra-articular deformities, particularly of the femur, require placement of implants often at odds with the usual referenced bone landmarks to achieve a summed mechanical axis that is neutral and perpendicular to the ground at the joint line.11,32 The intramedullary canal used to assist with femoral component alignment instrumentation may be blocked by callus from a malunited fracture or filled with hardware. The diaphyseal canal additionally may be offset from the metaphysis, resulting in sagittal or coronal plane deformities.
These deformities are not new, and surgeons for the past 30 years have attempted to compensate for them with “best guess” measure and cut techniques, or with more sophisticated alignment systems.3,27,40 In recent years, imageless computer-assisted navigation systems have been developed that allow surgeons to accurately plan and execute bone resections in total knee arthroplasty based on a virtual mechanical axis.20,29,31 Numerous studies have shown the accuracy of this navigation technology, often reporting fewer outliers in sagittal and coronal plane alignment compared with manual conventional total knee instrumentation.2,9,10,16,30,43 Although debate over the utility of computer-assisted total knee for routine total knee surgery continues, focusing on the cost of the technology, surgical time investment, and the impact of error reduction on revision rates,34,42,49 one distinct area of benefit of computer-assisted navigation is help with the management of extra-articular deformity.
Extra-articular Deformities: Intra-articular versus Extra-articular Correction
Painful arthritis resulting in the need for total knee replacement may occur in association with extra-articular deformity of the femur or tibia. These deformities are typically the result of prior trauma with malunited fractures, but they can result from other conditions such as prior corrective osteotomies and metabolic conditions such as Blount’s, Paget’s, tertiary syphilis, or rickets.47 Often, the surgeon is forced to consider the possible presence of confounding hardware or a tortuous relationship of the diaphysis to the metaphysis, which may prevent the passage of intramedullary guide instrumentation or may complicate the placement of stems required for secondary stabilization of the implant (Fig. 119-1).

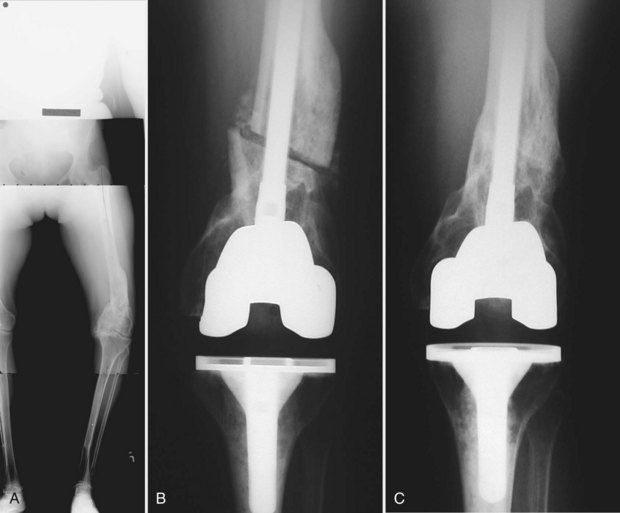
Strategies for management of extra-articular deformity include performing simultaneous corrective osteotomies at the time of total knee, with restoration of the diaphyseal-to-metaphyseal relationship,12,26,36,37 or correction of the deformity within the joint via corrective bone resections and subsequent soft tissue balancing to allow implant stability throughout the motion arc of the knee.47 The latter strategy, intra-articular correction with soft tissue balancing, is appealing because it is more efficient for the surgeon. It does not require creating an osteotomy that needs to be stabilized and heal. If, however, the degree of deformity would require a bone resection that extends to the epicondylar attachment of the collateral ligaments, then ligament integrity would be lost and constraining implants required.15,36 A more optimal strategy in this case is corrective osteotomy (Fig. 119-2A-C).
Some authors have argued that when deformities of the distal femur or proximal tibia exceed 15 degrees, because of the difficulty associated with simultaneous osteotomy and total knee replacement, corrective osteotomies should be performed and allowed to heal before total knee replacement surgery is performed.8,39 Wang and Wang47 reported on 15 patients with extra-articular deformities and arthritis treated with total knee replacement using intra-articular bone resections and soft tissue releases to achieve correction of mechanical alignment. These authors stressed the need for long-standing films to outline the deformity. Using line drawings, they determined whether the intra-articular bone resection necessary to correct the mechanical axis of the extremity would pass through the insertion of the collateral ligaments. Successful intra-articular correction was attained when coronal plane resections were less than 20 degrees and/or sagittal plane resections less than 25 degrees in the femur, or less than 30 degrees in coronal plane alignment of the tibia.
Wolff and colleagues50 stressed the relationship between degree of deformity and distance from the joint line. The closer the deformity apex is to the joint line, the greater is the impact on soft tissue releases necessary for balancing. Additionally, the authors noted that deformities of the tibia are easier to correct at the time of total joint replacement than those of the femur before the ligaments are balanced. Compensatory wedge resections necessary for axial correction of femoral deformities result in an asymmetrical extension space, with reduced impact on flexion balance. In contrast, correction of tibial deformity by compensatory wedge resection equally impacts flexion and extension spaces. Finally, varus deformities that cannot be completely balanced via intra-articular correction and soft tissue releases produce subtle lateral laxity that can be tolerated if the alignment is proper. In contrast, valgus deformity that cannot be completely balanced leads to medial laxity, which is much less well tolerated.50 These authors also concluded that in cases of extreme deformity wherein intra-articular resection is unlikely to yield satisfactory ligament balance, extra-articular osteotomy is indicated.
With coronal plane deformity of less than 20 degrees in the femur or less than 30 degrees in the tibia, intra-articular correction with total knee replacement is advantageous.26,28,50 One-stage correction of these deformities eliminates the risks associated with a possible second incision for the osteotomy, nonunion of the osteotomy, the need for osteotomy-stabilizing hardware, and potential delay in rehabilitation related to the osteotomy. For these reasons, when possible, one-stage intra-articular correction is preferable to performing a correction osteotomy.
Rationale for Total Knee Arthroplasty With Navigation in the Management of Extra-articular Deformities About the Knee
Optimal component alignment and positioning are critical to the long-term clinical success of total knee replacement.4,18,38 Failure to achieve optimal positioning of prosthetic knee implants can result in instability, increased pain, decreased range of motion, increased polyethylene wear, and implant loosening.5,14,17,22,41 The challenges of alignment and positioning in routine total knee replacement surgery and its association with compromised results when these goals are not achieved have led to the development of numerous systems and alignment guides designed to achieve neutral mechanical alignment and correct component rotation. These mechanical alignment systems include intramedullary and extramedullary guide rod systems that have inherent limitations in accuracy.24,45 Despite surgical experience and improved mechanical alignment devices, errors in postoperative alignment in total knee surgery still occur.44 Optical navigation systems—so-called imageless navigation—have become readily available in operating theaters around the world. Endorsement in multiple centers has allowed evaluation of the accuracy of the navigation systems, as well as comparative assessment versus manual instrumentation. Meta-analysis of available data suggests that these systems can deliver coronal and sagittal plane alignment that is superior to that attained with manual instrumentation.29
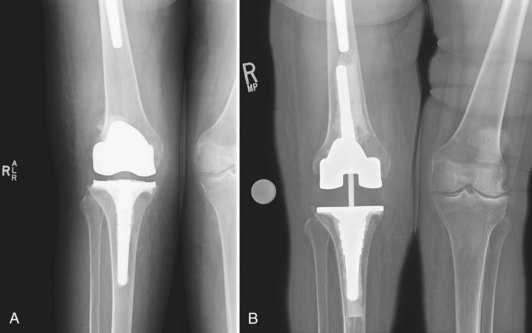
Although adoption of computer-assisted navigation for routine total knee replacement is hampered by the cost of the instrumentation, operative time requirements, and the paucity of literature linking its use to improved clinical outcomes,42 the value of this technology is uniquely leveraged when patients present with extra-articular deformity, retained hardware, or both (Fig. 119-3A and B). With computer-assisted navigation systems, the mechanical axis for the femur is determined irrespective of the bone between the femoral head and the central portion of the distal femur, and similarly between the central aspect of the tibia and the ankle. By virtually linking these points through imageless navigation, a mechanical axis is automatically calculated. In contrast, conventional instrumentation in the presence of obstructing hardware, a tortuous medullary canal, or complete occlusion of the medullary canal would require extramedullary alignment devices, osteotomy, or removal of the obstructing hardware. Digital mapping of the hip center of rotation, articular portions of the knee, and the ankle center offers the surgeon a clinical solution to the obstacles associated with extra-articular deformity.
In the relatively common presentation of patients with arthritis of the knee and retained hardware, the advantage of navigation is unique (Fig. 119-4A and B). Two scenarios may present. The first is hardware that for structural reasons may not be removed and that obstructs the use of conventional intramedullary instrumentation. In the second presentation, removal of the hardware is structurally feasible but requires greater surgical exposure, operative time, and risk to the patient. In these cases, navigation may represent a better option for the surgeon.

Surgical Technique: Navigation for Extra-articular Deformities Not Requiring Osteotomy
In cases with deformity primarily in the coronal plane, rotational alignment of the femoral component may be based on routine landmarks such as the transverse epicondylar axis. Unfortunately, in patients with extra-articular deformities, simple coronal deformity is uncommon, often corrupted by rotational deformities. The correct rotational position of the femoral implant is perpendicular to the resected surface of the proximal tibia when the knee is flexed and the ligaments are tensed. Consequently, after sufficient releases are obtained in extension to create a rectangular extension space, classic gap balancing techniques are utilized to obtain femoral rotation in flexion, while tensioning the collateral ligaments at 90 degrees of flexion and making anterior and posterior femoral cuts parallel to the tibial cut. Most navigation balancing algorithms assist the surgeon in referencing the femoral rotation to the resected tibial plane. Once femoral rotation is determined, femoral bone resections are completed (Fig. 119-5).

Related posts:
 Articular Cartilage: Biology, Biomechanics, and Healing Response
Advanced Technologies in Performing Total Knee Arthroplasty: Roundtable Discussion
In Vivo Mechanics and Vibration of the Knee Joint
Secondary, Spontaneous, and Postarthroscopy Osteonecrosis of the Knee: Diagnosis and Management
Advances in Mechanical Compression Devices
Articular Cartilage Injury and Adult OCD: Treatment Options and Decision Making
Articular Cartilage: Biology, Biomechanics, and Healing Response
Advanced Technologies in Performing Total Knee Arthroplasty: Roundtable Discussion
In Vivo Mechanics and Vibration of the Knee Joint
Secondary, Spontaneous, and Postarthroscopy Osteonecrosis of the Knee: Diagnosis and Management
Advances in Mechanical Compression Devices
Articular Cartilage Injury and Adult OCD: Treatment Options and Decision Making
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


