CHAPTER 3 Instrumentation and Operative Setup for Ankle and Subtalar Arthroscopy
PREOPERATIVE CONSIDERATIONS
Diagnostic Assessment
If doubt remains after this assessment, more advanced imaging and possibly diagnostic injections may assist in determining the nature and location of the pathology1. Liberal use of preoperative diagnostic injections can pinpoint symptomatic pathology, which can aid in decision making for the operating room setup. A patient with anterior and posterior ankle pathology may have complete resolution of symptoms with an anterior ankle injection, obviating the need for posterior access and vice versa. For lesions on the talar dome, it is essential to assess the extent of ankle plantar flexion to determine whether an anterior approach alone is sufficient to access the lesion.
Operating Room Setup
Some surgeons may choose to use an arthroscopic pump. Occasionally, fluoroscopy is necessary, which requires a significant amount of space. The arthroscopy tower should be mobile to optimize its position for each case. The components of the arthroscopy tower are listed in Box 3-1 and shown in Figure 3-1. The equipment table is used for therapeutic instruments. The instruments routinely used during the diagnostic arthroscopy (e.g., scalpels, 18-gauge needle, trocars, cannulas, probes) are placed on a Mayo stand for easy accessibility (Fig. 3-2). Backup equipment should be readily available in the event that additional instrumentation is required.


Anesthesia and Positioning
The most appropriate patient positioning for ankle arthroscopy is a matter of the surgeon’s preference. Supine and lateral positions are well described. There are two common variations of the supine position (Fig. 3-3). In the first, the patient is placed supine with the operative leg placed in a knee holder. The knee is placed just distal to the break in the operating room table, and the foot of the bed is lowered to allow the lower leg to rest unsupported.2 A second option is to place the patient supine and use a well-padded thigh holder to position the operative leg such that the hip is flexed 45 degrees and the leg is allowed to hang, providing access to the ankle.3 The lateral position has been described by Parisien (Fig. 3-4).4 It involves placing the patient in a 45-degree lateral position with the operative side up. A platform (box or sheets) is placed underneath the operative leg to elevate it above the nonoperative leg. The hip is externally rotated to access the anterior aspect of the ankle. The leg can be returned to neutral position for access to the lateral or posterior aspects of the ankle. Harbach5 modified the lateral position with the addition of a thigh holder, which allows the ankle to hang similar to the supine position described previously. Although all previously described positions may be used for subtalar arthroscopy, the most common approaches are from the lateral position or posteriorly with the patient in the prone position.


ARTHROSCOPIC METHODS AND INSTRUMENTATION
Distraction
Although several methods of invasive distraction exist, all involve drilling traction pins or wires into bone. The well-described Guhl technique uses two  -inch threaded Steinmann pins and an external distraction device containing a strain gauge and a pivoting distal end.6 The proximal pin is placed into the distal tibia approximately 3 to 5 cm proximal to the ankle joint and 1 cm posterior to the anterior tibial crest. The distal pin is placed into the calcaneus 2 to 2.5 cm anterior to its posterior border and just beneath the peroneal tendons. Both pins are placed in unicortical fashion from lateral to medial aspects. The calcaneus pin should be aimed 20 degrees distally. Many other techniques have been described, including medial distraction with the distal pin in the talus7; medial and lateral distraction8; a single, smooth, 0.045-mm wire passed through the sinus tarsi and attached to weights9; and a single pin through the calcaneus attached to a fracture table.10
-inch threaded Steinmann pins and an external distraction device containing a strain gauge and a pivoting distal end.6 The proximal pin is placed into the distal tibia approximately 3 to 5 cm proximal to the ankle joint and 1 cm posterior to the anterior tibial crest. The distal pin is placed into the calcaneus 2 to 2.5 cm anterior to its posterior border and just beneath the peroneal tendons. Both pins are placed in unicortical fashion from lateral to medial aspects. The calcaneus pin should be aimed 20 degrees distally. Many other techniques have been described, including medial distraction with the distal pin in the talus7; medial and lateral distraction8; a single, smooth, 0.045-mm wire passed through the sinus tarsi and attached to weights9; and a single pin through the calcaneus attached to a fracture table.10
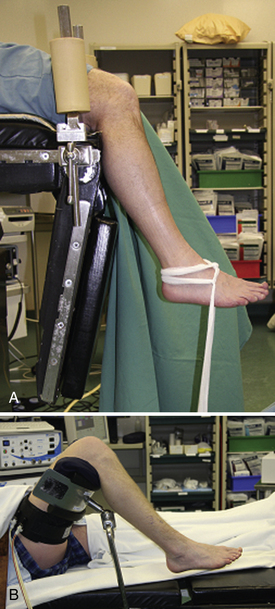
Yates and Grana11 described a means of applying semicontrolled distraction. A small loop is tied in the center of a Kerlix gauze roll. The free ends of the roll are wrapped around the ankle and then passed through the loop. The ends are tied together and then placed underneath the surgeon’s foot. Traction can be added by stepping (similar to stepping on a gas pedal) on the loop underfoot (Fig. 3-5A). Cameron12 modified this technique by passing the loop behind the surgeon’s back, rather than underfoot (see Fig. 3-5B). To apply distraction, the surgeon leans backward.

Takao and colleagues13 use a different bandage configuration to produce equal distraction anteriorly and posteriorly (see Fig. 3-5B). These methods of distraction require little equipment and are very cost effective. However, it is difficult to maintain consistent traction, and some operators may find the multitasking of operating and controlling distraction somewhat onerous. Another disadvantage is that placing the Kerlix roll underfoot or behind the back may compromise the sterility of the procedure.
Related posts:
 Soft Tissue Impingement of the Ankle Joint
Osteochondral Lesions of the Talar Dome: Anatomy, Etiology, and Evaluation
Anatomy, Evaluation, and Operative Setup for Posterior Ankle Arthroscopy
Arthroscopic Fusion for Degenerative Arthritis of the Subtalar Joint
Fusion for Degenerative Arthritis of the Ankle
Diagnostic Arthroscopy for the Ankle and Subtalar Joints
Soft Tissue Impingement of the Ankle Joint
Osteochondral Lesions of the Talar Dome: Anatomy, Etiology, and Evaluation
Anatomy, Evaluation, and Operative Setup for Posterior Ankle Arthroscopy
Arthroscopic Fusion for Degenerative Arthritis of the Subtalar Joint
Fusion for Degenerative Arthritis of the Ankle
Diagnostic Arthroscopy for the Ankle and Subtalar Joints
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


