61
Intraarticular Distal Radius Fractures: Volar Approach, Dorsal Approach, and Arthroscopic Reduction
Kevin D. Plancher
History and Clinical Presentation
A 55-year-old right hand dominant woman was ice skating when she fell on her dominant outstretched hand. She had immediate pain and swelling. She noticed an obvious deformity near her wrist.
Physical Examination
The patient is holding her right hand and wrist close to her body. She is tentative when moving her right arm away from her body to be examined. She has an obvious deformity at the wrist with swelling, but the skin is intact (Fig. 61–1). She has full sensation to light touch of all fingers and has good capillary refill of fingers. Her radial and ulna pulse is normal. With the wrist supported, her elbow exam shows no tenderness with palpation or range of motion. Patient also reports no pain in her shoulder with range of motion or palpation.
Diagnostic Studies
The standard zero anteroposterior (AP) (Fig. 61–2A), lateral (Fig. 61–2B), and oblique radiographs of the distal radial injury are very important because they show the extent and direction of the initial displacement. Traction radiographs assist the surgeon in determining whether the fracture is intraarticular or extraarticular and should be done only in the operating room under anesthesia because of the pain produced with traction.
PEARLS
- Mini C-arm can be useful in verifying proper fixation.
- Complete muscle relaxation is necessary for reduction.
PITFALLS
- Overdistraction with external fixator can lead to RSD.
- Inaccurate reduction can lead to complications.

Figure 61–1. A closed distal radius intraarticular fracture.

Computed tomography (CT) exams may be helpful to determine the amount of displacement or if comminution is large or when the fracture pattern is difficult to visualize on plain radiographs. Three-dimensional reconstruction often makes the fracture look more complex than it really is.
Differential Diagnosis
Extraarticular distal radius fracture
Displaced versus nondisplaced
Intraarticular distal radius fracture
Displaced versus nondisplaced Tumor
Diagnosis
Distal Radius, Intraarticular Fracture Displaced
Most injuries to the articular surface of the distal radius are caused by shear from high-energy injuries. These fractures can cause degeneration of the joint, even if only a small amount of displacement is present. Treatment is determined by the fracture pattern, degree of displacement of the fracture fragments, and stability of the fracture.
Fractures can be classified by the Melone classification system, which is based on the importance of the medial portion of the articular column of the distal aspect of the radius in determining the options for treatment (Table 61–1). By definition, this classification is relevant only to intraarticular fractures. Interobserver disagreement is common with this system, as observers often disagree about whether or not the fracture extends into the radiocarpal joint.
| Classification | Description |
| Type I | Four-part minimally displaced |
| Type II | Carpus displacement (displaced anterior or posterior) |
| Type III | Volar spike |
| Type IV | Volar fragment (palmar medial and dorsal medial rotation) |
Surgical Treatment
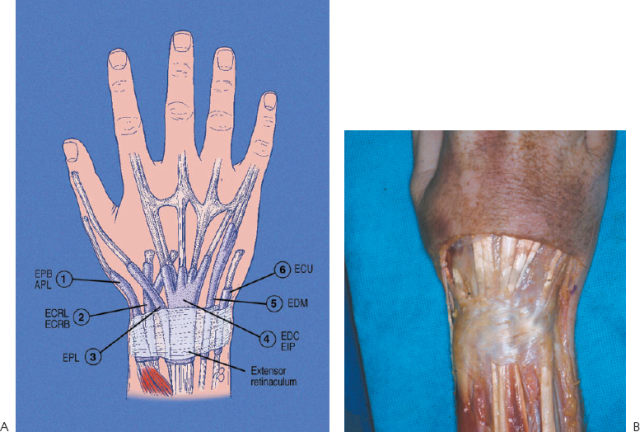
Open Reduction and Internal Fixation (ORIF): Dorsal Approach
A longitudinal midline incision is made over the dorsum of the wrist, which provides useful and practical exposure of the dorsum of the radius (Fig. 61–3). The extensor pollicis longus (EPL) is identified distally and traced to the third dorsal compartment. This compartment is often distended from fracture hematoma, and most fractures that split the scaphoid and lunate facets extend into the floor of the third compartment. This occurs because the stronger and thicker Lister tubercle influences the fracture pattern. The third and fourth compartments are sharply elevated off the dorsal aspect of the capsule, with both the tendon compartments and the dorsal capsular ligaments, including the dorsal radiotriquetral ligament, kept intact. Following this technique avoids the need to repair the extensor retinaculum and related compartments later. Swelling of the tendons and the joint capsule can make closure more difficult. If the dorsal retinaculum is divided and not repaired, the tendons of the fingers and wrist will bow-string with extension of the wrist. The EPL is translocated radially to allow for visualization of the fracture.