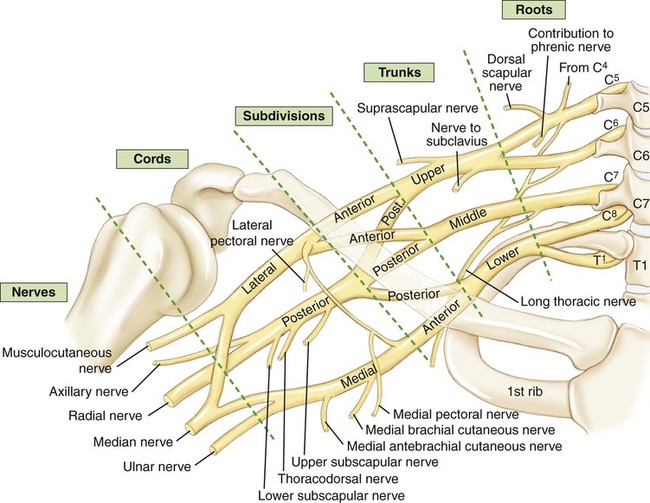
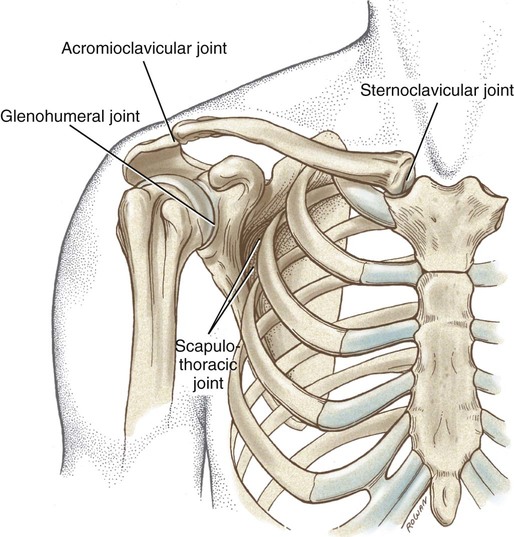
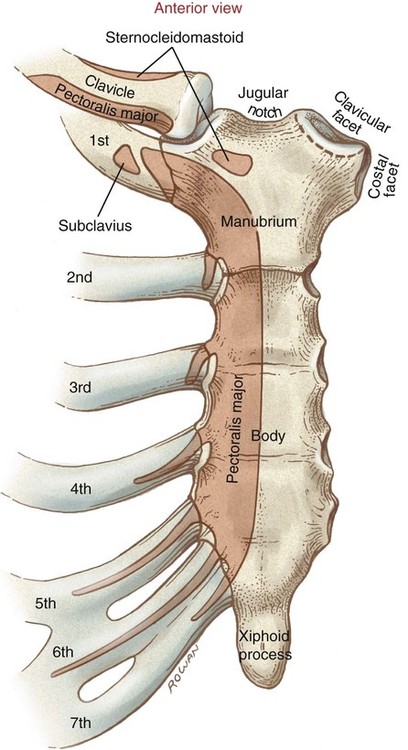
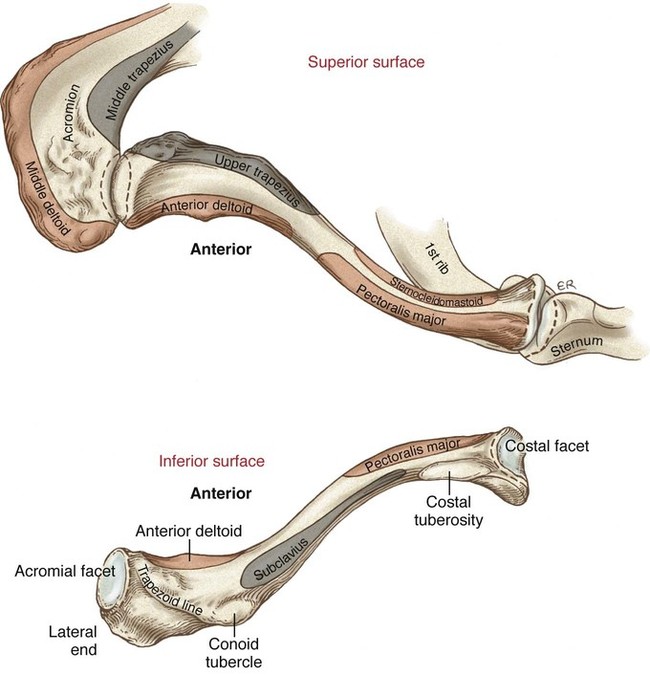
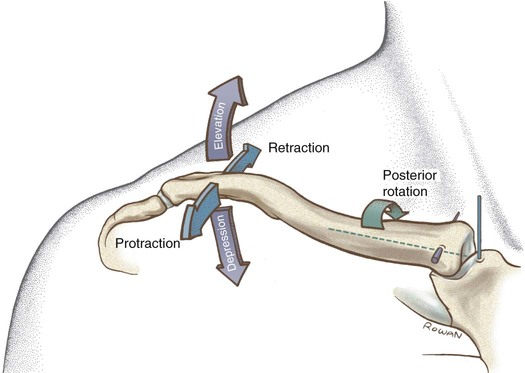
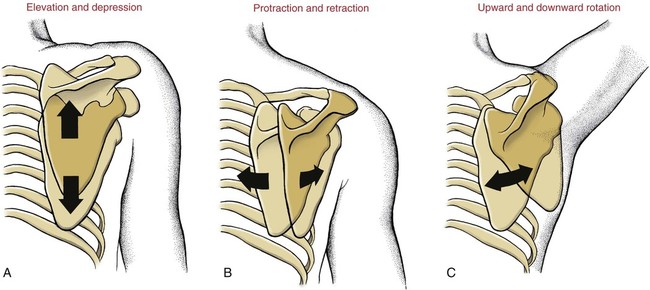
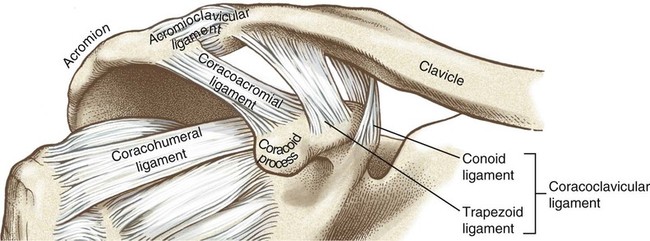
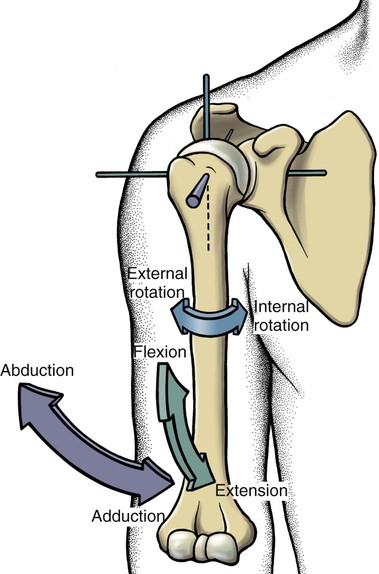
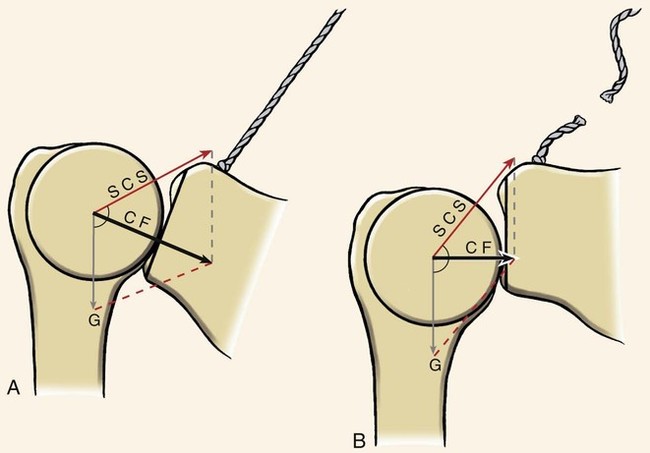
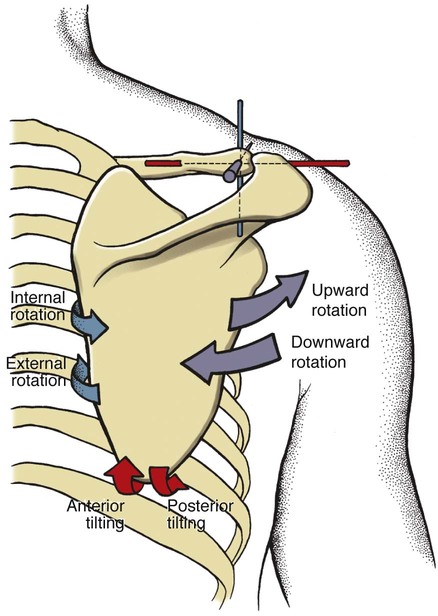
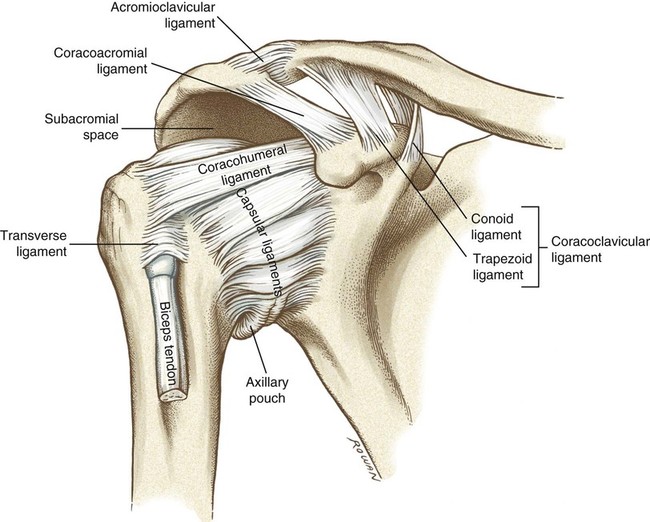
• Identify the bones and primary bony features relevant to the shoulder complex. • Describe the location and primary function of the ligaments that support the joints of the shoulder complex. • Cite the normal ranges of motion for shoulder flexion and extension, abduction and adduction, and internal and external rotation. • Describe the planes of motion and axes of rotation for the primary motions of the shoulder. • Cite the proximal and distal attachments, actions, and innervation of the muscles of the shoulder complex. • Describe the muscular interactions involved with active shoulder abduction. • Describe the scapulohumeral rhythm. • Explain the force-couple that occurs to produce upward rotation of the scapula. • Identify the primary muscles involved with dynamic stabilization of the glenohumeral joint. • Explain how the shoulder depressor muscles can be used to elevate the thorax. • Describe the interaction between the internal and external rotators of the shoulder during a throwing motion. Our study of the upper limb begins with the shoulder complex—a set of four articulations involving the sternum, clavicle, ribs, scapula, and humerus (Figure 4-1). This series of joints works together to provide large ranges of motion to the upper extremity in all three planes. Rarely does a single muscle act in isolation at the shoulder complex. Rather, muscles work in teams to produce highly coordinated movements that are expressed over multiple joints. The cooperative nature of the shoulder musculature increases the versatility, control, and range of active movements available to the upper extremity. Because of the nature of this functional relationship among the shoulder muscles, paralysis, weakness, or tightness of any single muscle can disrupt the natural kinematic sequencing of the entire shoulder complex. This chapter provides an overview of the kinesiology of the four joints of the shoulder complex and the important muscular synergies that support proper function of the shoulder (Figure 4-1). The sternum, often called the breast bone, is located at the midpoint of the anterior thorax and is composed of the manubrium, body, and xiphoid process (Figure 4-2). The manubrium is the most superior portion of the sternum that articulates with the clavicle—forming the sternoclavicular joint. The body or middle portion of the sternum serves as the anterior attachment for ribs 2 through 7. The inferior tip of the sternum is called the xiphoid process, meaning “sword shaped.” The clavicle, commonly called the collarbone, is an S-shaped bone that acts like a mechanical rod that links the scapula to the sternum (Figure 4-3). The flattened lateral portion—called the acromial end—articulates with the acromion of the scapula, forming the acromioclavicular joint. The medial or sternal end of the clavicle articulates with the manubrium of the sternum, forming the sternoclavicular joint. Commonly called the shoulder blade, the scapula is a highly mobile, triangular bone that rests on the posterior side of the thorax (Figure 4-4). The slightly concave anterior aspect of the bone is called the subscapular fossa, which allows the scapula to glide smoothly along the convex posterior rib cage. The glenoid fossa is the slightly concave, oval-shaped surface that accepts the head of the humerus, composing the glenohumeral joint. The superior and inferior glenoid tubercles border the superior and inferior aspects of the glenoid fossa and serve as proximal attachments for the long head of the biceps and the long head of the triceps, respectively. The scapular spine divides the posterior aspect of the scapula into the supraspinatous fossa (above) and the infraspinatous fossa (below). The acromion process is a wide, flattened projection of bone from the most superior-lateral aspect of the scapula. The acromion forms a functional “roof” over the humeral head to help protect the delicate structures within that area. The coracoid process is the finger-like projection of bone from the anterior surface of the scapula, palpable about 1 inch below the most concave portion of the distal clavicle. The coracoid process is the site of attachment for several muscles and ligaments of the shoulder complex. The medial and lateral borders of the scapula meet at the inferior angle, or tip, of the scapula. Clinically, the inferior angle is important in helping track scapular motion. The proximal humerus (Figure 4-5) is the point of attachment for a multitude of ligaments and muscles. The distal humerus is discussed in the next chapter. The sternoclavicular (SC) joint is created by the articulation of the medial aspect of the clavicle with the sternum (Figure 4-6). This joint provides the only direct bony attachment of the upper extremity to the axial skeleton—accordingly, the joint must be stable while also allowing extensive mobility. Figure 4-6 illustrates the supporting structures of the SC joint. • Sternoclavicular Ligament: Contains anterior and posterior fibers that firmly join the clavicle to the manubrium • Joint Capsule: Surrounds the entire SC joint; is reinforced by the anterior and posterior SC joint ligaments • Interclavicular Ligament: Spans the jugular notch, connecting the superior medial aspects of the clavicles • Costoclavicular Ligament: Firmly attaches the clavicle to the costal cartilage of the first rib and limits the extremes of all clavicular motion except depression • Articular Disc: Acts as a shock absorber between the clavicle and the sternum; helps improve joint congruency The SC joint structure is a saddle joint with concave and convex surfaces on each of the joint’s articular surfaces (Figure 4-7). This conformation allows the clavicle to move in all three planes. Motions include elevation and depression, protraction and retraction, and axial rotation (Figure 4-8). Motions at the scapulothoracic joint include elevation and depression, protraction and retraction, and upward and downward rotation (Figure 4-9). All motions are functionally linked to the motions that occur at the other three joints of the shoulder complex; these functional relationships are discussed in depth later. Scapular elevation involves the scapula sliding superiorly on the thorax (e.g., shrugging the shoulders). Depression occurs when the scapula slides inferiorly on the thorax (Figure 4-9, A; e.g., returning shrugged shoulders to a resting position; depressing the entire shoulder, as occurs when pushing up from a sitting position). Upward rotation occurs as the glenoid fossa of the scapula rotates upwardly, as a natural component of raising the arm overhead (Figure 4-9, C). Downward rotation occurs as the scapula returns from an upwardly rotated position to its resting position. This motion naturally occurs as an elevated upper extremity is lowered to one’s side. The acromioclavicular (AC) joint is considered a gliding or plane joint, created by the articulation between the lateral aspect of the clavicle and the acromion process of the scapula (Figure 4-10). In essence, this joint links the motion of the scapula (and attached humerus) to the lateral end of the clavicle. Because strong forces are frequently transferred across the AC joint, several important stabilizing structures are required to maintain its structural integrity. Figure 4-10 illustrates the supporting structures of the AC joint. • Acromioclavicular Ligament: Joins the clavicle to the acromion; helps to prevent dislocations of the scapula and links motion of the scapula to the clavicle • Coracoclavicular Ligament: Composed of the conoid and trapezoid ligaments. Together, these ligaments help suspend the scapula from the clavicle and prevent dislocation. • Coracoacromial Ligament: Attaches the coracoid process to the acromion process; one of the few ligaments of the body that attaches proximally and distally to the same bone. Along with the acromion, the coracoacromial ligament completes the coracoacromial arch—a functional “roof” that protects the head of the humerus. The AC joint allows motion in all three planes: Upward and downward rotation, rotation in the horizontal plane (internal and external rotation), and rotation in the sagittal plane (anterior and posterior tilting) (Figure 4-11). These relatively slight but important adjustment motions help to fine-tune the movements between the scapula and the humerus. Equally important, these motions allow the scapula to maintain firm contact with the posterior thorax. The glenohumeral (GH) joint is created by the articulation of the humeral head with the glenoid fossa of the scapula (Figure 4-12). Recall that the head of the humerus is a large, rounded hemisphere, and that the glenoid fossa is relatively flat. This bony conformation, in conjunction with the highly mobile scapula, allows for abundant motion in all three planes but does not promote a high degree of stability. It is interesting to note that the ligaments and capsule of the GH joint are relatively thin and provide only secondary stability to the joint. The primary stabilizing force of this joint is garnered from the surrounding musculature, particularly the rotator cuff muscles. • Rotator Cuff: A group of four muscles including the supraspinatus, infraspinatus, subscapularis, and teres minor. These muscles surround the humeral head and actively hold the humeral head against the glenoid fossa. These muscles are discussed at length in a subsequent section. • Capsular Ligaments: A thin fibrous capsule that includes the superior, middle, and inferior glenohumeral ligaments. This relatively loose capsule attaches between the rim of the glenoid fossa and the anatomic neck of the humerus (see Figure 4-12). • Coracohumeral Ligament: Attaches between the coracoid process and the anterior side of the greater tubercle. It helps limit the extremes of external rotation, flexion, and extension, as well as inferior displacement of the humeral head (see Figure 4-12). • Glenoid Labrum: A fibrocartilaginous ring that encircles the rim of the glenoid fossa. The labrum serves to deepen the socket of the GH joint, nearly doubling the functional depth of the glenoid fossa. The labrum also helps seal the joint, thereby contributing to stability by maintaining a suction effect between the humerus and the glenoid fossa. • Long Head of the Biceps: The proximal portion of the tendon wraps around the superior aspect of the humeral head, attaching to the superior glenoid tubercle. This tendon helps provide anterior stability because it acts as a partial extension of the glenoid labrum. The GH joint is a ball-and-socket joint that allows 3 degrees of freedom. The primary motions of this joint are abduction and adduction, flexion and extension, and internal and external rotation (Figure 4-13). Horizontal abduction and horizontal adduction are commonly used terms to describe special motions of the shoulder and are described in the following section. The arthrokinematics of abduction involves the convex head of the humerus rolling superiorly while simultaneously sliding inferiorly (Figure 4-14, A). Without an inferior slide, the upward roll of the humerus will result in the humeral head jamming into the acromion. This is known as impingement and often results in damage to the supraspinatus muscle or the subacromial bursa, which becomes pinched between these two bony structures (Figure 4-14, B). The arthrokinematics of GH joint adduction is the same as that of shoulder abduction but in the reverse direction. Internal and external rotation of the GH joint occurs in the horizontal plane about a vertical (longitudinal) axis of rotation (see Figure 4-13). Internal rotation results in the anterior surface of the humerus rotating medially, toward the midline, whereas external rotation results in the anterior surface of the humerus rotating laterally, away from the midline. During normal shoulder abduction (or flexion), a natural 2 : 1 ratio or rhythm exists between the GH joint and the scapulothoracic joint. This means that for every 2 degrees of GH abduction, the scapula must simultaneously upwardly rotate roughly 1 degree. For example, if the shoulder is abducted to 90 degrees, only about 60 degrees of that motion occurs from GH abduction; the additional 30 degrees or so is achieved through upward rotation of the scapula. The full 180 degrees of abduction normally attained at the shoulder is the summation of 120 degrees of GH joint abduction and 60 degrees of scapular upward rotation (Figure 4-15). Scapulothoracic motion is an integral part of nearly every shoulder movement. Furthermore, motion at the scapulothoracic joint is dependent on the combined movements of the AC and SC joints. The full 60 degrees of scapulothoracic upward rotation is achieved by combining about 30 degrees of clavicular elevation with 30 degrees of AC joint upward rotation (see Figure 4-15). Box 4-1 summarizes the interactions among the joints during common shoulder motions. Two Ways to Help Prevent Shoulder Impingement Even with the humerus in full external rotation, complete abduction of the shoulder may result in impingement if performed in the true frontal plane (Figure 4-16, A). Therapists often request that their patients perform shoulder exercises in the scapular plane as a way to prevent recurring impingement. The scapular plane is about 35 degrees anterior to the frontal plane (Figure 4-16, B). Shoulder abduction in the scapular plane, often referred to as scaption, positions the greater tuberosity of the humerus under the highest point of the acromion and helps to prevent bony impingement, regardless of the amount of rotation of the glenohumeral joint. This can be verified by performing abduction in the scapular plane, with the upper extremity positioned in internal rotation, in neutral, or in external rotation. Static Passive Locking Mechanism of the Glenohumeral Joint Ideal posture of the scapula positions the glenoid fossa so that it is tilted about 5 degrees upward (Figure 4-17, A). This position not only improves the contact of the articulation but allows the surrounding soft tissues to help support this joint. The superior capsular ligaments provide an upward force vector to counteract the downward force of gravity. When these forces are combined, the resultant vector is a compressive force directed through the middle of the glenoid fossa, enhancing the static stability of the GH joint. As illustrated in Figure 4-17, B, when the scapula becomes downwardly rotated, as commonly occurs after a stroke involving weakness or paralysis of the trapezius muscles, the static locking mechanism becomes ineffective. Not only does the humeral head lose its ledge on which to rest, but the direction of the upward forces created by the superior capsular ligaments is changed, reducing the overall potential of these structures to produce a passive compression force (CF). The entire upper extremity receives innervation primarily through the brachial plexus (Figure 4-18). The brachial plexus is formed by a network of nerve roots from the spinal nerves C5-T1. Nerve roots C5 and C6 form the upper trunk, C7 forms the middle trunk, and C8 and T1 form the lower trunk. The trunks travel a short distance before forming the anterior or posterior division. The divisions then reorganize into lateral, medial, and posterior cords, named by their position relative to the axillary artery. The cords eventually branch into nerves that primarily innervate muscles of the upper extremity.
Structure and Function of the Shoulder Complex
Osteology
Sternum
Clavicle
Scapula
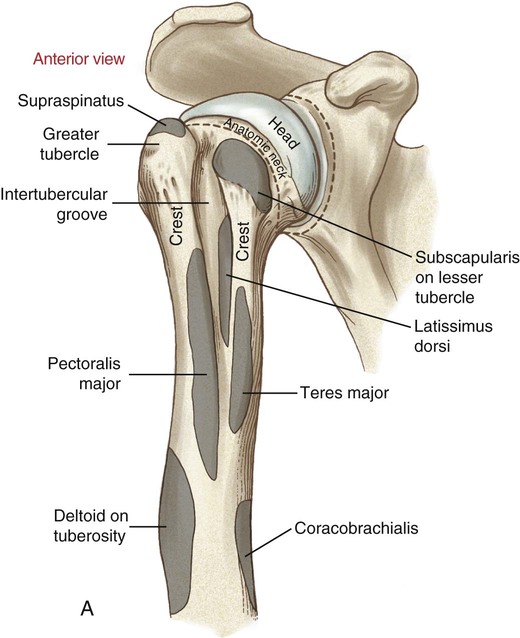
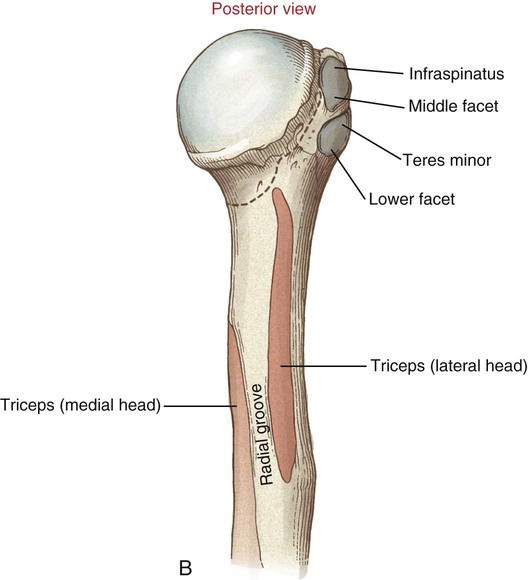
Proximal-to-Mid Humerus
Arthrology
Sternoclavicular Joint
General Features
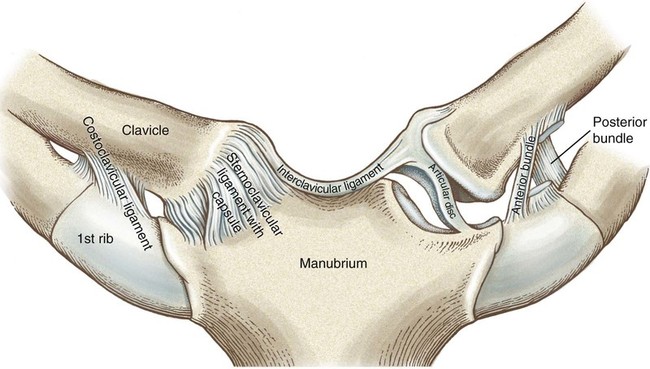
Supporting Structures of the Sternoclavicular Joint
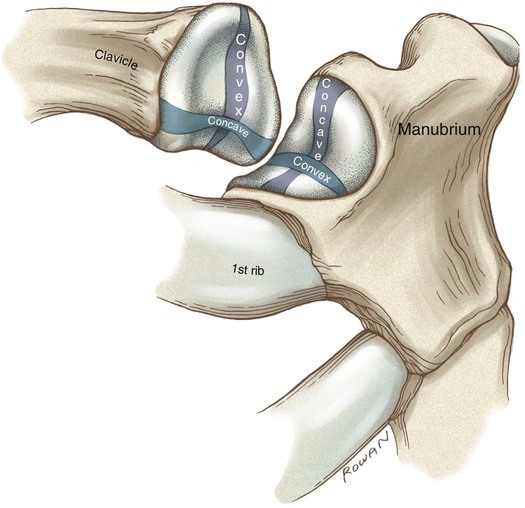
Kinematics
Scapulothoracic Joint
General Features
Kinematics
Elevation and Depression
Upward and Downward Rotation
Acromioclavicular Joint
General Features
Supporting Structures of the Acromioclavicular Joint
Kinematics
Glenohumeral Joint
General Features
Supporting Structures of the Glenohumeral Joint
Kinematics
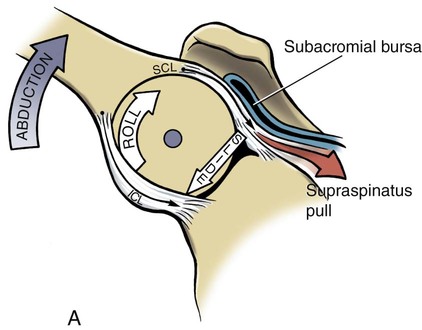
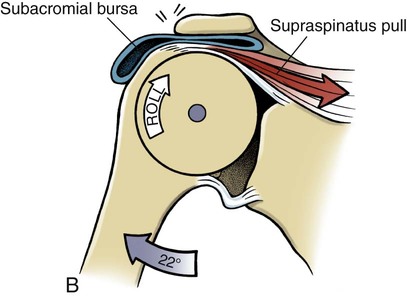
Abduction and Adduction
Internal and External Rotation
Interaction Among the Joints of the Shoulder Complex
Scapulohumeral Rhythm
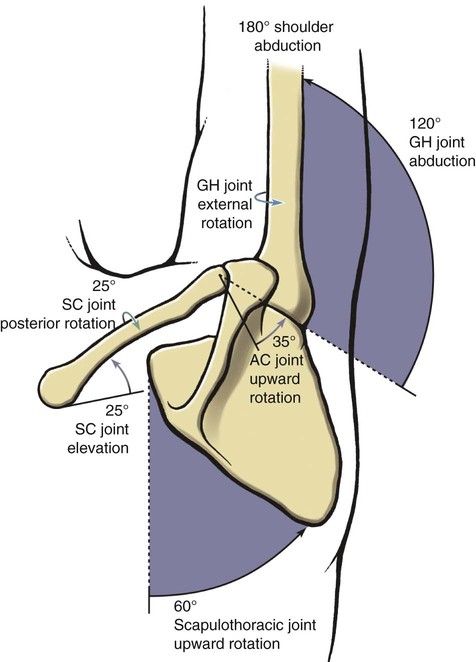
Acromioclavicular and Sternoclavicular Joint Interaction Within the Scapulohumeral Rhythm
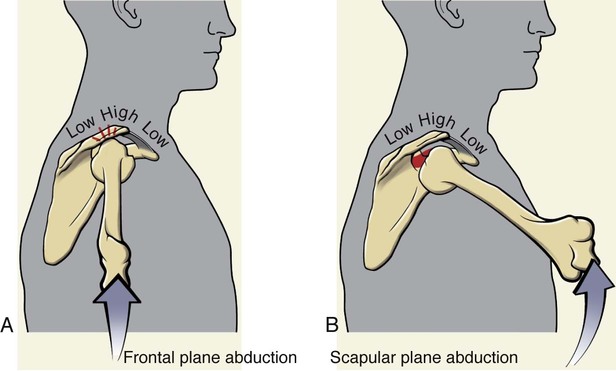
 Clinical insight
Clinical insight
 Consider this…
Consider this…
Muscle and Joint Interaction
Innervation of the Shoulder Complex
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Structure and Function of the Shoulder Complex
 Objectives
Objectives Key Terms
Key Terms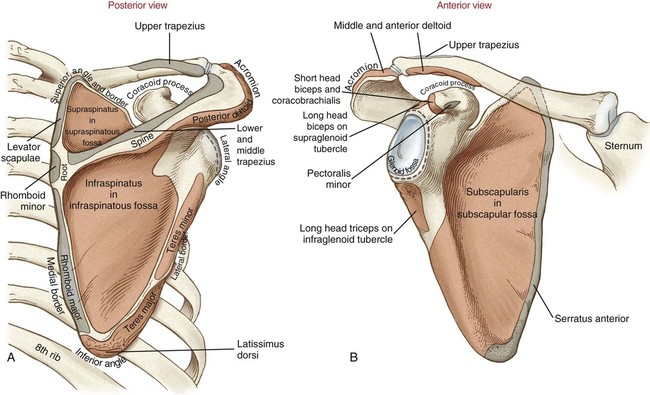
 Consider this…
Consider this… Box 4-1
Box 4-1