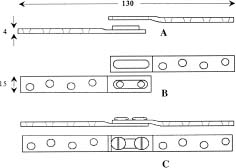
Chapter 26 Fracture healing is greatly influenced by the biomechanical environment at the fracture site. In terms of fixator design, this is determined by the type of fixation method and the structural properties of the fixator. In plate fixation, there has been considerable interest in recent years in assessing the effects of plate stiffness on fracture healing. This has arisen for two reasons. Firstly, the traditional rigid plate is known to give rise to stress-shielding of the bone at the fracture site, causing bone resorption and local bone weakness. Secondly, fractures supported by standard compression plates heal by primary bone healing and there has been concern about unacceptable rates of refracture for primary healed bone after the removal of the implant.1,2 Bone porosity and loss of strength at the fracture site have also been associated with vascular impairment due to the presence of a bone plate,3,4 but low-contact plates are now available5,6 or being evaluated7 to help alleviate this problem. From a biomechanical standpoint the superiority of secondary bone healing has been emphasized as it provides an earlier restoration of the strength of the fractured diaphysis to its former level.8–11 Secondary bone healing and bone remodeling can be promoted by reducing the stiffness of the fixator. When considering plate design, it is generally agreed that a high torsional stiffness is necessary for maintaining alignment and should not be compromised.11 The use of fixators with reduced bending stiffness has proved to be effective in stimulating callus formation,12,13 but the risks of delayed union, fixator failure, and fracture dislocation have made the routine use of such fixators unsafe.14–16 Much experimental and clinical work has shown the beneficial effect on bone healing from reduced axial stiffness of fixators and from intermittent axial compression provided by a device attached to an external fixator.17–20 In fact, axial dynamization has become one of the most important functions of modern external fixators. In comparison, much less work has been done on internal fixators. Two examples of plates designed for axial flexibility are the tubular plate21 and the axially flexible plate,22,23 both of which have been shown in animal experiments to produce healing bone that has superior mechanical and structural properties to bone fixed with rigid plates. The tubular plate has a rigid tubular cross section that is filled with a flexible polymeric material. Its low axial stiffness, obtained from the small cross-sectional area of the metal tube, permitted the underlying bone to take a greater proportion of the load than did stiffer plates.21 This enabled improved postunion healing. The axially flexible plate is made from stainless steel. A low-modulus elastic insert, made of a polymer, fits into each of its six screw holes. Screws pass through holes in the inserts, providing a structure that is flexible axially. In a study using dogs,23 four plates with different axial stiffnesses were tested. In all cases healing was found to be superior to that obtained with the dynamic compression plate in terms of bone stiffness. The rate of healing was affected by the stiffness of the flexibility of the plate. An axial sliding plate offers freedom of axial movement and full axial load carrying by the bone at the fracture site. This of course limits its use to fractures that are not comminuted, because they lack bony support after fixation. The earliest sliding plate design was the “Eggers Splint,”24 developed in 1948. This has two long slotted screw holes into which screws are tightened against the plate and then backed off one turn. The author believed that muscle forces would produce compression and that the bone ends would be guided toward each other through the slotted plate mechanism. This simple plate has more recently been tested on femora in canine subjects25 and found to produce a stronger bone in the earlier stages of healing, with less intracortical resorption. The uncertainty of the sliding mechanism, however, means that the plate is unlikely to find future clinical use. An axially mobile plate (AMP) has been designed by the authors26,27 to allow the bone fragments free axial movement after fixation while maintaining bending and torsional stability. It is expected that the use of such a plate for long bone fracture fixation would remedy some of the shortcomings of other internal fixation plates, particularly the fracture fragment end resorption that has been noted in flexible plate fixation and the stress-shielding that occurs with rigid fixation. This would result in a quicker healing process and a stronger healed bone. Figures 26–1A through C show a schematic diagram of the AMP. There are two parts, which together form a sliding mechanism. One part has two holes set into a raised elongated column; the other has a matching elongated hole such that the parts can slide longitudinally while constraining movement in other directions. Two screws with large heads connect the two parts. The depth of the elongated column is slightly greater than that of the matching section with the elongated hole, so when the screws are fully tightened there is a set clearance for the components to slide. The maximum sliding distance is 2 mm. All components are made from surgical grade stainless steel (316L). The AMP plate dimensions are similar to those of commonly used plates so its bending and torsional stiffness will also be similar. The dimensions shown on the representative plate in Figure 26–1 would make it suitable for tibial or humeral fixation. FIGURE 26–1 Axially mobile plate (AMP): (A) exploded side view; (B) exploded top view; and (C) assembled side and top views. (Reprinted with permission from Jun et al.27)
AN AXIALLY MOBILE PLATE FOR
FRACTURE FIXATION
BIOMECHANICAL CONSIDERATIONS
AXIALLY FLEXIBLE PLATES
SLIDING PLATE FIXATION
DESIGN OF THE AMP PLATE
MECHANICAL
Related posts:
 External Fixation in Osteoporotic Bone
Norian SRS Resorbable Cement for Augmentation of Internal Fixation of Hip Fractures
Synthes Spiral Blade Intramedullary Nail System for Proximal Humeral Fractures
An Injectable Cementing Screw for Fixation in Osteoporotic Bone
Internal Fixation of Osteoporotic Long Bone
Enhanced Stability of External Fixation with Hydroxyapatite-Coated Pins
External Fixation in Osteoporotic Bone
Norian SRS Resorbable Cement for Augmentation of Internal Fixation of Hip Fractures
Synthes Spiral Blade Intramedullary Nail System for Proximal Humeral Fractures
An Injectable Cementing Screw for Fixation in Osteoporotic Bone
Internal Fixation of Osteoporotic Long Bone
Enhanced Stability of External Fixation with Hydroxyapatite-Coated Pins
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


