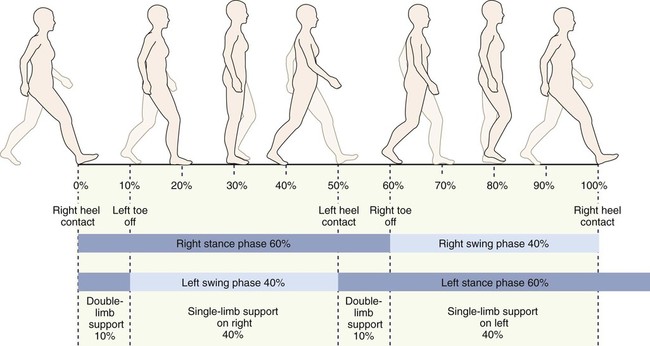
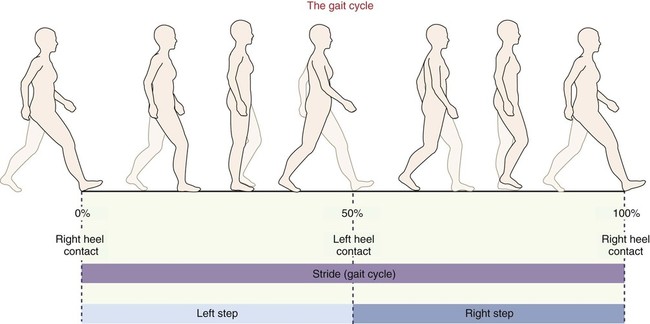
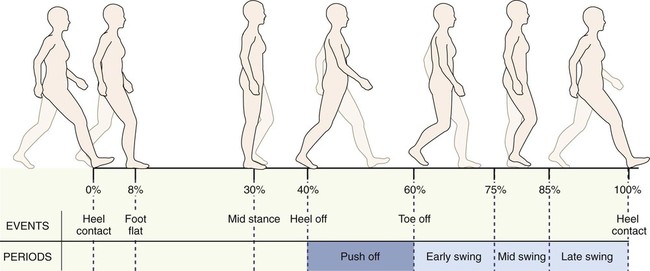
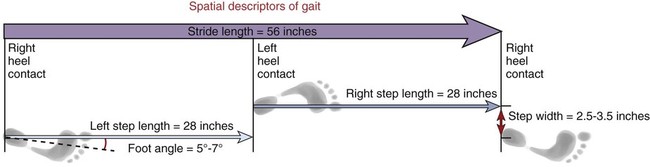
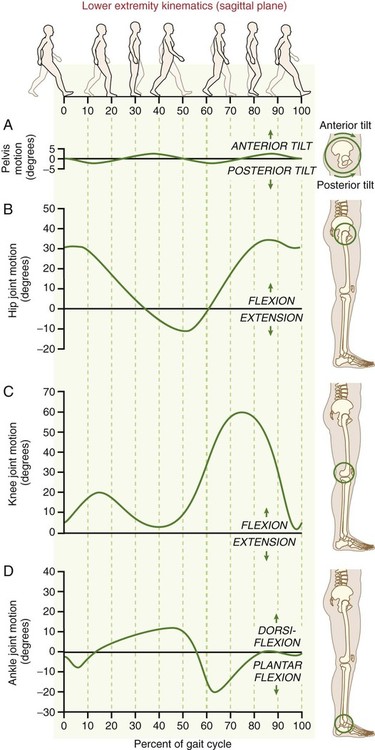
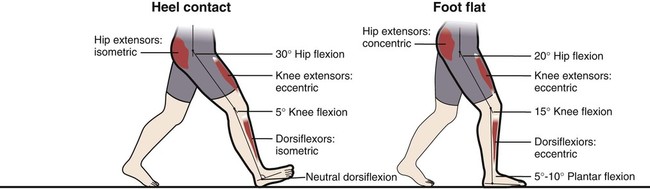
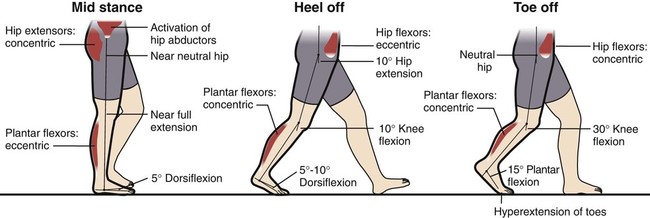
• Describe the primary events of the gait cycle. • Define the common terms used to describe human gait. • Describe the muscular and joint interactions that occur during heel contact. • Describe the muscular and joint interactions that occur during foot flat. • Describe the muscular and joint interactions that occur during mid stance. • Describe the muscular and joint interactions that occur during heel off and toe off. • Describe the muscular and joint interactions that occur during early, mid, and terminal swing. • Define the common terms that are used to describe human gait. • Explain the role of the hip abductor muscles during the stance phase of gait. • Describe common gait deviations, including impairments that may cause the deviations. The study of gait uses a special set of terminology. Much of this terminology relates to the events that occur within the gait cycle. The gait cycle describes all the important events that occur between two successive heel contacts of the same limb (Figure 12-1). Because of the dynamic and continuous nature of walking, the gait cycle is described as occurring between 0% and 100% (Figure 12-2). As is shown in Figure 12-2, during the first 60% of the gait cycle, the foot remains in contact with the ground; this is known as the stance phase. The stance phase is subdivided into five events: • Heel contact: The instant the lower limb contacts the ground (0% of the gait cycle). • Foot flat: The period that the entire plantar aspect of the foot is on the ground (8% of the gait cycle). • Mid stance: The point where the body weight passes directly over the supporting lower extremity (30% of the gait cycle); coincides with a vertically oriented lower leg. • Heel off: The instant the heel leaves the ground (40% of the gait cycle). • Toe off: The instant the toe leaves the ground (60% of the gait cycle). In the last 40% of the gait cycle, the limb is off the ground in the swing phase. The swing phase is subdivided into three events (see Figure 12-2): • Early swing: The period from toe off to mid swing (60% to 75% of the gait cycle). • Mid swing: The period when the foot of the swing leg passes next to the foot of the stance leg (75% to 85% of the gait cycle). This corresponds to the mid stance phase of the opposite lower extremity. • Terminal swing: The period ranging from mid swing until heel contact (85% to 100% of the gait cycle). In addition to the terms that define the events within the gait cycle, the following terms and concepts are useful in the study of gait (Figure 12-3). Note that the following terms are based on a healthy adult, walking at an average speed. Walking faster or slower causes significant changes in these variables. • Stride: The events that take place between successive heel contacts of the same foot. All events within one stride occur within a gait cycle. • Step: The events that occur between successive heel contacts of opposite feet, for example, between left and right heel contacts. • Step length: The distance traveled in one step, which, on average, is about 28 inches in the healthy adult. • Stride length: The distance traveled in one stride (between two consecutive heel contacts of the same foot); typically 56 inches in the healthy adult. • Step width: The distance between the heel centers of two consecutive foot contacts. Normally, this distance is about 3 inches in the healthy adult. • Cadence: The number of steps taken per minute; also called step rate. The average cadence for a healthy adult is 110 steps per minute. • Walking velocity: The speed at which an individual walks. Normal walking velocity is about 3 miles per hour; walking velocity increases by increases in cadence or step length, or both. Although normal gait involves movement in all three planes, the upcoming discussion focuses on the sagittal plane movements of the pelvis, hip, knee, and ankle (talocrural) joints. Figure 12-4 shows the sagittal plane range of motion of the hip, knee, and ankle throughout the full gait cycle. This figure should be referred to throughout the following sections. Bear in mind that the discussions below refer to the kinesiology of a typical adult walking on level surfaces at an average speed. Compensations Used to Mask Hip Joint Tightness During Walking Individuals with a stiff or painful hip often have limited amounts of hip flexion or extension, but nevertheless many can ambulate with relatively normal stride lengths. How is this possible? Often the person will learn to compensate for the loss of hip motion by producing an exaggerated pelvic motion in the sagittal plane. For example, at heel contact, the hip is normally flexed to about 30 degrees while the pelvis remains in a relatively neutral position (Figure 12-4, A and B). A person with limited hip flexion can effectively maintain normal stride length (and therefore normal heel contact location on the ground) by excessively posteriorly tilting the pelvis. Adding the posterior pelvic tilt to available hip flexion increases the overall “functional reach” at the hip and pelvis, thereby preserving stride length. Conversely, if hip extension is limited, the individual may compensate by excessively anteriorly tilting the pelvis at the end of stance phase to increase the amount of “functional extension” at the hip and pelvis. Because the motions of the lumbar spine and pelvis are mechanically linked, these repetitive and exaggerated motions of the pelvis may cause excessive stress and damage to structures of the lumbar spine. Therefore, it is not only important for clinicians to be able to identify these compensations, but also to employ treatment strategies that selectively elongate the tight structures of the hip while improving the strength and control of the structures that stabilize the pelvis. Heel contact marks the beginning of the gait cycle as the heel contacts or strikes the ground (heel contact is often referred to as heel strike) (Figure 12-5, left). At this point in the gait cycle, the center of gravity of the body is at its lowest point. At heel contact, the ankle is held in neutral dorsiflexion through isometric activation of the dorsiflexor muscles. As the ankle transitions toward foot flat (the next event), the dorsiflexor muscles (e.g., tibialis anterior) are eccentrically active to lower the ankle into plantar flexion. The hip is in about 30 degrees of flexion. As weight bearing continues, the hip extensor muscles are isometrically active to prevent the trunk from “jackknifing” forward (see Figure 12-5, left). Foot flat is defined as the point at which the entire plantar surface of the foot is in contact with the ground (see Figure 12-5). This event is often described as the loading-response phase. During this time, the muscles and joints of the lower limb assist with shock absorption, as the lower extremity continues to accept increasing amounts of body weight. Immediately after foot flat, the opposite limb begins to leave the ground and enters its early swing phase. The knee continues to flex to about 15 degrees, acting as a shock-absorbing spring. The knee extensor muscles continue to be active eccentrically, as the hip extensor muscles shift from isometric to slight concentric activation, guiding the hip toward extension (Figure 12-5, right). Mid stance occurs as the lower leg approaches the vertical position (Figure 12-6, left). The leg is in single-limb support, as the other limb is freely swinging forward. The hip and the knee are in near extension, as the ankle continues to move into greater dorsiflexion. During mid stance, the stance leg is in single-limb support as the other leg is freely swinging toward the next step. The hip abductor muscles (e.g., gluteus medius) of the stance leg therefore are active to stabilize the hip in the frontal plane, preventing the opposite side of the pelvis from dropping excessively (see Figure 12-6, left). The events of heel off occur just after mid stance as the lower leg and ankle begin “pushing off” to propel the body upward and forward (Figure 12-6, middle). As the name implies, the heel-off phase begins as the heel breaks contact with the ground. At heel off, the extended knee prepares to flex, often driven by a short burst of activity from the hamstring muscles. The hip continues to extend to about 10 degrees of extension. Eccentric activation of the hip flexors, in particular the iliopsoas, helps to control the rate and amount of hip extension (see Figure 12-6, middle). Tight ligaments of the hip or tight hip flexor muscles will reduce the amount of hip extension at this point in the gait cycle, thereby reducing stride length. Toe off is the final event of the stance phase of gait (Figure 12-6, right). The events that occur during this period are designed to complete push-off and begin the early swing phase. As the name implies, toe off coincides with the toes leaving the ground. The contralateral leg begins its foot flat phase and begins to accept a greater portion of body weight. At toe off, the knee is flexed 30 degrees. In the very end of toe-off phase, the slightly extended hip starts to flex as the result of concentric activation of the hip flexor muscles (see Figure 12-6). Transition Between Single- and Double-Limb Support: The “Balancing Act” of Walking During double-limb support, both legs are in contact with the ground. This period occurs during the first and last 10% of the stance phase (Figure 12-7). During these periods of walking, the body’s center of gravity is at its lowest point. The lower center of gravity combined with bilateral support affords maximum stability to the body as a whole—useful as weight is transferred between limbs.
Fundamentals of Human Gait
Terminology
Details of the Gait Cycle
 Clinical insight
Clinical insight
Stance Phase
Heel Contact (0% Point of the Gait Cycle)
Foot Flat (8% Point of the Gait Cycle)
Mid Stance (30% Point of the Gait Cycle)
Heel Off (40% Point of the Gait Cycle)
Toe Off (60% Point of the Gait Cycle)
 Consider this…
Consider this…
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree



 Objectives
Objectives Key Terms
Key Terms