Table Placement
Roderic P. Rochester
Learning Objectives
After studying this chapter, the reader should be able to:
List the concepts that determine appropriate patient placement on the adjusting table.
Describe the general patient placement on the table for the Adjustment.
Explain the proper placement of the mastoid on the Mastoid support.
Determine the appropriate head placement on the headpiece for Handheld instrument, Table-mounted instrument, and Hand adjusting.
Explicate the importance of a Mastoid support without parietal support and how the headpiece is constructed to assist in achieving this goal.
Demonstrate the difference in patient placement and headpiece angle based on skull morphology.
Express the difference in patient placement and headpiece angle based on the four types of misalignment patterns.
Position the headpiece height for an inferior or superior axis spinous.
Determine the proper lower shoulder placement to aid in Instrument adjusting.
The importance of the placement of the patient on the adjusting table is often overlooked as a major factor in the successful Orthospinology Adjustment. If 100% reduction of the misalignment occurs following an Adjustment, it is thought that 40% is due to Table placement. Generally, Table placement is the same for instrument or Hand adjusting. The hand Adjustment uses Torque during the Adjustment as an advantage that is not possible with the Handheld instrument Adjustment; however, the table-mounted Laney instrument is able to reproduce Torque similar to that of the hand Adjustment. Small variations in the patient’s Table placement can assist the doctor, depending on the chosen adjusting method. The Table placement is accomplished by getting the patient into the general position, supporting the mastoid appropriately, raising or lowering the headpiece, and modifying the headpiece angle to the required settings. The proper elevation of the headpiece is valuable in the correction of axis spinous deviations for all methods of delivering the adjusting force. Table placements are based on rigorous biomechanical concepts, reduction of variables, and steps to improve Reliability and Validity.
General Placement of the Patient
The Orthospinology Adjustment is performed with the patient in the side posture position with the Atlas laterality side upward. Before positioning the patient, change the headpiece angle from the Supine leg check position by elevating the headpiece a few inches to accommodate the patient’s shoulder, then reducing the more cephalic or upper portion of the headpiece. This will help ensure that the patient’s head does not rotate into the direction of Atlas laterality as they initially lay down on the table on their side. The patient is instructed to sit on the table facing the appropriate direction and distance from the headpiece to allow him/her to lie on his/her side so that the mastoid settles on the Mastoid support. The doctor stands behind the patient and places the appropriate hand over the patient’s mastoid and neck to help guide the patient down to the side-lying position with the mastoid on the Mastoid support. The patient may be a little nervous for the first Adjustment and will tend to straighten the knees after lying on their side. To add stability and relaxation, ask the patient to bend the knees slightly and stack the feet on each other
on the table. The ankles, hips, shoulders, and external auditory meatus should form roughly a straight line. The patient’s shoulders should be approximately vertical, but the lower shoulder can be slightly anterior to allow the weight to rest on the posterolateral aspect of the shoulder. This is more comfortable for most people.
on the table. The ankles, hips, shoulders, and external auditory meatus should form roughly a straight line. The patient’s shoulders should be approximately vertical, but the lower shoulder can be slightly anterior to allow the weight to rest on the posterolateral aspect of the shoulder. This is more comfortable for most people.
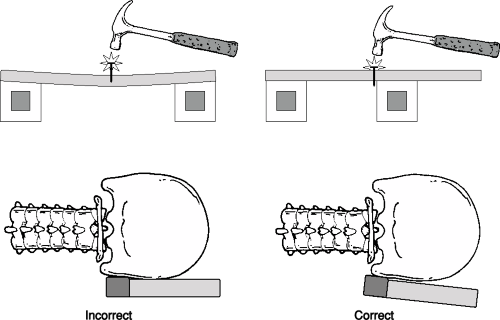 FIGURE 12-1 Easily driving a nail into a board near its support demonstrates the concept of how a solid Mastoid support in close proximity to the occipitoatlantal joint creates a significant mechanical advantage with minimal Adjustment force dissipation. |
Positioning the Patient’s Head on the Headpiece
The Orthospinology procedure is based on the Grostic model of the upper cervical Subluxation complex and is composed of many concepts (see Chapters 8 and 16). The Adjustment and patient placement are based on the physics of misalignment, the X-ray analysis, adjusting method, and patient’s skull morphology. Changing or omitting any of the steps may seriously affect the outcome. Placing the skull on the headpiece properly is essential for the correction of misalignment in the upper cervical spine, and improper placement can result in poor reductions or even increasing the misalignment.
The headpiece contains a Mastoid support that is 2 inches long located the length of the caudal or lower edge of the headpiece. The patient’s mastoid is placed about 1/4 inch cephalad to the lower edge of the Mastoid support, not to exceed 3/4 inch. The headpiece is capable of elevating or lowering independently at the top, bottom, or simultaneously. To eliminate parietal support, the superior portion of the headpiece is lowered or tipped down at the top. The angulation of the headpiece will be determined by how round or elongated the skull and the type of misalignment that is to be corrected. A solid Mastoid support is essential for the desired biomechanical results based on the radiographic measurements. Any parietal support alters the physics that are predicted based on these measurements. Parietal support decreases the Reliability and predictive Validity of the procedure and is not advised (Fig. 12-1).
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


