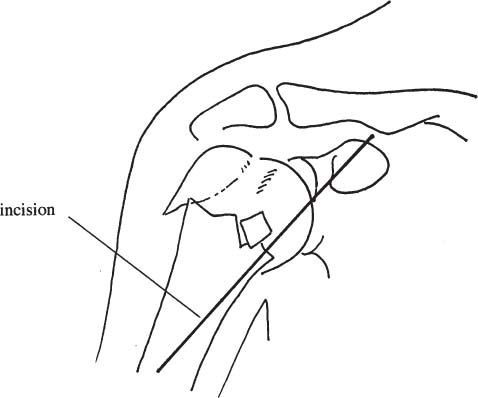
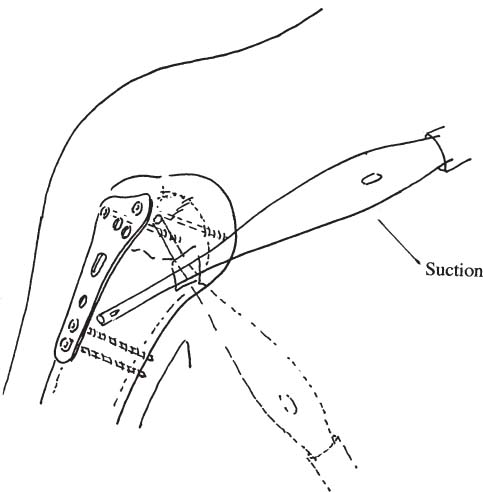
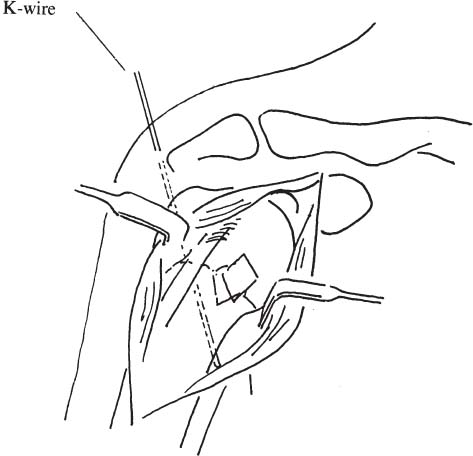
Chapter 28 In the majority of the proximal humeral fractures, satisfactory results can be expected with either conservative or operative treatment. However, in cases of elderly patients with advanced osteoporosis, there have been some problems obtaining a successful outcome. These fractures in the elderly patients with advanced osteoporosis are usually unstable. As a rigid and appropriate fixation can not be easily obtained even using a plate and screws, conservative treatment has been considered superior to open reduction and internal fixation.1–3 Conservative treatment, however, sometimes requires a long period of immobilization that causes the limitation of range of motion. We believe that sufficient range of motion is necessary even for elderly patients. Unfortunately, with conventional osteosynthesis, early mobilization cannot be achieved. As augmentation with methylmethacrylate has been helpful in osteoporotic fractures of distal femur,4 distal radius,5 and calcaneus,6 we have performed an intramedullary cement fixation procedure for proximal humeral fractures in the elderly since 1997. The improved stability achieved by cement augmentation allows immediate mobilization, so we believe this procedure is suitable treatment for elderly patients with advanced osteoporosis. Patients over 75 years old with advanced osteoporosis who have sustained proximal humeral fracture that is unstable due to insufficient bone stock have an absolute indication for this procedure. The patient was placed in the beach chair position with a sandbag under the shoulder. Using a deltopectoral incision (Fig. 28–1), the fracture was carefully reduced. Temporary fixation with a Kirschner wire was added where needed (Fig. 28–2). With the aid of a fluoroscope, an eight-hole plate was placed lateral to the bicipital groove. The proximal fragment was then fixed with cancellous screws using two holes, and the distal shaft was fixed with cortical screws using two holes to keep the alignment. If there was no perforation, the cortex of the fracture area was incised over an area about 15 × 10 mm. In the osteoporotic bone of the elderly, the medullar cavity is commonly almost empty. After careful irrigation of the cavity (Fig. 28–3), it was filled with dough-type bone cement using a pressurized cement gun (Fig. 28–4). Using the remaining four holes of the plate, cancellous screws should be inserted into the intramedullary bone cement before polymerization of the methylmethacrylate is complete. To prolong the working time, the cement is cooled before the operation.7 Used in this manner, bone cement acted as an internal fixation material and as an anchor for the screws. FIGURE 28–1 Schematic drawing of deltopectoral incision. FIGURE 28–2 Temporary fixation with a Kirschner wire. FIGURE 28–3 Irrigation of the cavity.
INTRAMEDULLARY CEMENT
FIXATION OF PROXIMAL
HUMERAL FRACTURES IN THE
ELDERLY PATIENT
SURGICAL TECHNIQUE AND POSTOPERATIVE CARE
Related posts:
 External Fixation in Osteoporotic Bone
External Fixation in Osteoporotic Bone
 Internal Fixation of Osteoporotic Acetabular and Pelvic Fractures
Internal Fixation of Osteoporotic Acetabular and Pelvic Fractures
 An Axially Mobile Plate for Fracture Fixation
An Axially Mobile Plate for Fracture Fixation
 The Huckstep Nail for Fixation of Mechanically Deficient Femoral Bone
The Huckstep Nail for Fixation of Mechanically Deficient Femoral Bone
 A Self-Guided Pedicle Screw for Anterior Fixation of Cervical Spine
A Self-Guided Pedicle Screw for Anterior Fixation of Cervical Spine
 Minimally Invasive Surgery for the Treatment of Vertebral Compression Fractures
Minimally Invasive Surgery for the Treatment of Vertebral Compression Fractures
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


