Chapter 117 Imageless Computer Navigation in Total Knee Arthroplasty
The Simpler Wave of the Future
The use of computer-based systems during total knee arthroplasty (TKA) has become more readily accepted during recent years. Computer-assisted surgery for total knee replacement was first approved for use in the United States in 2001. Since its introduction, this technology has expanded rapidly, and several different types of navigation systems have been developed by several different manufacturers. Each new version of the software has incorporated increasingly sophisticated analysis modules to allow not only accurate alignment of the limb and component position but also assessment of ligament balance and knee kinematics.45 An increasing number of references in the orthopedic literature are reporting on computer-assisted techniques and early outcomes with these techniques.* Each system affords surgeons the opportunity to maximize clinical outcomes by perfecting the surgical technique. Specifically, component alignment during the procedure must be optimized.20,21,31
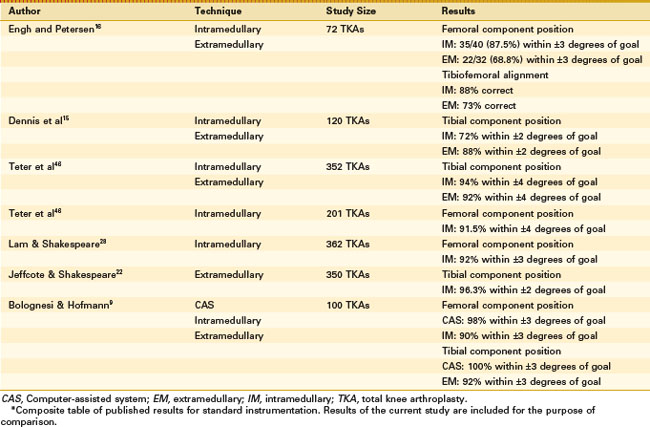
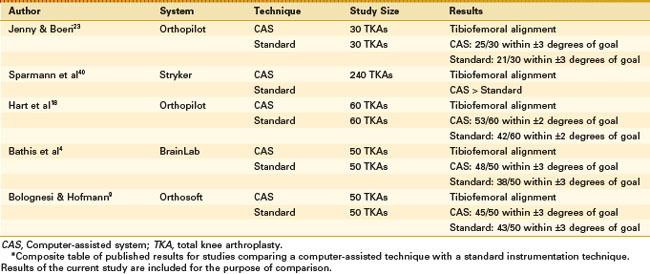
The significance of component and limb alignment has been extensively studied since the earliest days of TKA. Several early references in the knee arthroplasty literature focusing on outcome and experience with TKA underscore the importance of alignment.2,29,37 Alignment errors in TKA greater than 3 degrees can be associated with poorer outcomes and accelerated failure. Rotation of the femoral and tibial components has a strong influence on patellar tracking, and malrotation of components can lead to patellofemoral complications.8 Hungerford and Krackow proposed that technical perfection of alignment and component position should be the goals for TKA.20 Insall found that most failures in TKA could be attributed to incorrect ligament balance or incorrect alignment.21 Moreland’s experience in TKA yielded similar findings and led him to state that component alignment was the most important factor influencing postoperative loosening and instability.31 The real promise with computer navigation may be its potential to help surgeons avoid outliers when using standard instruments (Fig. 117-1). Outliers represent patients who fall outside the accepted values for alignment. Conventional techniques that use extramedullary alignment guides or intramedullary rods for component orientation can result in component malalignment.15,34 The computer-assisted technique allows errors to be verified and corrected intraoperatively. Even an experienced surgeon can attain improved results (Tables 117-1 and 117-2).

Figure 117-1 Long, standing radiograph of malpositioned total knee arthroplasty components performed with standard instruments.
Numerous studies already support the use of computer-assisted systems in knee arthroplasty. In 1999, Krackow and associates published a technique that used computer assistance to determine proper mechanical axis alignment during TKA.26 Jenny and Boeri compared a navigation system with a surgeon-controlled operative technique in 60 TKAs.23 Radiographic evaluation demonstrated improved accuracy of implantation in the computer-assisted group. Bathis and colleagues showed that computer-assisted TKA gave better correction of alignment of the leg and orientation of the components than the conventional technique did.3 If implant longevity, pain relief, and function are related to the accuracy with which a TKA is performed, mechanical instrumentation does not result in a high incidence of accuracy when each step of the procedure is measured.42 Computer-assisted TKA allows more reproducible component positioning, avoids outliers in alignment errors, and assists with soft tissue balancing.
The incidence of fat embolism syndrome from instrumenting the medullary canal during cemented or cementless TKA is not negligible.25,30 Kim found that fat embolism was seen in 65 patients (65%) with a bilateral TKA and in 46 patients (46%) with a unilateral TKA.25 Comparative studies between conventional and computer-assisted surgery have been performed to look at embolism occurrence via Doppler or echocardiography studies. It has been shown using this method that computer-assisted surgery significantly decreases the occurrence of embolic events.12,24 With computer-assisted surgery, violation of the medullary canal is avoided, thereby reducing the occurrence of embolic events.
Image-Based Systems
In image-based total knee replacement, the procedure begins with preoperative planning. To create the preoperative plan, three-dimensional computer models of the patient’s femur and tibia are constructed from CT or fluoroscopic data. Once computer models of the bones have been created, planning software orients the tibial and femoral components and calculates bone resections that align the mechanical axis of the limb and produce the intended implant contact. An intraoperative system determines the position and orientation of the patient’s femur and tibia and guides placement of the cutting jigs so that resections determined in the preoperative plan can be made.14 Image-based navigation systems include the fluoroscope unit and the CT scanner. Frequent use of the fluoroscope in an operation presents a potential radiation hazard to the surgical staff and patient. A technique known as virtual fluoroscopy enhances the fluoroscope’s capability for image-guided surgery by optically tracking the position of the C-arm, the surgical instruments, and the patient. Virtuality is achieved by the overlay of surgical instruments onto one or more previously captured fluoroscopic images. A key benefit of virtual fluoroscopy is that it considerably reduces the radiation hazard.36
CT scan navigation has shown good results in surgeons’ hands. Chauhan and coworkers demonstrated that computer-assisted total knee replacement via CT navigation techniques resulted in better alignment of the femoral component and the posterior slope of the tibial component in rotation and flexion and better matching of the femoral and tibial components in rotation in a cadaver model.10 Perlick and associates implanted 100 TKAs with the computer-assisted technique (50 knees) or the conventional approach (50 knees). Accuracy of implantation was determined on postoperative long-leg coronal and lateral radiographs. A postoperative leg axis between 3 degrees varus and 3 degrees valgus was achieved in 46 patients in the group with computer-assisted implantation and in 36 patients in the control group (P = .01). A significant difference was noted in femoral component alignment in the frontal plane. Investigators concluded that the CT-based navigation system improves the accuracy of TKA, but that higher cost and time-consuming planning mean that its use will be limited to special cases.35
Robot-Assisted Surgery
Robot-assisted knee replacement was designed to improve the accuracy and precision of bone resection. Robot-assisted surgery can aid in drilling alignment holes for conventional cutting blocks to make femoral and tibial bone cuts. Robot assistance also provides the capability to machine bone surfaces for alignment or for contact areas for bone ingrowth. The earlier version of these robotic systems used industrial robots, which are not suitable or designed for use in the operating room.39 Similar to image-guided knee replacement, robot-assisted surgery has the advantage of providing preoperative imaging, modeling, and planning. The machining capability of a robot may provide a more accurate fit between prosthesis and bone, thus making the use of cement unnecessary in certain cases because of the ability to control milling heads and minimize temperature increases noted with the conventional saw technique. One mechanism being used to minimize the discomfort that surgeons feel regarding robotic surgery is robotically assisted surgery. A surgeon may template an implant using computer navigation, and the surgeon’s hand controls a burr that machines a location in the bone for it. Errant strokes with the burr at the terminal end of the robotic arm are controlled by a mechanical block (haptic feedback). Bellemans and associates described their initial results with 25 robot-assisted primary knee arthroplasties. They achieved excellent results with alignment, yet they point out that cost, the learning curve, and excessive tourniquet time (>100 minutes) are significant obstacles that remain to be overcome.6
Image-Free Navigation Systems
Image-free navigation systems use mechanical instruments that are enhanced by their integration with accurate measuring equipment. Current image-free navigation systems are predominantly using infrared or electromagnetic tracking technology (Fig. 117-2).47 Reference frames or trackers are used to locate the limb in space (Fig. 117-3). These trackers or frames can be attached to bones and to surgical instruments to track the position and orientation of each surgical tool relative to the bone. The computer workstation displays the position of the cutting blocks relative to the desired position. Once the jig is oriented properly, it is secured in position, and bone cuts are made with a standard saw.13

Figure 117-2 An imageless computer navigation system showing the computer screen and infrared camera.

Related posts:
 Cemented Total Knee Arthroplasty: The Gold Standard
Cemented Total Knee Arthroplasty: The Gold Standard
 Management of Extra-articular Deformity in Total Knee Arthroplasty With Navigation
Management of Extra-articular Deformity in Total Knee Arthroplasty With Navigation
 Computer-Assisted Navigation: Minimally Invasive Surgery for Total Knee Replacement
Computer-Assisted Navigation: Minimally Invasive Surgery for Total Knee Replacement
 Distal Realignment of the Patellofemoral Joint: Indications, Effects, Results, and Recommendations
Distal Realignment of the Patellofemoral Joint: Indications, Effects, Results, and Recommendations
 Anterior Cruciate Ligament Reconstruction With Central Quadriceps Free Tendon Graft
Anterior Cruciate Ligament Reconstruction With Central Quadriceps Free Tendon Graft
 Osteochondritis Dissecans
Osteochondritis Dissecans
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


