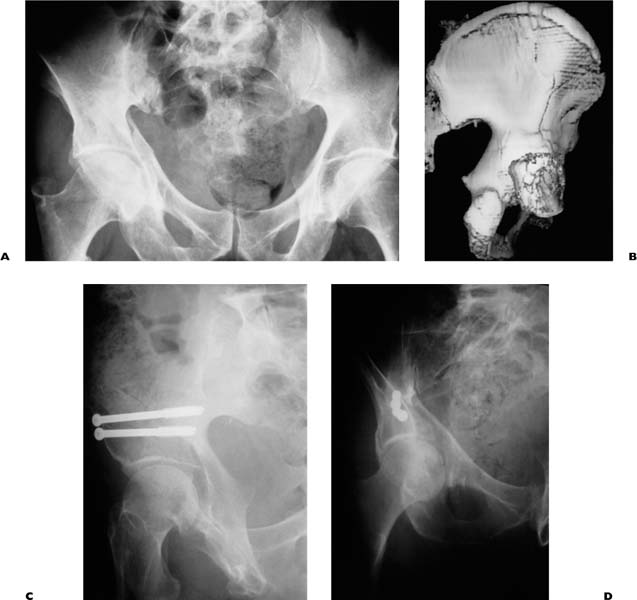
Chapter 10 Fractures of the acetabulum and pelvis represent uncommon injuries that, nevertheless, are growing rapidly in number. Historically, these traumatic insults have been viewed as the aftermath of major trauma, typically related to motor vehicles, and especially in young adults following exposure to alcohol and/or drugs.1 Many of these fractures follow minor trauma, such as a simple fall to the ground from a standing position.2 The minor traumatic injuries occur primarily in the elderly with osteoporotic bone, although they may arise in younger individuals with osteoporosis secondary to an inflammatory arthritis and steroid dependency. In many of the latter group, there is no history of a true accident, in which case the term insufficiency fracture is applied. With the rapidly aging population, and including those individuals with predisposing factors such as prior pelvic irradiation therapy or steroid dependency, the number of clinical presentations is soaring.2–4 For example, currently in the United States, annually there are approximately 300,000 hip fractures, 16,000 pelvic fractures, and 3000 acetabular fractures involving osteoporotic bone. Unless preventive measures are markedly improved, all of these figures can be expected to at least double during the next 20 years. This chapter outlines the clinical presentations, diagnostic features, biomechanical factors, and modified techniques of fixation as well as complications of these fractures. Historically the hallmark of pelvic or acetabular trauma is a recent motor vehicular accident involving a young adult, typically after exposure to alcohol or drugs.1 Many pelvic fractures are accompanied by injuries to multiple organ systems. A somewhat special circumstance is the presentation of similar multiple traumatic insults in an elderly individual, over 70 years of age.5,6 Typically the more limited physiological reserves of the older person are further impaired by the presence of comorbidities such as ischemic heart disease, diabetes mellitus, and cerebrovascular disease. Overall, such a patient possesses a much higher mortality and a greater likelihood to sustain multiple complications from the event than is the case for his younger counterpart.7 The recovery period, including the duration of hospitalization, is likely to be much longer than for a young adult. Also, the elderly person has a higher likelihood of displaying permanent physical impairment than his younger counterpart. One such example in the elderly is where inadequately controlled hypovolemic shock precipitates a myocardial infarct. In turn, surgical reconstruction of an unstable pelvic ring or displaced acetabular fracture may be deferred indefinitely, so that the prognosis for the recovery is significantly impaired. In the presence of marked osteoporosis, the types of acetabular and pelvic injury patterns that present clinically are different from those that occur in young, healthy adults.8 In part, the discrepancies follow the mechanisms of trauma that usually occur in younger and older individuals. Whereas the younger patients sustain major trauma, most of the elderly sustain minor traumatic incidents that would be unlikely to provoke a fracture in a young and healthy individual. Where an elderly, osteoporotic patient presents after major trauma to the pelvis, the fracture is likely to display marked comminution. If the acetabulum is involved, both the femoral head and the acetabulum may be highly impacted as well as fractured. Such complicating features unfavorably impact the prognosis. With such acetabular involvement, a surgical reconstruction may be unlikely to provide a correction of impaction so that posttraumatic arthritis is exceedingly likely to occur. In part, the differences observed for pelvic injuries in younger versus older individuals correlate with the different mechanisms of trauma including the vectors of the provocative blow. As initially described by LeTournel and Judet,9 the characteristic pattern of an acetabular fracture depends upon the precise vector of the provocative blow. With a forceful injury, an associated or comminuted fracture pattern is likely such as a posterior wall-posterior column, a posterior wall-transverse, a T-type, or a both-column fracture. In an elderly, osteoporotic individual who sustains a simple fall to land on the side of his hip, a comminuted anterior column fracture is the most frequently encountered injury. The fracture site involves the thinnest and weakest portion of the acetabulum that is further compromised by the osteoporosis. One specific fracture pattern involves the anterior wall, column, and quadrilateral surface and is rarely observed in young adults.10 Another frequent injury in elderly individuals is a posterior wall fracture in which the wall undergoes so-called marginal impaction. The area of involvement varies greatly. Impaction or deep abrasive damage to the femoral head often accompanies the acetabular impaction and comminution. Ironically, this “simple” injury pattern possesses a poor prognosis that is much worse than certain associated fractures, such as the typical both-column fracture. With respect to the pelvic ring, after a major trauma, an unstable injury of the posterior pelvic ring may involve a dislocated sacroiliac joint or a displaced fracture of the posterior ilium or sacrum.1 Following minor trauma or minimal trauma, such as an insufficiency fracture, the typical pattern of injury is the propagation of a minimally displaced fracture across the sacral ala, accompanied by uni- or bilateral ramus fractures.11,12 One special manifestation of an insufficiency fracture is where the patient has a prior history of pelvic irradiation therapy, typically for uterine or prostatic carcinoma.13 Years later, in the face of an apparent cure, the pelvis is vulnerable to an insufficiency fracture, followed by a delayed union or nonunion. The compromised healing potential of the bone may lead to a prolonged symptomatic course. A similar clinical picture may follow steroid dependency, particularly for rheumatoid arthritis or lupus erythematosis. In this situation a complicating feature may be a prior history of a total hip replacement. Here, initially an insufficiency fracture of the sacral ala may propagate across the partly or completely fused sacroiliac joint into the posterior ilium. Then, the fracture advances across the acetabulum to create a periprosthetic fracture, possibly accompanied by loosening of the cup. Usually, such a fracture exits through the superior pubic ramus. A stabilization of the pelvic ring may necessitate a revision of the cup. While most acetabular and pelvic fractures ultimately unite, after a conservative course of treatment, a small percentage progress to a nonunion.14,15 This likelihood increases enormously after prior pelvic irradiation therapy, which heavily compromises bony healing and remodeling. Where a nonunion persists, the principal symptoms are pelvic pain, aggravated by activity, and pelvic instability. The latter problem is highly disabling, whereby the patient perceives an unnatural motion of the nonunion site with sitting, transfers, ambulation, or even rolling in bed. In the presence of a sacral insufficiency fracture that becomes a nonunion, an insidious presentation of a pelvic deformity may ensue that is typified by a sagittal and internal malrotation of the involved hemipelvis. The injury hinges around the sacral nonunion so that the maximum deformity occurs at the sites of the ramus disruptions. The epidemiologic features of pelvic fractures in the elderly have been evaluated by Melton et al,3 Ragnarsson and Jacobsson,2 and Kannus4 in both the United States and Europe. The incidence of pelvic fractures in the elderly following minor trauma is increasing rapidly, especially in women. In the most recent study, from Finland,4 during the period from 1971 to 1997, the incidence of major pelvic trauma after motor vehicular trauma declined while the number of osteoporotic fractures in the elderly after minor trauma increased by 4.6 times. The authors predict an exponential increase in these numbers during the next two to three decades. Further studies are needed to reappraise these dire predictions and to evaluate preventive methods as well as potentially superior methods of definitive treatment. For the osteoporotic individual who presents for an evaluation of a presumptive pelvic fracture, one clinical scenario follows a major traumatic event, where a careful evaluation of multiple organ systems and timely initiation of a therapeutic protocol is necessary. These schemes are fully presented elsewhere.1 The more typical clinical picture is an elderly individual or a somewhat younger adult with known risk factors for osteoporosis, such as a steroid-dependent inflammatory arthropathy, chronic alcoholism, or prior pelvic irradiation therapy. A history of a simple fall or other minor injury may be present, followed by an inability to transfer or to ambulate. Alternatively, no traumatic event may have occurred or a senile patient may not be able to give an adequate history. Still another presentation is of an insidious onset of pelvic pain and a progressive deterioration of ambulation and transfers. During transfers or possibly when rolling in bed, the patient may be aware of a sudden onset of focal pelvic pain and a sense of motion within the pelvis that is very unsettling. This history typifies pelvic instability. On examination, the relevant portion of the pelvis may be tender. If a fall occurred recently, ecchymosis and soft tissue swelling may be evident, especially overlying the greater trochanter, ischium, or iliac crest. Unlike a patient with a hip fracture, the individual does not display a deformity of the relevant lower extremity, such as the typical external rotation and foreshortening. Whereas the hip fracture victim complains of severe pain with even minute motion of the hip, the pelvic and acetabular fracture victim does not complain of pain, at least with limited passive motion of the hip. The patient may even display limited active motion of the hip, which is highly unusual after a proximal femoral fracture. Usually the acetabular fracture patient has pain on passive motion of the hip, but no intrinsic deformity of the hip. Standard radiographs of the pelvis and acetabulum include an anteroposterior (AP) view and 45-degree iliac and obturator oblique views, along with 40-degree outlet and inlet views.1,9 The former three are used to study the acetabulum while the last two supplement the AP view to permit an assessment of the pelvic ring. A computed tomography (CT) scan is needed to evaluate the posterior pelvic ring, especially the sacrum, along with the acetabulum and rami. In the assessment of the osteoporotic pelvic fracture, the CT scan is particularly helpful to permit the detection of an occult fracture of the sacral ala or transforaminal region. A minimally displaced fracture of the superior ramus, possibly extending into the anterior acetabulum, may be detected, along with an accompanying inferior pubic ramus or ischial fracture. With respect to an acetabular fracture in the presence of osteoporosis, impaction of the subchondral bone is a frequent accompanying feature. Various patterns of posterior fracture dislocation are the most frequent injuries to display impaction, both of the acetabulum and of the femoral head. If impaction of the femoral head is visualized radiographically, usually the area of involvement that would be inspected during an open reduction is much larger than that impression which would be evident by a study of the CT scan. In the CT views, the degree of comminution tends to be exaggerated by the images of bony fragments that possess convoluted surfaces. Nevertheless, the conventional radiographs inadequately display comminution. After a review of the images, the injury pattern is characterized by one of the available schemes.1 For both the pelvic ring and acetabulum, the alphanumeric Comprehensive Classification (CCF) System16 is the most detailed and represents an outgrowth of most prior classifications. As an alternative, the acetabulum may be characterized by the method of LeTournel and Judet9 into one of five simple or five associated injury patterns. A rigorous classification permits a determination of the prognosis, the available methods of treatment, and a guideline to a surgical plan, where appropriate. For unusually displaced fractures, especially of the acetabulum, a three-dimensional CT scan affords the optimal recognition of a complex multiplanar rotational deformity as a guideline to surgical planning.17 Many of the fractures after minor trauma are minimally displaced and unrecognizable by a review of plain radiographs or even a computerized tomogram. During the review of the history of the patient, and especially where the patient is a poor historian, the examiner needs to consider the potential diagnosis of an occult fracture of the proximal femur or acetabulum and pelvic ring. If an elderly or especially a demented patient is unable to transfer or ambulate, with apparent hip or pelvic pain and despite the presence of normal plain hip and pelvic radiographs, the presumptive diagnosis is a minimally displaced fracture, until proven otherwise.18 The optimal diagnostic method is either a technetium bone scan or magnetic resonance imaging (MRI). The latter method permits a detailed characterization of the injury site where the fracture propagates in an irregular manner across the involved segment of bone. During an inspection of the MRI, a careful scrutiny of the femoral neck and intertrochanteric regions for an occult fracture is needed for what may be the sole injury or an accompanying one. MRI also provides the most reliable diagnostic method to distinguish an insufficiency fracture from a malignancy or recurrent tumor in the bone, or to document an effusion of the hip.19 For an acute minimally displaced fracture of the pelvic ring or acetabulum, conservative treatment suffices, with a resolution of symptoms during a 6- to 12-week period. Nevertheless, occasionally the occult fracture is an unstable or potentially unstable one that is vulnerable to displacement if the patient is mobilized less than 4 weeks after the injury. Examples include a minimally displaced transtectal transverse acetabular fracture, a high anterior column fracture, an anterior column-posterior hemitransverse fracture, or a vertical fracture of the posterior ilium. In any of these situations, a therapeutic alternative is percutaneous fixation under image guidance with the use of cannulated screws (Fig. 10–1). The method requires a familiarity with the appropriate pelvic columns of available bone and the techniques for intraoperative image guidance with either an image intensifier or a CT scanner. When properly used the method provides rapid relief of pelvic pain and the potential to mobilize the patient promptly. FIGURE 10–1 The use of percutaneous screws for a minimally displaced but unstable anterior column-posterior hemitransverse fracture in an osteopenic man of 75 years. The 7 mm cannulated screws were inserted into the anterior-inferior spine under image intensification, with the use of a radiolucent operating table. (A) Anteroposterior (AP) view. (B) External iliac three-dimensional CT view. (C) Postoperative iliac oblique view. (D) Postoperative obturator oblique view. Almost all displaced posterior fracture dislocations are unstable whereby any residual deformity is poorly tolerated by the hip joint. Similarly, displaced, juxta-, and supratectal transverse fractures are poorly tolerated. Comminuted T-type and transverse posterior wall injuries likewise are indications for surgery. These and other injury patterns that possess an incarcerated fragment or an acetabular deformity that is incongruent with the femoral head merit consideration for an open reduction and internal fixation. For a displaced fracture with one or more of the previously described features that typically would be indicative of an open reduction, the most frequent contraindication is the presence of a comorbid condition that renders the patient unstable, such as uncorrected hemorrhagic shock or a recent myocardial infarct. In the osteoporotic elderly, this type of situation is much more common than arises with respect to younger individuals. With the technical complexity of many of these fractures, the possession of the appropriate surgical skills, training, and technical resources is essential. If the surgical procedure has to be deferred for more than 3 weeks, in view of unstable medical conditions or other considerations, then the surgical procedure becomes immeasurably more difficult.9 During the intervening period, erosion of the femoral head may eliminate any possibility for a favorable outcome. If the surgery has to be deferred, the use of skeletal traction may lessen the degree of erosive damage. Prior to such a delayed procedure, the imaging studies are repeated to determine the degree of erosion and the merits of an open reduction. In the authors’ opinions, once the femoral head is destroyed as a bearing surface, then an open reduction of the acetabulum is no longer indicated. Alternatively, the procedure of choice is a total hip arthroplasty performed before or after the fracture is fully united.8 Nevertheless, many elderly patients who undergo an open reduction and internal fixation of their acetabular fractures achieve a highly satisfactory outcome, especially in physiologically younger and more active individuals.20 Overall, the intrinsically poorer results that have been reported for progressively older patients appear to be related to the sizable subgroup of patients that are inactive and osteoporotic.9,21 In certain osteoporotic individuals, extensive areas of impaction to the femoral head and acetabulum may be present. Marked comminution may further hamper any attempt at an accurate and stable open reduction and internal fixation. If the procedure has to be deferred beyond 3 weeks, usually the outcome in such a patient is poor. Still other elderly patients present with preexisting severe degenerative arthritis. For any combination of these factors, another therapeutic option is primary conservative treatment. Once the acetabulum is healed and if the patient becomes symptomatic with posttraumatic arthritis, then a total hip arthroplasty can be considered.22 Another therapeutic option is an acute total hip replacement with concomitant internal fixation of the osteoporotic fracture.23,24 While the role for the latter solution remains somewhat controversial, nevertheless the method provides the shortest overall recovery period for the unusual case where either an acute open reduction or the use of conservative treatment possesses an abysmal prognosis. An open reduction is recommended for most unstable pelvic ring disruptions with true posterior instability.1,15 Although the clinical outcomes after the treatment of unstable pelvic fractures with the use of internal and external fixation are optimized, some degree of residual disability and persistent pelvic pain is not uncommon.25–28 For minor trauma or after an insufficiency fracture that involves the pelvic ring, most of these minimally displaced injuries heal un-eventfully after conservative treatment.29 In one of the few long-term studies on the recoveries of older patients, by Morris et al,30 there was an unfavorable impact on the patient’s mobility, at least for the short term. Over a longer period of up to a year, many of the patients displayed a need for increased levels of support by the community, or institutionalization. The in-patient mortality was 7% and the mortality at 1 year was 27%, secondary to the frequent presence of comorbidities. Some of the individuals remained symptomatic for periods of many months or longer.14 Explanations for the persistent pain included the presence of osteoporosis, a pelvic nonunion, and/or a history of prior pelvic irradiation. An extended period of incapacitating pelvic pain in the presence of a radiographic nonunion that fails to show signs of radiographic healing during a period of a few months or longer is an indication for an open reduction and internal fixation. Occasionally, such a nonunion undergoes an insidious onset of a deformity, with an internal rotation and sagittal malrotation that hinges around the involved side of the sacrum. In our experience, the onset of a deformity is an indication for surgical stabilization, prior to the origin of a major deformity that would impede the surgical reconstruction. Once a large fracture gap appears, at the time of an open reduction and in the face of osteoporotic bone and especially after a prolonged duration of the problem, reapproximation of the displaced fragments with an obliteration of the fracture gap is exceedingly difficult. If an insufficiency fracture propagates across the acetabulum with radiographic loosening of the cup, an open reduction and internal fixation of the fracture including a revision of the cup is usually necessary to achieve symptomatic relief. Accompanying technical challenges may include the obliteration of a large acetabular defect.31 The surgical plan involves visualization of the hip joint and the site (s) of the pelvic nonunion or at least arrangements to perform appropriate percutaneous fixation of a stable acetabular fracture and cup. While many biomechanical factors pertaining to the fixation of osteoporotic bone were reviewed in Chapter 4, a few special considerations germane to the pelvis follow. Most conventional pelvic fixation techniques rely upon the use of isolated screws or screws employed with an accompanying plate. The fixation depends upon the holding power of the screws in the osteoporotic bone. Overall, the bony pelvis consists of two thin peripheral layers of cortical bone and a thicker intervening layer of cancellous bone. Screw fixation rests upon the anchorage of the screws in the cancellous bone. The holding power of a screw in a porous material such as cancellous bone or its resistance to pullout has been characterized by Tencer et al.32 These observations were derived from prior bio-mechanical studies.33,34 The resistance to pullout is dependent upon six factors, three of which are related to the geometry of the screw: its outer diameter, its length of contact with the bone, and its thread geometry. The other three factors pertain to the shear strength of the adjacent bone, the size of the pilot hole, and the features of tapping. In cancellous bone, tapping can be eliminated as a significant factor, along with the size of the pilot hole. From quantitative assessments, the relationships in Table 10–1 account for 97% of the variability of the pullout strength for nontapped screws that are inserted into a porous foam that is a mechanical equivalent to cancellous bone. For virtually all types of pelvic fixation, generally one or more of four types of screw are used: a 6.5 or 7 mm (large) cannulated cancellous screw, a 6.5 mm (large) noncannulated cancellous screw, a 4.5 mm (large) cortical screw, or a 4 mm fully threaded (small) cancellous screw. It is useful to examine the relative holding power of these examples, in various lengths, and how varying degrees of osteoporosis influence their holding power. In Table 10–2, the geometric and mechanical features of these screws are listed. Since the 7 mm cannulated and 6.5 mm noncannulated screws possess nearly identical features referable to their holding power, only the latter is listed.
INTERNAL FIXATION OF
OSTEOPOROTIC ACETABULAR AND
PELVIC FRACTURES
THE IMPACT OF OSTEOPOROSIS ON CLINICAL PRESENTATIONS
EPIDEMIOLOGY
DIAGNOSIS
OCCULT PELVIC AND ACETABULAR FRACTURES
INDICATIONS AND CONTRAINDICATIONS FOR SURGICAL TREATMENT
PERCUTANEOUS FIXATION
DISPLACED ACETABULAR FRACTURES
CONTRAINDICATIONS TO AN OPEN ACETABULAR REDUCTION
TOTAL JOINT ARTHROPLASTY
THE PELVIC RING
PERIPROSTHETIC INVOLVEMENT
BIOMECHANICAL CONSIDERATIONS
| Fs | = S × As = S× (L×π× Dmajor) × TSF | |
| Where | ||
| Fs | = predicted shear failure force (N) | |
| S | = material ultimate shear stress (Mpa) | |
| As | = thread shear area (mm2) | |
| L | = length (mm) | |
| Dmajor | = major diameter (mm) | |
| (L×π× Dmajor) | = area of a cylinder of diameter Dmajor and length L | |
| TSF | = thread shape factor (dimensionless) | |
| = (0.5 + 0.57735d/p) | ||
| d | = thread depth (mm) | |
| = (Dmajor—Dminor)/2 | ||
| Dminor | = minor (root) diameter (mm) | |
| p | = thread pitch (mm) | |
For the large cancellous screw, thread lengths of 16 mm and 32 mm are commonly stocked. While fully threaded models are commercially available, most hospitals do not routinely stock them. For the purpose of this discussion, the 4.5 mm and 4 mm screws are evaluated with thread lengths of 15, 30, 60, and 90 mm. These lengths are widely used in pelvic surgery, admittedly with the exceptional longer or shorter variants. In Table 10–3, the corresponding thread shear areas, As (mm), for useful pelvic bone screws of assorted lengths are displayed.
Related posts:
 External Fixation in Osteoporotic Bone
Norian SRS Resorbable Cement for Augmentation of Internal Fixation of Hip Fractures
An Injectable Cementing Screw for Fixation in Osteoporotic Bone
Improving the Distal Fixation of Intramedullary Nails in Osteoporotic Bone
Internal Fixation of Osteoporotic Long Bone
Enhanced Stability of External Fixation with Hydroxyapatite-Coated Pins
External Fixation in Osteoporotic Bone
Norian SRS Resorbable Cement for Augmentation of Internal Fixation of Hip Fractures
An Injectable Cementing Screw for Fixation in Osteoporotic Bone
Improving the Distal Fixation of Intramedullary Nails in Osteoporotic Bone
Internal Fixation of Osteoporotic Long Bone
Enhanced Stability of External Fixation with Hydroxyapatite-Coated Pins
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


