CHAPTER 16 Tendoscopy
To become familiar with the endoscopic techniques used in foot and ankle surgery, surgeons can train in a cadaveric setting through international courses that are offered annually.1,2 Tendoscopy can be performed for the diagnosis and treatment of pathologic conditions of the peroneal tendons, the posterior tibial tendon, and the flexor hallucis longus (FHL) tendon. These endoscopic procedures and their indications are discussed in this chapter.
TENDOSCOPY OF THE PERONEAL TENDONS
Peroneal tendon pathology frequently coexists with or results from chronic lateral ankle instability. These disorders often cause chronic ankle pain in runners and ballet dancers.3 Post-traumatic lateral ankle pain is common, but peroneal tendon pathology is not always recognized as a cause of these symptoms. In a study by Dombek and coworkers, only 60% of peroneal tendon disorders were accurately diagnosed at the first clinical evaluation.4
Pathology consists of tenosynovitis, tendon dislocation or subluxation, and (subtotal) rupture or snapping of one or both of the peroneal tendons. It accounts for most symptoms at the posterolateral aspect of the ankle. Other causes of posterolateral ankle pain are rheumatoid synovitis, bony spurs, calcifications or ossicles, pathology of the posterior talofibular ligament (PTFL), or disorders of the posterior compartment of the subtalar joint. Posterior ankle impingement can manifest as posterolateral ankle pain.5
The primary indication for treating pathology of the peroneal tendons is pain.6 If conservative treatment fails, the surgical intervention involves débridement of the tendons, fibular groove deepening in case of recurrent peroneal tendon dislocation, and an adequate and precise determination of the location and extent of tendon ruptures. Van Dijk introduced a tendoscopic approach to treat a wide variety of peroneal tendon disorders, and the subsequent patient follow-up was published in 2006.7 The tendoscopic technique is safe and produces good or excellent clinical outcomes, making it a good alternative to open surgical approaches.
Anatomy
The peroneal muscles are located in the lateral compartment of the leg, also known as the peroneal compartment. Both muscles are innervated by the superficial peroneal nerve and the peroneal, and medial tarsal arteries supply the muscles with blood through separate vinculae.8,9 The peroneus brevis tendon is situated dorsomedial to the peroneus longus tendon from its proximal aspect up to the fibular tip, where it is relatively flat. Just distal to this lateral malleolus tip, the peroneus brevis tendon becomes rounder and crosses the round peroneus longus tendon. The distal posterolateral part of the fibula forms a sliding channel for the two peroneal tendons. This malleolar groove is formed by a periosteal cushion of fibrocartilage that covers the bony groove.10 Posterolaterally, the tendons are held into position by the superior peroneal retinaculum.7,11
The peroneal tendons act as lateral ankle stabilizers. In chronic ankle instability, more strain is put on these tendons, resulting in hypertrophic tendinopathy, tenosynovitis, and ultimately in tendon tears.7
In 1803, Monteggia was the first to describe peroneal tendon dislocation in a female ballet dancer.12 These tendons dislocate if the superior peroneal retinaculum ruptures, frequently because of an inversion or dorsiflexion trauma of the foot with the muscles contracted, or if it is congenitally absent or weak.11 A nonconcave fibular groove predisposes to dislocation. The cartilaginous rim, located laterally from the fibular groove, adds to the overall depth of the groove.13 If this rim is absent or flat, the tendons are more likely to dislocate.14
Patient Evaluation
History and Physical Examination
Tendinopathy of the peroneal tendons often coexists with a lateral ankle sprain, and the diagnosis of peroneal tendon pathology in a patient with lateral ankle pain can be difficult.15 The anterior drawer test and varus stress test are applied routinely to detect laxity of the ankle ligaments. In acute cases, the detailed history should include reconstruction of the trauma mechanism. The presence of associated conditions such as rheumatoid arthritis, psoriasis, hyperparathyroidism, diabetic neuropathy, calcaneal fracture, fluoroquinolone use, and local steroid injections is important, because they can increase the degree of peroneal tendon dysfunction.16 The differential diagnosis includes fatigue fractures or fractures of the fibula, posterior impingement of the ankle, and lesions of the lateral ligament complex. Post-traumatic or postoperative adhesions and irregularities of the posterior aspect of the fibula (i.e., peroneal groove) also can be responsible for symptoms in this region.
Patients with peroneal tendon dislocation typically complain of lateral instability, giving way, and sometimes a popping or snapping sensation over the lateral aspect of their ankle. On physical examination, the tendons can be subluxated by active dorsiflexion and eversion, which provokes the pain.17
Diagnostic Imaging
Peroneal tendon dislocation is a clinical diagnosis, and it is frequently accompanied by a tendon rupture. Additional investigations such as magnetic resonance imaging (MRI) and ultrasonography may be helpful in diagnosing partial tears of the tendon of peroneus brevis or longus.18 Both modalities are considerably accurate and precise, although ultrasonography is more cost effective.19
Treatment
Conservative Management
Conservative management should be attempted first. This includes activity modification, footwear changes, temporary immobilization, and corticosteroid injections. Lateral heel wedges can take the strain off the peroneal tendons, which may allow healing.16
Surgical Technique
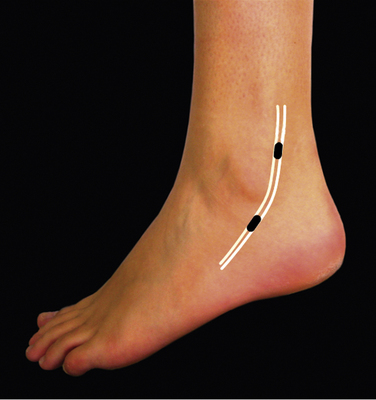
The patient is placed in the lateral decubitus position. Alternatively, the patient can be placed in the supine position with the foot in endorotation. A support can be placed under the leg, allowing the ankle to be moved freely. Before anesthesia is administered, the patient is asked to evert the foot so that the peroneal tendons can be visualized clearly. Their course is drawn on the skin, and the locations of the portals are marked (Fig. 16-1). The surgery can be performed under local, regional, epidural, or general anesthesia. After exsanguination, a tourniquet is inflated around the thigh of the affected leg.
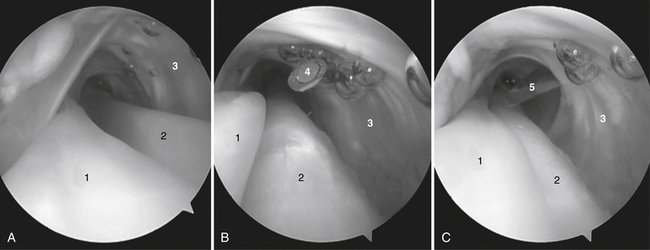
The inspection starts approximately 6 cm proximal to the posterior tip of the fibula, where a thin membrane splits the tendon compartment into two separate tendon chambers. More distally, the tendons lie in one compartment. A second portal is made 2 to 2.5 cm proximal to the posterior edge of the lateral malleolus under direct vision by placing a spinal needle directly over the tendons (Fig. 16-2). Through the distal portal, a complete overview of both tendons can be obtained.
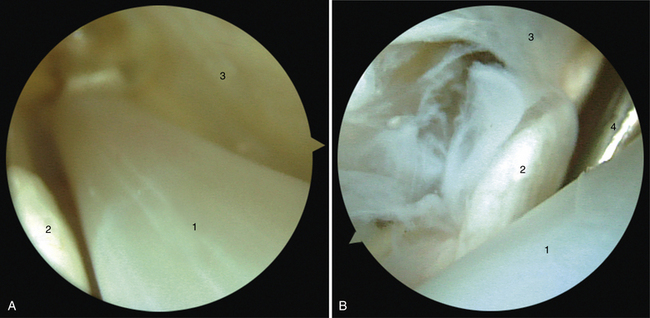
By rotating the arthroscope over and between both tendons, the entire compartment can be inspected (Fig. 16-3). When a total synovectomy of the tendon sheath has to be performed, it is advisable to make a third portal more distal or more proximal than the portals described previously. When a rupture of one of the tendons is seen, endoscopic synovectomy is performed, and the rupture is repaired through a mini-open approach.
In patients with recurrent dislocation of the peroneal tendon, endoscopic fibular groove deepening can be performed through this tendoscopic approach. It is a time-consuming procedure because of the limited working area. Groove deepening is performed from within the tendon sheath, with the risk of iatrogenic damage to the tendons. We therefore prefer an approach based on the two-portal hindfoot technique, with an additional portal located 4 cm proximal to the posterolateral portal.20
PEARLS& PITFALLS
PEARLS
PITFALLS
TENDOSCOPY OF THE POSTERIOR TIBIAL TENDON
These disorders can be divided in two groups: the younger group of patients, who had dysfunction of the tendon caused by some form of systemic inflammatory disease (e.g., rheumatoid arthritis), and an older group of patients, whose tendon dysfunction is mostly caused by chronic overuse.21 After trauma, surgery, and fractures, adhesions and irregularity of the posterior aspect of the tibia can be responsible for symptoms in this region.
A dysfunctional posterior tibial tendon usually evolves to painful tenosynovitis. Tenosynovitis is also a common extra-articular manifestation of rheumatoid arthritis, in which hindfoot problems are a significant cause of disability. Tenosynovitis in rheumatoid patients eventually leads to a ruptured tendon.22
Anatomy
The posterior tibial muscle arises from the interosseous membrane and the proximal adjacent surfaces of the tibia and fibula, and it is part of the deep posterior compartment of the calf. The tendon forms in the distal third of the calf and passes behind the medial malleolus, where it changes direction.23 The posterior tibial tendon is the most superficial structure coursing directly behind the medial malleolus.
Pain complaints are often localized in the relative hypovascular zone immediately distal to the medial malleolus, beginning 4 cm proximal to the insertion of the tendon.24 This hypovascular zone may contribute to the development of degenerative changes and consequently to ruptures.25
The posterior tibial tendon is held in the retromalleolar groove by a strong fibro-osseous tunnel and the flexor retinaculum originating from the tip of the medial malleolus and inserting into the calcaneus. Distally, the retinaculum blends with the sheath of the tendon and the superficial deltoid ligament.23 The anterior, major slip of the tendon inserts primarily into the tuberosity of the navicular, the inferior capsule of the medial naviculocuneiform joint, and the inferior surface of the medial cuneiform. A second slip extends to the plantar surfaces of the cuneiforms and the bases of the second, third, and fourth metatarsals.23
A tendon sheath surrounds the posterior tibial tendon, and both structures are connected by a vincula, which carries part of the blood supply to the tendon. A vincula can become symptomatic when damaged, causing thickening, shortening, and scarring of the distal free edge. In these patients, a painful local thickening can be palpated posterior and just proximal to the tip of the medial malleolus.25
Patient Evaluation
History and Physical Examination
In the early stage of dysfunction, patients complain of persistent ankle pain medially along the course of the tendon, fatigue, and aching on the medial plantar aspect of the ankle. Tenosynovitis commonly is associated with swelling.23,25 A typical observation is abnormal wear of the medial sides of the shoes. Walking increases pain, and participation in sports activities becomes difficult.
Careful clinical examination is important, and both feet should be examined. Valgus angulation of the hindfoot is frequently seen with accompanying abduction of the forefoot (i.e., too many toes sign).23
Related posts:
 Soft Tissue Impingement of the Ankle Joint
Osteochondral Lesions of the Talar Dome: Anatomy, Etiology, and Evaluation
Instrumentation and Operative Setup for Ankle and Subtalar Arthroscopy
Anatomy, Evaluation, and Operative Setup for Posterior Ankle Arthroscopy
Fusion for Degenerative Arthritis of the Ankle
Diagnostic Arthroscopy for the Ankle and Subtalar Joints
Soft Tissue Impingement of the Ankle Joint
Osteochondral Lesions of the Talar Dome: Anatomy, Etiology, and Evaluation
Instrumentation and Operative Setup for Ankle and Subtalar Arthroscopy
Anatomy, Evaluation, and Operative Setup for Posterior Ankle Arthroscopy
Fusion for Degenerative Arthritis of the Ankle
Diagnostic Arthroscopy for the Ankle and Subtalar Joints
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


