Imaging of the Acetabular Labrum
Fiona Carty
Adam C. Zoga
William B. Morrison
Introduction
Hip magnetic resonance (MR) arthrography has a high accuracy in the detection of labral tears (1,2,3) and is the imaging modality of choice in patients in whom there is a strong suspicion of labral lesions. Abnormalities of the acetabular labrum include partial tears, complete tears, and labral detachment, with detachments being more common than tears (4,5). There are reports of the successful assessment of the labrum without joint distention (6), however in a study by Czerny et al. the sensitivity and accuracy of MRI for nondistended joints were 30% and 36%, respectively, when compared with surgical findings. Sensitivity and accuracy of MRI increased to 90% and 91%, respectively, after joint distention with gadolinium contrast (7).
In a small group of eight patients, Sundberg et al. showed MR arthrography at 1.5 T and conventional MRI at 3 T, both identified seven out of eight labral tears. In one patient in whom the interpretations from the two examinations disagreed, the labrum demonstrated a marked increase in intrasubstance signal intensity indicative of a tear at 3 T MR imaging, whereas a normal labrum was shown at 1.5 T MR arthrography. At arthroscopy, the labrum was found to be torn (8).
Anatomy
The acetabular labrum is a fibrocartilaginous structure which rims the acetabulum anteriorly, superiorly, and posteriorly, and which evolves into the fibrous transverse ligament inferiorly (9). The labrum may be separated from the transverse ligament by a defect that is filled with articular cartilage. This defect may be confused with a tear on MR and MR arthrographic images (10). The labrum serves to deepen the acetabulum; however, its role in maintaining stability is probably less critical than that of the glenoid labrum. On MR arthrography, the normal labrum is triangular in appearance with sharply defined margins. The labrum is thinnest anteroinferiorly and thickest posterosuperiorly and is typically low signal intensity on all imaging sequences. The capsule of the hip joint inserts directly at the base of the labrum anteriorly and posteriorly and superiorly, the capsule inserts several millimeters above the labral attachment. Inferiorly, the capsule blends with the transverse ligament (11) (Fig. 15.1).
MR Arthrography Technique
MR arthrography of the hip is performed as a two-stage procedure. The first step is performed under fluoroscopic guidance. The preferred approach for hip arthrography is a direct anterior approach, targeting the lateral femoral neck or the lateral femoral head (Fig. 15.2). The intra-articular needle position is confirmed by injection of iodinated contrast material. Joint distention is achieved by injection of a dilute solution of gadolinium (12). The standard dilution of gadolinium for joint distention is 2.5 mm of gadopentetate dimeglumine (9). For a single hip this dilution may be achieved by mixing 0.1 mL of gadopentetate dimeglumine in 20 mL of normal saline, however, different gadolinium products may contain different gadolinium concentrations. The joint capacity is 8 to 20 mL. Intra-articular lidocaine injection also may be useful. Pain relief with intra-articular lidocaine further supports an intra-articular source. Failure to produce pain relief, however, does not exclude an intra-articular source. With the use of intra-articular gadolinium, axial, coronal, and sagittal T1-weighted fat suppressed images are acquired through the hip joint using a surface coil and field of view of 14 to 16 cm. It is important to use at least three imaging planes to ensure that all portions of the labrum are adequately assessed. An assessment of the entire pelvis is performed with T1 and short tau inversion recovery (STIR) coronal images that include the symphysis pubis and the sacrum, increasing the field of view to 36 to 40 cm.
Anatomical Variants
One pitfall in the interpretation of MR arthrography of the hip is the question about the presence of a normal sulcus or recess at the anterosuperior aspect of the joint. To date, no conclusive data are available about whether such a sulcus may exist normally. The perilabral recesses are located at the labrocapsular junction on the capsular surface of the labrum. A sulcus created by the junction of the transverse ligament and the labrum is also a normal finding (Fig. 15.3). This sulcus should be known as the labroligamentous sulcus.
Another sulcus is located at the posteroinferior aspect of the joint, and it represents a physiologic cleft at the junction of the articular cartilage. The cleft may be partial or complete. Histologic studies have concluded that the articular cartilage and the labrum blend together seamlessly, which suggests that a separation between the articular cartilage and labrum would be abnormal (2,13,14). Cashin et al. studied the prenatal development of the human acetabular labral–chondral complex in 11 fetal hips, aged from 8 weeks of gestation to term. Morphologically, the anterior acetabular labral–chondral complex had a somewhat marginal attachment to the acetabular cartilage and seemed to cap its anterior part. There was an intra-articular labral projection which formed a recess between the articular surface of the acetabulum and the labrum. The posterior labrum differed in that it was directly attached to and continuous with the acetabular cartilage. It lacked a labral projection into the articular space. Under higher magnification, the attachment site of the labrum to the acetabulum anteriorly demonstrated a sharp, abrupt transition at the junction of the cartilaginous acetabulum and the labrum. Anteriorly, the collagen fibers at the junction of the acetabular cartilage ran parallel to the labral–cartilage junction, but posteriorly they were perpendicular to this junction when examined under polarized light (15).
Another sulcus is located at the posteroinferior aspect of the joint, and it represents a physiologic cleft at the junction of the articular cartilage. The cleft may be partial or complete. Histologic studies have concluded that the articular cartilage and the labrum blend together seamlessly, which suggests that a separation between the articular cartilage and labrum would be abnormal (2,13,14). Cashin et al. studied the prenatal development of the human acetabular labral–chondral complex in 11 fetal hips, aged from 8 weeks of gestation to term. Morphologically, the anterior acetabular labral–chondral complex had a somewhat marginal attachment to the acetabular cartilage and seemed to cap its anterior part. There was an intra-articular labral projection which formed a recess between the articular surface of the acetabulum and the labrum. The posterior labrum differed in that it was directly attached to and continuous with the acetabular cartilage. It lacked a labral projection into the articular space. Under higher magnification, the attachment site of the labrum to the acetabulum anteriorly demonstrated a sharp, abrupt transition at the junction of the cartilaginous acetabulum and the labrum. Anteriorly, the collagen fibers at the junction of the acetabular cartilage ran parallel to the labral–cartilage junction, but posteriorly they were perpendicular to this junction when examined under polarized light (15).
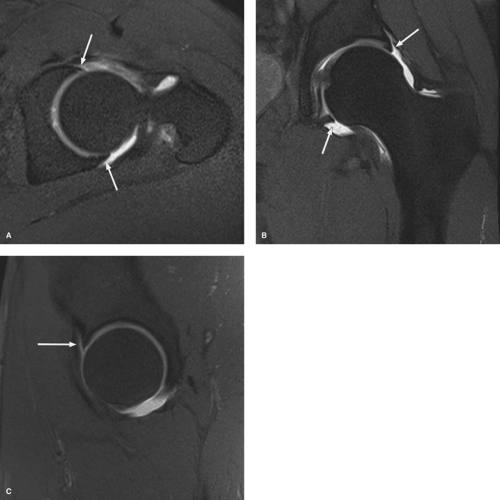 Figure 15.1. Axial (A), coronal (B), and sagittal (C) MR arthrogram of the left hip showing a normal triangular appearance to the anterior and posterior labrum (white arrows). |
 Figure 15.2. Arthrogram of the right hip showing needle tip placement along the lateral aspect of the femoral neck (arrow). |
Hodler et al. (2) examined 12 cadaver hips from elderly individuals to make their observations. The conclusions of Seldes et al. (13) and Tan et al. (14) are drawn from studies of 67 cadaveric specimens. Seldes and Tan, however, report tears at the anterosuperior margin in 74% of hips, and 89% of these tears were detachments. In their study, few normal anterosuperior labral margins were examined. The average age of their specimens was 78 years. The finding is of significance in the younger population but not the older population. In their study of six cadaveric hips (age range: 72 to 84 years), Czerny et al. (16) did not identify any sublabral sulci. Dinauer et al. (17) and Petersilge et al. (3) in their studies of 23 and 24 hips, respectively, were unable to confirm the presence of a sulcus at the anterosuperior portion of joint. In an arthroscopic study of 56 hips, Fitzgerald (5) found 41 tears with separation of the articular cartilage and labrum. Most tears were in the anterior aspect of the hip. Based on visual inspection, they reported that evidence of attempted healing of the defect was usually seen but a residual sulcus could be identified. The sulcus measured 2 to 5 mm in width and 8 to 20 mm in length, which would suggest that the sulcus is abnormal. The literature suggests that a normal cleft is located between the margin of the articular cartilage and the labrum and that this normal variant has an incidence of 5% to 6%. The margins of the cartilage edge and the border of the labrum are sharp. In contrast, any extension of contrast into the acetabular (osseous) labrum junction should be considered abnormal. Any irregularity of the margins of the cartilage edge or the adjacent labrum would indicate that the separation between labrum and cartilage is abnormal.
A defect in the capsule between the pubofemoral and iliofemoral ligaments may lead to communication between the joint and the iliopsoas bursa, and contrast may occasionally fill this structure (3). The bursa should not be confused with an extra-articular cyst or ganglion. The bursa typically lies lateral to the iliopsoas tendon, whereas extra-articular cysts are medial and usually adjacent to the acetabulum (18).
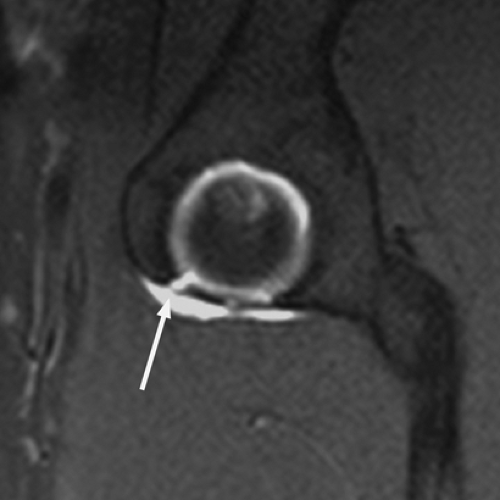 Figure 15.3. Sagittal MR arthrogram of the hip showing an anterior paralabral recess (arrow) at the transverse ligament attachment. |
Diagnostic Criteria
The majority of acetabular labral tears reported in the MR arthrography and arthroscopy literature have occurred in the anterior or anterosuperior portion of the labrum (1,3). Isolated posterior labral tears are seen most frequently after a posterior hip dislocation or with dysplasia but are not commonly seen in other populations having hip arthroscopy. Lateral labral tears are encountered infrequently in arthroscopic evaluation. When lateral tears occur, they invariably are associated with additional labral and acetabular lesions (19). Leuing et al. (20) found in femoroacetabular impingement only undersurface tears were seen, whereas there was labral degeneration and volume increase in patients with dysplasia, although transitions from undersurface tears to complete avulsions from the acetabular rim were seen suggesting decompensation of the disease process.
Criteria for identification of torn labra at MR arthrography include labra with intrasubstance contrast material, and labra with irregular margins with and without labral detachment. Labral detachment is identified by contrast material interposed at the acetabular–labral interface with or without displacement of the labrum (1




Related posts:






Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
