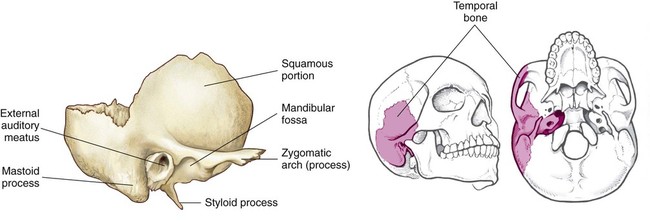
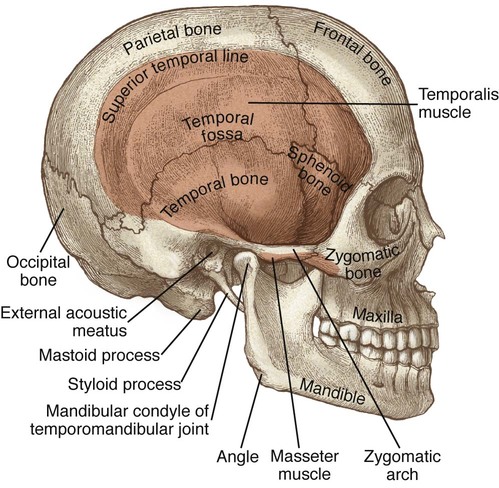
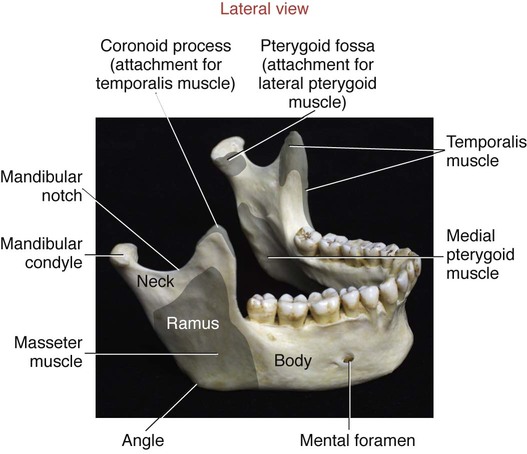
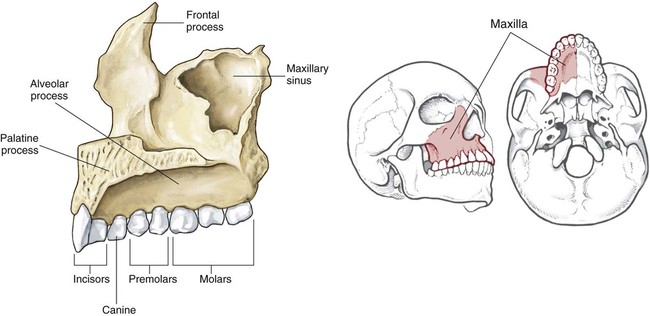
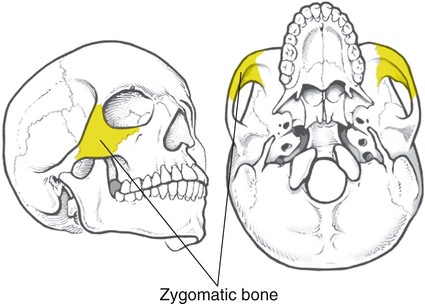
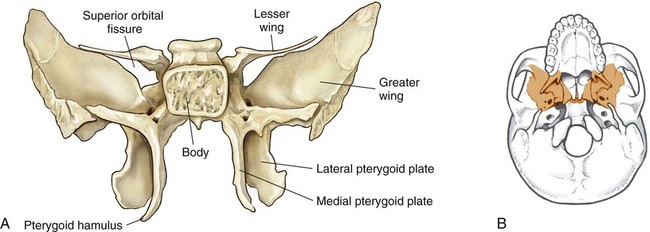
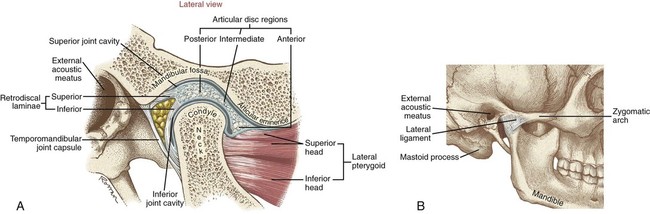
• Identify the bones and bony features relevant to the temporomandibular joint. • Describe the capsule and ligament that support the temporomandibular joint. • Identify the motions that occur at the temporomandibular joint. • Describe the muscular and joint interactions involved in opening the mouth. • Describe the muscular and joint interactions involved in closing the mouth. • Justify the actions of the primary muscles of the temporomandibular joint through knowledge of the muscles’ proximal and distal attachments. • Explain Boyle’s law in reference to the process of inspiration and expiration. • Compare the mechanics of quiet expiration with those of forced expiration. • Cite the primary muscles of inspiration. • Cite the primary muscles of forced expiration. • Describe the muscular interactions involved in forced inspiration. • Describe the muscular interactions involved in forced expiration. • Explain why accessory muscles of inspiration are often used by an individual with chronic obstructive pulmonary disease. The mandible, the temporal bone, the maxillae, and the zygomatic, sphenoid, and hyoid bones are related to the structure and function of the TMJ. Although this text highlights the most important features of these bones, additional anatomic features are included in Figure 13-1 for future reference. The mandible, or lower jaw bone, is the largest of the facial bones (Figure 13-2). This highly mobile bone is suspended from the cranium by muscles, ligaments, and the capsule of the TMJ. Many of the important bony landmarks are described as follows. The body is the horizontal portion of the mandible with sockets for the lower 16 adult teeth (see Figure 13-2). The ramus projects vertically from the body of the mandible. The angle of each mandible provides the attachment for the masseter and medial pterygoid muscles. The mandibular condyle is the convex portion of bone arising from the ramus. Each condyle articulates with the concave mandibular fossa of the temporal bone, forming the TMJ (see Figure 13-1). The coronoid process is the thin triangular projection of bone arising from the anterior aspect of the ramus. The mandibular notch extends between the coronoid process and the mandibular condyle (see Figure 13-2). The mandibular fossa of the temporal bone articulates with the mandibular condyle, forming the TMJ. The anterior aspect of the mandibular fossa is marked by the articular eminence (Figure 13-3). Just posterior to the mandibular fossa is the external auditory meatus: The external opening for the ear. The zygomatic process of the temporal bone projects anteriorly, forming the posterior half of the zygomatic arch (see Figure 13-3). The zygomatic arch is formed by the union of the zygomatic process of the temporal bone and the temporal process of the zygomatic bone (cheek bone) (see Figure 13-1). The zygomatic arch serves as the proximal attachment for the masseter muscle. The temporal fossa is a slightly depressed area on the side of the skull formed by the union of five different cranial bones (see Figure 13-1). The right and left maxillae unite to form a single maxilla, or upper jaw. The maxilla is firmly fused to adjacent bones of the face, including sphenoid, nasal, and zygomatic bones. The inferior aspects of the maxilla contain sockets for the upper teeth (Figure 13-4). The zygomatic bone forms the cheek region and lateral orbit of the eye (Figure 13-5). As has been mentioned, the temporal process of the zygomatic bone forms the anterior half of the zygomatic arch (see Figure 13-1). The sphenoid bone (Figure 13-6) is a single, deep bone that runs transversely across the cranium. The greater wings are located on either side of the cranium, just anterior to the temporal bone. Projecting inferiorly are the medial and lateral pterygoid plates (see Figure 13-6); the lateral plate provides proximal attachments for the medial and lateral pterygoid muscles. • Articular disc: The articular disc of the TMJ rests between the mandibular condyle and the mandibular fossa of the temporal bone (Figure 13-7, A). This prominent structure consists of dense fibrous connective tissue. The disc provides joint stability, reduces joint contact pressure, and helps safely guide the condyle across the rough articular eminence of the temporal bone. • Capsule: The TMJ is surrounded by a fibrous capsule. Laterally, the capsule thickens and is called the lateral ligament of the TMJ. The capsule and the lateral ligament provide stability to the TMJ during chewing motions (Figure 13-7, B). Protrusion, also referred to as protraction, describes the anterior translation of the mandible (Figure 13-8, A). As will be described, protrusion is an important component of opening the mouth. Retrusion, also called retraction, is the opposite of protrusion. This motion occurs as the mandible translates posteriorly—an important motion for closing the mouth (Figure 13-8, B). Depression of the mandible opens the mouth, whereas elevation closes the mouth (Figure 13-10). Both motions play a fundamental role in eating, yawning, and talking. The adult mouth can be opened an average of slightly more than 2 inches. This degree of opening is often gauged by the ability to fit three knuckles (proximal interphalangeal joints) into the mouth. As is illustrated in Figure 13-10, A, fully depressing the mandible—opening the mouth—requires extreme anterior translation (protrusion) of each mandibular condyle relative to its mandibular fossa. Normally, the articular disc translates anteriorly along with each mandibular condyle, helping to properly guide the motion (Figure 13-10, B). The disc is “reseated” into the joint as the mandible is elevated and retrudes (retracts) during closure of the mouth. In both opening and closing the mouth, the articular disc is essential in minimizing the contact stress between the mandibular condyle and the articular eminence of the temporal bone. The primary muscles of the TMJ are the masseter, temporalis, medial pterygoid, and lateral pterygoid. These muscles work together in a relatively complex fashion when the mouth is opening and closing; this will be explained in greater detail as the chapter progresses (see Figure 13-12). Bilateral: Bilateral:
Kinesiology of Mastication and Ventilation
Temporomandibular Joint
Osteology and Related Structures
Mandible
Temporal Bone
Maxillae
Zygomatic Bone
Sphenoid Bone
Supporting Structures
Kinematics
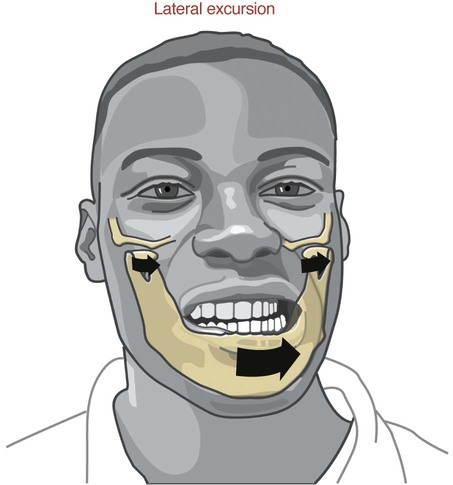
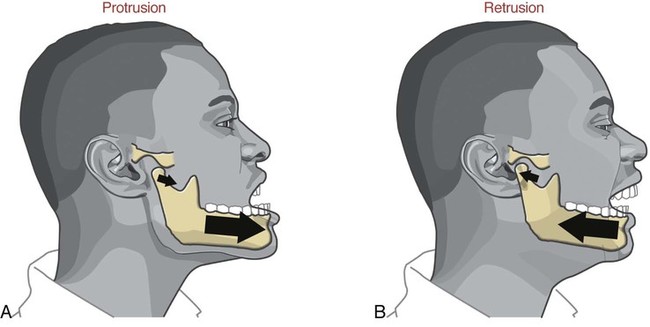
Protrusion and Retrusion
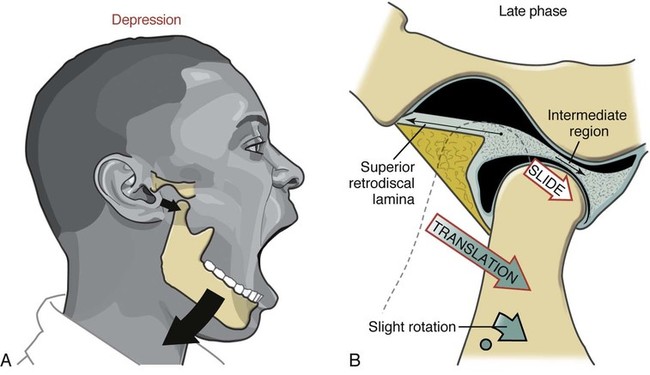
Depression and Elevation
Muscle and Joint Interaction
Muscles of the Temporomandibular Joint
Primary Muscles
Atlas
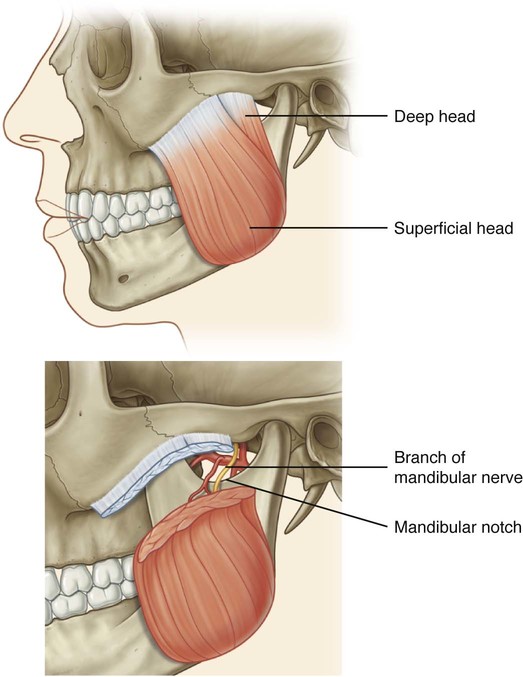
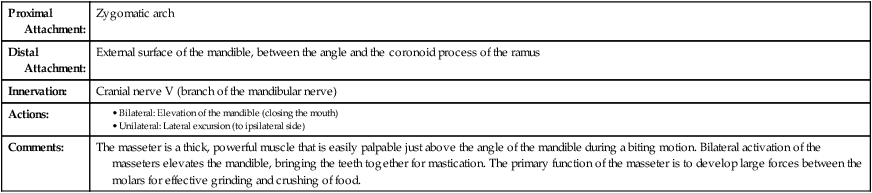
Masseter
Proximal Attachment:
Zygomatic arch
Distal Attachment:
External surface of the mandible, between the angle and the coronoid process of the ramus
Innervation:
Cranial nerve V (branch of the mandibular nerve)
Actions:
Comments:
The masseter is a thick, powerful muscle that is easily palpable just above the angle of the mandible during a biting motion. Bilateral activation of the masseters elevates the mandible, bringing the teeth together for mastication. The primary function of the masseter is to develop large forces between the molars for effective grinding and crushing of food.
Temporalis
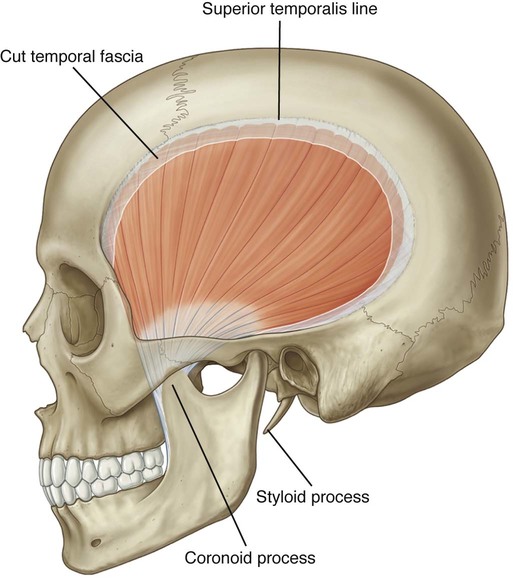
Proximal Attachment:
Temporal fossa
Distal Attachment:
Coronoid process and anterior edge of the ramus of the mandible
Innervation:
Cranial nerve V (branch of the mandibular nerve)
Actions:
Unilateral:
Comments:
The temporalis is a fan-shaped muscle that fills much of the concavity of the temporal fossa. The temporalis narrows into a broad tendon as it courses distally through a space between the zygomatic arch and the lateral side of the skull. This muscle contributes to both essential kinematic elements of closing the mouth: Elevation and retrusion of the mandible.
Medial Pterygoid
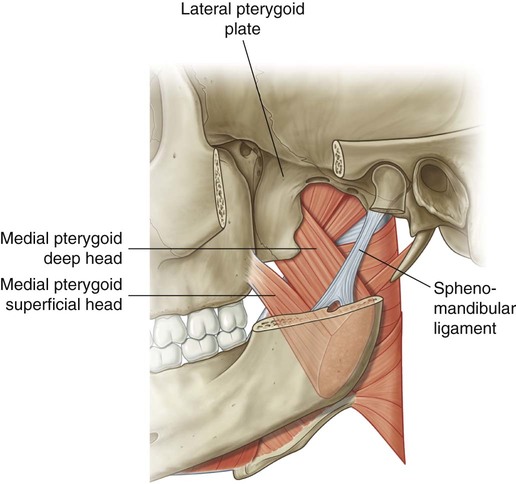
Proximal Attachment:
Medial surface of the lateral pterygoid plate
Distal Attachment:
Internal surface of the angle and ramus of the mandible
Innervation:
Cranial nerve V (branch of the mandibular nerve)
Actions:
Unilateral:
Comments:
The medial pterygoid and the masseter form a sling around the angle of the mandible. This sling affords a similar and secure line of pull for both muscles, which is especially useful for biting actions. Simultaneous bilateral contraction of these muscles can produce an average of almost 100 lb of biting force in the healthy adult. Related posts:
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


 Objectives
Objectives Key Terms
Key Terms