Instrument Adjusting
Kirk Eriksen
Learning Objectives
After studying this chapter, the reader should be able to:
Develop an understanding of the development and function of different types of upper cervical adjusting instruments.
Establish the coordinates for the Adjustment vector.
Understand the importance of Atlas transverse process contact and how to establish accurate instrument placement.
Line up the handheld and Table-mounted instruments on the Adjustment coordinates.
Express how preload is used and varied for different alignment patterns.
Vary the speed and number of Thrusts for various Subluxation patterns.
Know when to use Torque and how to set it with the Table-mounted instrument.
Understand the amount of force used with various types of Adjustments.
Orthospinology teaches doctors the use of a handheld and a table-mounted adjusting instrument. Various handheld solenoid-powered instruments have been produced over the years from the original research of Dr. Cecil Laney. In the late 1990s, Laney designed the Torque-specific Table-mounted instrument, which uses a multivector force that aids in reducing the atlantoaxial rotatory Subluxation. A moving stylus creates an accelerating force with a specially designed cam inside the adjusting head of the instrument. The force starts slowly and gains speed as it reaches its peak at the end of the Thrust. This differs from the solenoid impulse force of the Handheld instrument.
This chapter will demonstrate the proper use of these instruments to help the doctor achieve effective and safe clinical outcomes. The Orthospinology Adjustment is the culmination of the precision of the X-ray equipment alignment, the accuracy of the X-ray setup and analysis, attention to detail of patient placement on the side posture, the use of Mastoid support adjusting table, and the use of the proper line of correction. With the Adjustment goes a tremendous responsibility to be as accurate and careful as possible, because the Adjustment is a somewhat invasive procedure intended to alter vertebral alignment and positively affect the central nervous system. The Orthospinology philosophy holds that any attempt to change the function of the nervous system must be undertaken with great care and planning. A favorable outcome should be predictable with a high degree of probability. This concept has been continually reinforced since the inception of the Grostic seminars in the 1940s with the following statement related to patient care: “How wonderful the opportunity, how great the responsibility.”
History of Upper Cervical Instrument Adjusting
Dr. Arden Zimmerman’s Contributions
In 1930, Dr. B. J. Palmer announced to the profession that he had further refined chiropractic and introduced the controversial HIO (hole-in-one) technique (see Chapter 1).1 Palmer’s research clinic took care of the worst-of-the worst cases from North America and around the world with great success in most cases. One such patient was Arden Zimmerman. He traveled from California to
Davenport, Iowa, and was unloaded from the train by stretcher and transported to the clinic in one of B. J.’s chiropractic ambulances. Over the previous few years, Zimmerman’s Health had rapidly deteriorated to the point that he weighed only 110 pounds and was hardly able to walk. Palmer performed 22 upper cervical Adjustments between the day Zimmerman arrived on February 11, 1937, until May 1939. Zimmerman experienced immediate and sustained improvements in his Health from Palmer’s care. He noticed that when he was “in Adjustment,” he had much improvement and when “out of Adjustment,” he became sick rather rapidly. This observation would later shape his philosophy that each patient, barring later trauma, should only have one Subluxation and need one Adjustment. Zimmerman was disappointed that 22 Adjustments were necessary in his case, even though his Health was significantly improved. However, he thought that if it were done correctly the first time, the other 21 Adjustments would not have been necessary.2
Davenport, Iowa, and was unloaded from the train by stretcher and transported to the clinic in one of B. J.’s chiropractic ambulances. Over the previous few years, Zimmerman’s Health had rapidly deteriorated to the point that he weighed only 110 pounds and was hardly able to walk. Palmer performed 22 upper cervical Adjustments between the day Zimmerman arrived on February 11, 1937, until May 1939. Zimmerman experienced immediate and sustained improvements in his Health from Palmer’s care. He noticed that when he was “in Adjustment,” he had much improvement and when “out of Adjustment,” he became sick rather rapidly. This observation would later shape his philosophy that each patient, barring later trauma, should only have one Subluxation and need one Adjustment. Zimmerman was disappointed that 22 Adjustments were necessary in his case, even though his Health was significantly improved. However, he thought that if it were done correctly the first time, the other 21 Adjustments would not have been necessary.2
His personal experience motivated Zimmerman to enter Palmer School of Chiropractic to become a chiropractor. While in private practice, he developed a large, floor-mounted machine that was named the Specific adjusting machine (SAM). He used the best electrical and mechanical engineering technology available at the time to create this 250-pound machine that delivered a Thrust using an electrically controlled Adjustment. The SAM instrument delivered a Thrust in an average time of
 second with an average depth of 5/8 inch.3 Typically, 105 pounds per square inch of force was used to adjust the patient. The first instrument included a recoil action in an attempt to duplicate the hand-delivered Thrust. The first SAM Adjustment was performed in 1948 to a patient suffering from asthma, who reported good results. Zimmerman suggested that patients return every 13 months to be checked to ensure they remained free of Subluxation. By the time of his retirement, it was reported that he had more than 58,000 patient files.3
second with an average depth of 5/8 inch.3 Typically, 105 pounds per square inch of force was used to adjust the patient. The first instrument included a recoil action in an attempt to duplicate the hand-delivered Thrust. The first SAM Adjustment was performed in 1948 to a patient suffering from asthma, who reported good results. Zimmerman suggested that patients return every 13 months to be checked to ensure they remained free of Subluxation. By the time of his retirement, it was reported that he had more than 58,000 patient files.3
Dr. Cecil Laney’s Contributions
Dr. Cecil Laney began taking classes in 1951 for what later became known as the Grostic procedure. He has been known as one of the most influential supporters of Grostic’s Work to this day. In 1954, he began developing adjusting instruments that attempted to duplicate the corrections made by hand. Laney said that the biggest mistake he made in the early days was using too much force, and this tended to lock up the Articulations and prevent any osseous movement. Likewise, the original Grostic hand Adjustment evolved from its original Palmer-type toggle to use a lighter, more controlled force.
The first practical instrument Dr. Laney built in the early 1960s was called the Grasshopper (Fig. 14-1). This was an instrument that moved around the arc of the head of the table, and the doctor adjusted down the line of drive. The instrument was a percussion device that required the doctor to strike a spring-loaded plunger to create stylus excursion. Laney moved from the Grasshopper to the creation of a Handheld instrument. The first instrument was a spring-operated device; he later developed an electric-powered Handheld instrument with a solenoid that would emit an adjustive force. A solenoid converts electricity into a mechanical impulse. The electricity magnetizes the coil, which moves the core forward. The core is attached to the stylus of the instrument, which can be set to move from 0 to ¼ inch during the Adjustment. However, in clinical practice, the instrument is typically set to about
 inch or less. Laney created the “single-axis” method to use these devices, which consists of using a formula that figures in the Height factor and the rotation into a number of degrees from the vertical (see Table of Resultant angles).
inch or less. Laney created the “single-axis” method to use these devices, which consists of using a formula that figures in the Height factor and the rotation into a number of degrees from the vertical (see Table of Resultant angles).
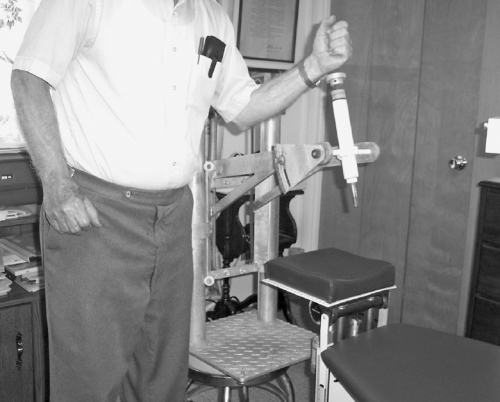 FIGURE 14-1 The Grasshopper, one of the first adjusting instruments developed by Dr. Cecil Laney. |
The Laney Instrument
The first Handheld instruments were known simply as the Laney instrument. Laney had these instruments produced and sold at his cost to enable as many chiropractors to obtain them as possible. In the 1980s, a new version of this instrument was produced by Richard King and was called the KH-4 instrument. He later produced the KH-5 instrument in the late 1990s, and all of these instruments are still used with impressive clinical effectiveness (Fig. 14-2). Incidentally, Dr. J. K. Humber, in 1967, was one of the first to adapt the dental hammer to an upper cervical adjusting instrument.4 Dr. Warren Lee and Dr. Arlen Fuhr modified the basic
design of the dental hammer and later produced the Activator instrument.5
design of the dental hammer and later produced the Activator instrument.5
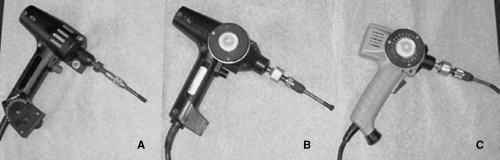 FIGURE 14-2 Orthospinology handheld, solenoid-powered instruments. A: Laney instrument. B: KH-4 instrument. C: KH-5 instrument. |
The Handheld instruments did not have the benefit of Torque, and the corrections were not as consistent in correcting the atlantoaxial misalignment. Laney spent 10 years observing the Adjustments of thousands of patients, and it appeared that Leverage was the key to moving the axis spinous process. In other words, more height used with the adjusting vector tended to reduce inferior spinous misalignments, and less height reduced the superior spinous misalignments. It was surmised that the hand Torque reduced inferior spinous by creating more Leverage; therefore, the addition of up to 10° on the Handheld instrument for opposite angles with large ipsilateral C2 spinous process misalignments was used. Laney also observed that it required less Leverage to correct contralateral (superior) axis spinous misalignments. However, these modifications did not completely solve the problem, so a Table-mounted instrument was developed in the mid- to late 1960s (Fig. 14-3). The Table-mounted instrument was first built with the Torque functioning where the stylist rotated. Laney was able to create either clockwise or counterclockwise rotation with any amount in between, or not at all. However, clinical research on countless patients demonstrated that the turning of the stylus did nothing for improving the C2 spinous process misalignments. It was also during this period that it was determined clinically that using more than 3/8 inch of stylus excursion was ineffective.
Dr. Laney experimented by going back to the original Grostic procedure line-of-correction vector, although the corrections diminished somewhat, and he realized that he was not getting extra Leverage with the turning of the stylist. One of the main goals of the Adjustment is to simultaneously reduce the lateral and rotatory atlanto-occipital and atlantoaxial misalignments by directing force into the atlas transverse process (ATP), therefore using the vertebra as a Lever. With the use of a straight stylus, the Resultant angle cannot be set more than 30° without losing contact with the ATP in most cases, because the patient’s skull will block the instrument’s placement. This limits the amount of Leverage that can be obtained without using a Bent stylus (see Fig. 19-2). For the Torque to Work, it must be coordinated with the Thrust and completed at the end of the Adjustment. Torque attempts to create an additional downward or upward increase in the Leverage factor of the vectored force to assist in correcting the lateral and rotatory atlantoaxial misalignments. The process creates a rectilinear and angular force in one operation—in other words, a multivector force.
 FIGURE 14-3 Dr. Cecil Laney’s first table-mounted adjusting instrument. |
Torque
It has been proposed that hand Adjustment Torque Works by spiraling the arms during the contraction of the long head of the triceps, which approximates the elbows and results in a slight amount of lateral movement of the doctor’s pisiform in either a cephalad or caudal direction, depending on the type of Torque. If the Torque is preset,
simply relaxing the muscles that maintain the preset Torque will allow the arms to rotate or unwind during the Adjustment. The pisiform and handset arch are kept in the same position during the Thrust, but the resulting force from the Torque will be transferred to the ATP toward the end of the Adjustment (see Chapter 13).
simply relaxing the muscles that maintain the preset Torque will allow the arms to rotate or unwind during the Adjustment. The pisiform and handset arch are kept in the same position during the Thrust, but the resulting force from the Torque will be transferred to the ATP toward the end of the Adjustment (see Chapter 13).
However, the mechanism of action related to Torque used in the hand Adjustment is a bit of a contentious issue, with varying opinions. It has to do with the coordination of the doctor’s arms as they unwind throughout the Thrust and whether the doctor keeps the pisiform somewhat stationary throughout the completion of the Adjustment. This can alter the direction of the Torque-induced force at the end of the Adjustment. Indeed, clinical evidence from more than 60 years of Grostic-based care has shown promising results with this method, although rigorous research is necessary to determine the exact mechanism and effectiveness of Torque used in the Adjustment. Regardless of the explanation, Torque does not Work by causing the pisiform to spin against the skin. It is incorrect to characterize the term Torque, as used in the Orthospinology Adjustment, as a revolving force.
Dr. John D. Grostic described the effect of Torque a bit differently than Laney. They both agreed that Torque results in a change in the line of correction at the very bottom of the Thrust. However, they differed on the direction of the force (related to inferior and superior Torque) and the mechanism of the actual correction of the axis spinous process misalignment. Grostic felt that this movement at the end of the Adjustment actually caused a type of unilateral traction maneuver that caused the capsular ligaments (or other structures) to pull the axis spinous process around into improved alignment. The raising or lowering of the headpiece helps by slightly opening either the superior or inferior atlantoaxial Articulation (with the patient in the side-lying position), and the Torque is supposed to open the joint a little further. This proposed traction mechanism may help to explain how medical traction can reduce Atlantoaxial rotatory fixations/Subluxations as evidenced with pre- and postradiography.6,7,8,9,10,11,12,13,14,15
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


